


 Sign Out
Sign Out



Of the most common adverse reactions, Grade ≥ 3 events were less than 5% with the exception of neutropenia, leukopenia, and diarrhoea.
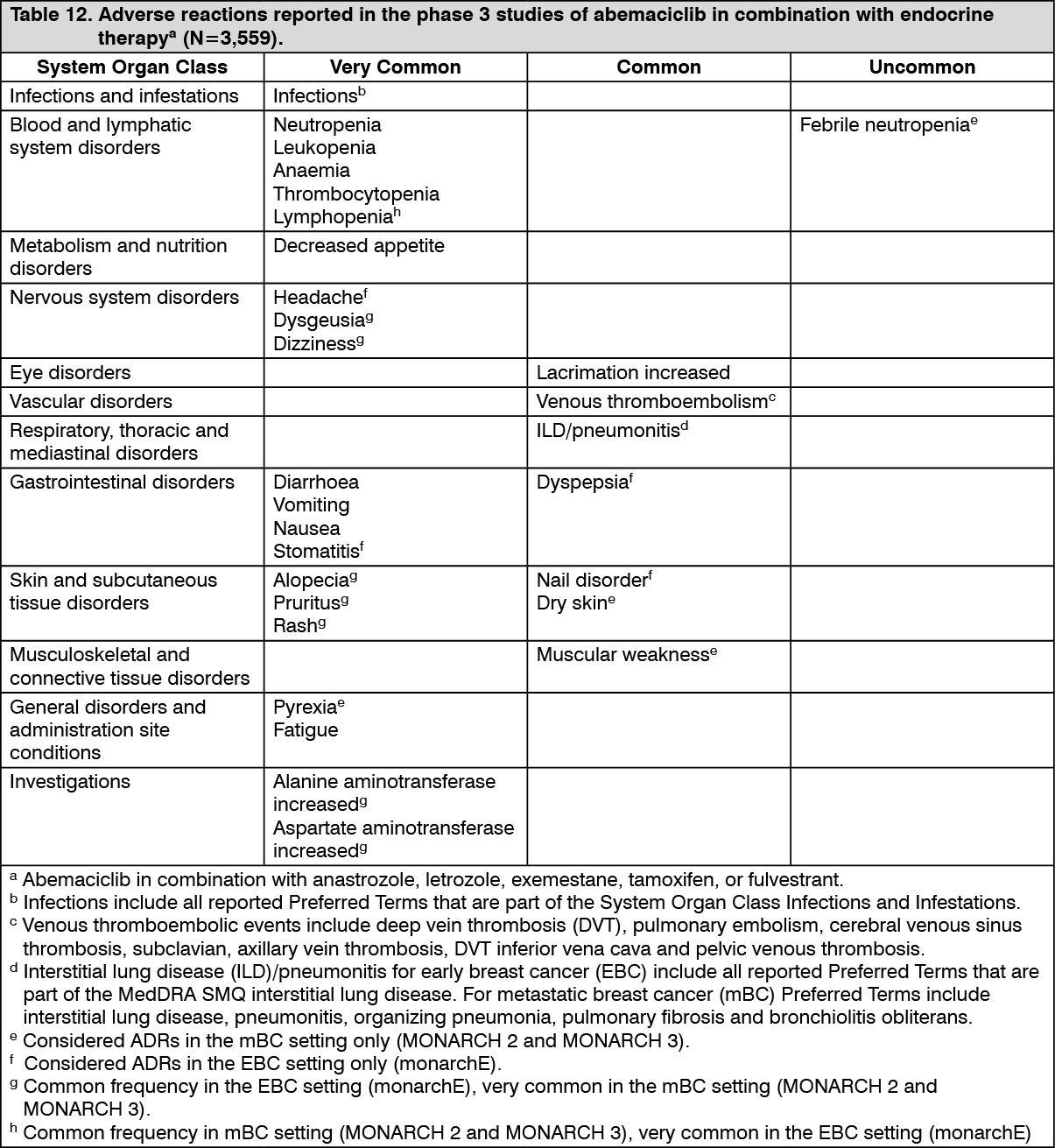
Tabulated list of adverse reactions: In the following table, adverse reactions are listed in order of MedDRA body system organ class and frequency. Frequency gradings are: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1 000 to < 1/100), rare (≥ 1/10 000 to < 1/1 000), very rare (< 1/10 000), and not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Neutropenia: Neutropenia was reported frequently across studies. In the monarchE study, neutropenia was reported in 45.8% of patients. Grade 3 or 4 decrease in neutrophil counts (based on laboratory findings) was reported in 19.1% of patients receiving abemaciclib in combination with endocrine therapy with a median time to onset of 30 days, and median time to resolution of 16 days. Febrile neutropenia was reported in 0.3% patients. In MONARCH 2 and MONARCH 3 studies, neutropenia was reported in 45.1% of patients. Grade 3 or 4 decrease in neutrophil counts (based on laboratory findings) was reported in 28.2% of patients receiving abemaciclib in combination with aromatase inhibitors or fulvestrant. The median time to onset of Grade 3 or 4 neutropenia was 29 to 33 days, and median time to resolution was 11 to 15 days. Febrile neutropenia was reported in 0.9% patients. Dose modification is recommended for patients who develop Grade 3 or 4 neutropenia (see Dosage & Administration).
Diarrhoea: Diarrhoea was the most commonly reported adverse reaction (see Table 12). Incidence was greatest during the first month of abemaciclib treatment and was lower subsequently. In the monarchE study, the median time to onset of the first diarrhoea event of any grade was 8 days. The median duration of diarrhoea was 7 days for Grade 2 and 5 days for Grade 3. In MONARCH 2 and MONARCH 3 studies, the median time to onset of the first diarrhoea event of any grade was approximately 6 to 8 days. The median duration of diarrhoea was 9 to 12 days for Grade 2 and 6 to 8 days for Grade 3. Diarrhoea returned to baseline or lesser grade with supportive treatment such as loperamide and/or dose adjustment (see Dosage & Administration).
Increased aminotransferases: In the monarchE study, ALT and AST elevations were reported frequently (12.3% and 11.8%, respectively) in patients receiving abemaciclib in combination with endocrine therapy. Grade 3 or 4 ALT or AST elevations (based on laboratory findings) were reported in 2.6% and 1.6% patients. The median time to onset of Grade 3 or 4 ALT elevation was 118 days, and median time to resolution was 14.5 days. The median time to onset of Grade 3 or 4 AST elevation was 90.5 days, and median time to resolution was 11 days. In MONARCH 2 and MONARCH 3 studies, ALT and AST elevations were reported frequently (15.1% and 14.2%, respectively) in patients receiving abemaciclib in combination with aromatase inhibitors or fulvestrant. Grade 3 or 4 ALT or AST elevations (based on laboratory findings) were reported in 6.1% and 4.2% patients. The median time to onset of Grade 3 or 4 ALT elevation was 57 to 61 days, and median time to resolution was 14 days. The median time to onset of Grade 3 or 4 AST elevation was 71 to 185 days, and median time to resolution was 13 to 15 days. Dose modification is recommended for patients who develop Grade 3 or 4 ALT or AST increase (see Dosage & Administration).
Creatinine: Although not an adverse reaction, abemaciclib has been shown to increase serum creatinine. In the monarchE study, 99.3% of patients had serum creatinine elevations (based on laboratory findings), and of these, 0.5% of patients had Grade 3 or 4 elevations. In patients receiving endocrine therapy alone, 91.0% reported an increase in serum creatinine (all laboratory grades). In MONARCH 2 and MONARCH 3 studies, 98.3% of patients had serum creatinine elevations (based on laboratory findings), and of these, 1.9% of patients had Grade 3 or 4 elevations. In patients receiving an aromatase inhibitor or fulvestrant alone, 78.4% reported an increase in serum creatinine (all laboratory grades). Abemaciclib has been shown to increase serum creatinine due to inhibition of renal tubular secretion transporters without affecting glomerular function (as measured by iohexol clearance) (see Interactions). In clinical studies, increases in serum creatinine occurred within the first month of abemaciclib dosing, remained elevated but stable through the treatment period, were reversible upon treatment discontinuation, and were not accompanied by changes in markers of renal function, such as blood urea nitrogen (BUN), cystatin C, or calculated glomerular filtration rate based on cystatin C.
Postmarketing Experience: The following adverse reactions have been identified during post-approval use of YULAREB. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Respiratory disorders: Interstitial lung disease (ILD)/pneumonitis [see Precautions].
View ADR Monitoring Form