


 Sign Out
Sign Out

 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe most frequently reported adverse reactions considered to be related to the intravitreal injection procedure rather than the dexamethasone implant, included vitreous hemorrhage and conjunctival edema. (See Table 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIntraocular Pressure in the Initial 6‐month Treatment Period of Studies 008 and 009: See Table 6.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe proportion of patients with increases from baseline IOP ≥10 mmHg in the study eye was significantly greater with OZURDEX compared to sham at days 7, 30, 60, and 90. At day 180, there were no significant differences between OZURDEX and sham as shown in Table 7. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe proportion of patients experiencing increased IOP with OZURDEX peaked at day 60 and returned to baseline levels by day 180. Elevations of IOP either did not require treatment or were managed with topical IOP‐lowering medications in the vast majority of patients. During the initial treatment period, only 0.7% (3/421) of the patients who received OZURDEX required laser or surgical procedures for management of elevated IOP in the study eye compared with 0.2% (1/423) with sham.
Systemic effects with OZURDEX would be expected to be negligible due to low systemic levels (below the lower level of quantitation). The adverse event profile for BRVO patients was generally similar to that observed for CRVO patients, and to the overall population. The overall incidence of adverse events was higher for the subgroup of patients with CRVO, which is consistent with the nature of the disease as patients with CRVO are more likely to develop ocular adverse events than patients with BRVO, even when not treated.
Clinical Studies 206207‐008 and 206207‐009 (6‐month Open‐label Extension): The clinical safety of OZURDEX was further assessed in a 6‐month open‐label (OL) extension of both phase 3 studies. Patients were eligible for re‐treatment if the BCVA was < 84 letters or retinal thickness was > 250 μm in the central 1 mm macular subfield and the investigator considered that the procedure would not put the patient at significant risk. The re‐treated population consisted of patients who received OZURDEX, or sham as their first injection, completed the initial treatment period at day 180, and then received OZURDEX as their second injection. A total of 997 patients received the OZURDEX injection in the open‐label phase of both studies.
For those events reported at a rate of ≥ 1%, the types of events and their incidence following the second injection were similar to those seen following the first injection with the exception of subcapsular cataract which were higher in patients who had received OZURDEX as their first injection followed by OZURDEX as the second injection. More specifically, subcapsular cataracts in the study eye were notably more common in the OZURDEX/OZURDEX group (12.9%) compared to either Sham/OZURDEX (3.4%).
For events reported in ≤ 1% of patients, mostly in only 1 or 2 patients per group, some differences between the first and second injection were seen. Review of these differences does not suggest a safety signal associated with repeat treatments.
The incidence of IOP increased was comparable between patients receiving either 1 or 2 doses of OZURDEX.
CONSTANCE 206207-025 (24-Month Post Approval Observational Study): The clinical safety of OZURDEX was assessed in a multicentre, 24-month real world observational study in the treatment of macular edema following RVO and non-infectious uveitis affecting the posterior segment of the eye. The most frequent adverse reactions observed in this study were consistent with the most frequent adverse reactions from clinical trials. Stratifications by injection frequency revealed increases in the incidence of adverse reactions among patients who received > 2 injections compared to patients who received ≤ 2 injections. The most frequent adverse reactions for patients who received > 2 injections included cataract [(24.7%, 44/178) for cataract formation and (32.0%, 57/178) for cataract progression] based on eyes with phakic lens status at baseline, vitreous hemorrhage (6.0%, 17/283), and increased IOP (24.0%, 68/283).
Treatment of Uveitis: Clinical Study 206207‐014: The clinical safety of OZURDEX was assessed in a multi-center, masked, and randomized, 26‐week phase 3 study in the treatment of non‐infectious uveitis affecting the posterior segment of the eye. A total of 76 patients were treated with OZURDEX and 75 were treated with sham. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIntraocular Pressure in Study‐014: As shown in Table 9, there were no clinically meaningful differences in the proportions of OZURDEX and sham patients who experienced IOP at ≥ 25 mmHg or ≥ 35 mmHg in the study eye, at any visit. At week 26, no OZURDEX patients and 3 sham patients had an IOP ≥ 25 mmHg; no patients had an IOP ≥ 35 mmHg. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTable 10 shows the proportion of patients with increases from baseline IOP ≥10 mmHg in the study eye was similar between OZURDEX and sham, except at week 8 where significantly higher percentages were observed with OZURDEX (9.6%) compared to sham (0.0%), p = 0.013. At week 26, only 1 OZURDEX patient and 2 sham patients showed an increase from baseline IOP ≥ 10 mmHg. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe proportion of OZURDEX-treated patients with increased IOP (≥ 25 mmHg) peaked at week 3 and returned to baseline by week 26. During the treatment period, no patients required incisional surgery for glaucoma. Three patients required laser iridotomies in the study eye for the treatment of pupillary block, iris bombe, and raised IOP.
CONSTANCE 206207-025 (24-Month Post Approval Observational Study): Refer to CONSTANCE Study Results under RVO as previously mentioned.
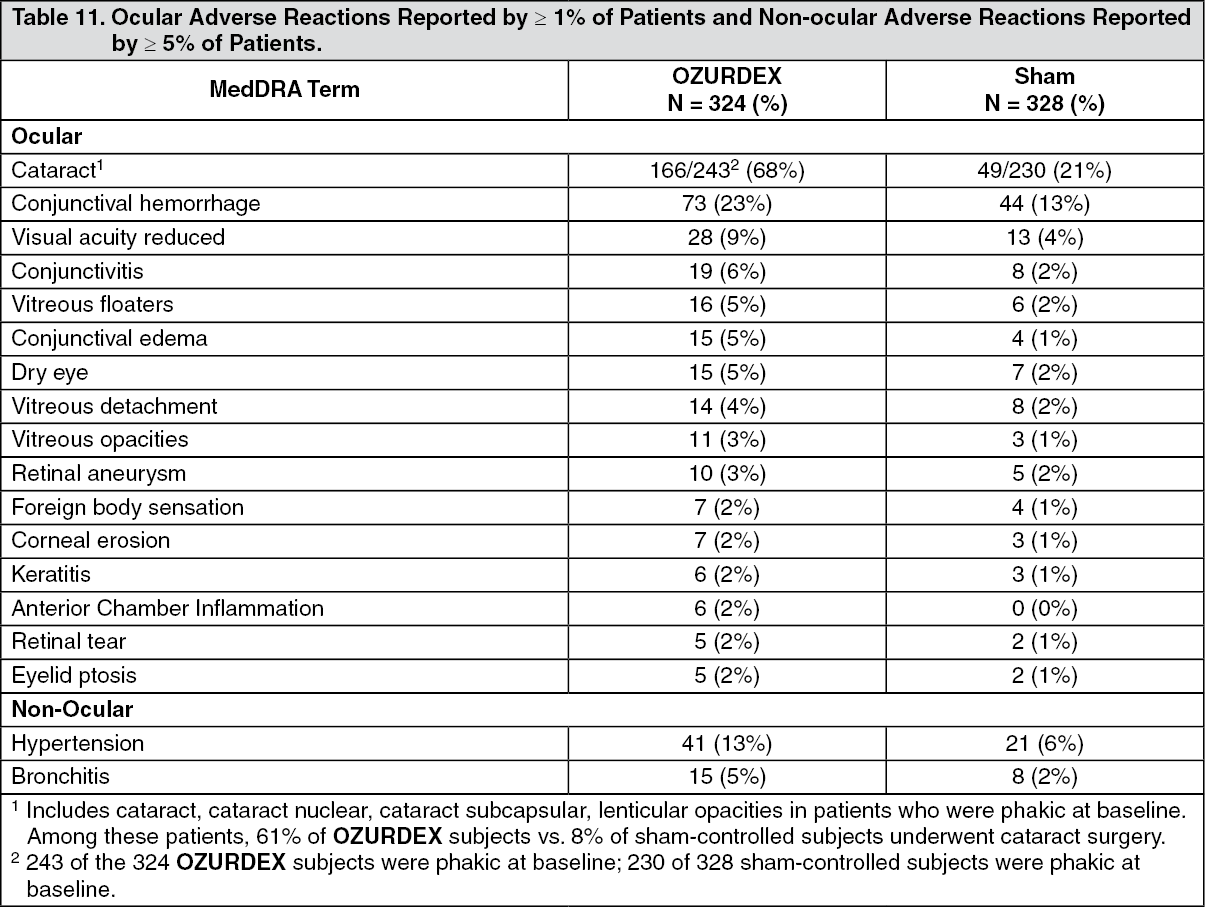
Treatment of Diabetic Macular Edema: The following information is based on the combined clinical trial results from 2 randomized, 3-year, sham-controlled studies in patients with diabetic macular edema. Discontinuation rates due to the adverse reactions listed in Table 11 were 3% in the OZURDEX group and 1% in the Sham group. The most common ocular (study eye) and non-ocular adverse reactions are shown in Tables 11 and 12: See Table 11.
 Click on icon to see table/diagram/image
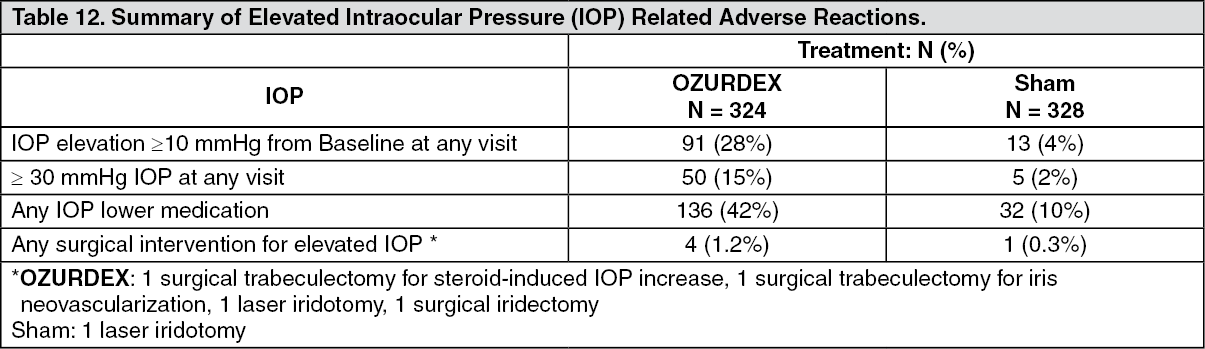
Click on icon to see table/diagram/imageIncreased Intraocular Pressure: See Table 12.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe increase in mean IOP was seen with each treatment cycle, and the mean IOP generally returned to baseline between treatment cycles (at the end of the 6 month period) shown as follows: See Figure 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCataracts and Cataract Surgery: At baseline, 243 of the 324 OZURDEX subjects were phakic; 230 of 328 sham-controlled subjects were phakic. The incidence of cataract development in patients who had a phakic study eye was higher in the OZURDEX group (68%) compared with Sham (21%). The median time of cataract being reported as an adverse event was approximately 15 months in the OZURDEX group and 12 months in the Sham group. Among these patients, 61% of OZURDEX subjects vs. 8% of sham-controlled subjects underwent cataract surgery, generally between Month 18 and Month 39 (Median Month 21 for OZURDEX group and 20 for Sham) of the studies.
Postmarketing Experience: The following adverse reactions have been identified during post-marketing use of OZURDEX in clinical practice. Because postmarketing reporting of these reactions is voluntary and from a population of uncertain size, it is not always possible to reliably estimate the frequency of these reactions. The reactions have been chosen for inclusion due to a combination of the frequency of reporting and/or possible causal connection to OZURDEX.
Eye disorders: Endophthalmitis; Hypotony of eye (associated with vitreous leakage due to injection); Retinal Detachment.
General disorders and administration site conditions: Complication of device insertion resulting in ocular tissue injury (implant misplacement); Device dislocation with or without corneal edema.
View ADR Monitoring Form