


 Sign Out
Sign Out

Most adverse reactions following the use of Optiray are of mild or moderate intensity, however, serious, life-threatening and fatal adverse reactions, mostly of cardiovascular origin, have been reported.
It should be kept in mind that, although most adverse reactions occur soon after the administration of the contrast medium, some adverse reactions can be delayed and can be of long-lasting nature.
The reported incidence of adverse reactions to contrast media in patients with a history of allergy is twice that of the general population. Patients with a history of previous reactions to a contrast medium are three times more susceptible than other patients.
The incidence of serious adverse reactions is higher with coronary arteriography than with other procedures. In those patients only who had coronary arteriography with Optiray, the incidence of angina was 1.2%. Cardiac decompensation, serious arrhythmias, myocardial ischemia or myocardial infarction may occur during coronary arteriography and left ventriculography.
In a controlled clinical trial involving 30 pediatric patients undergoing angiocardiography, no adverse reactions were reported.
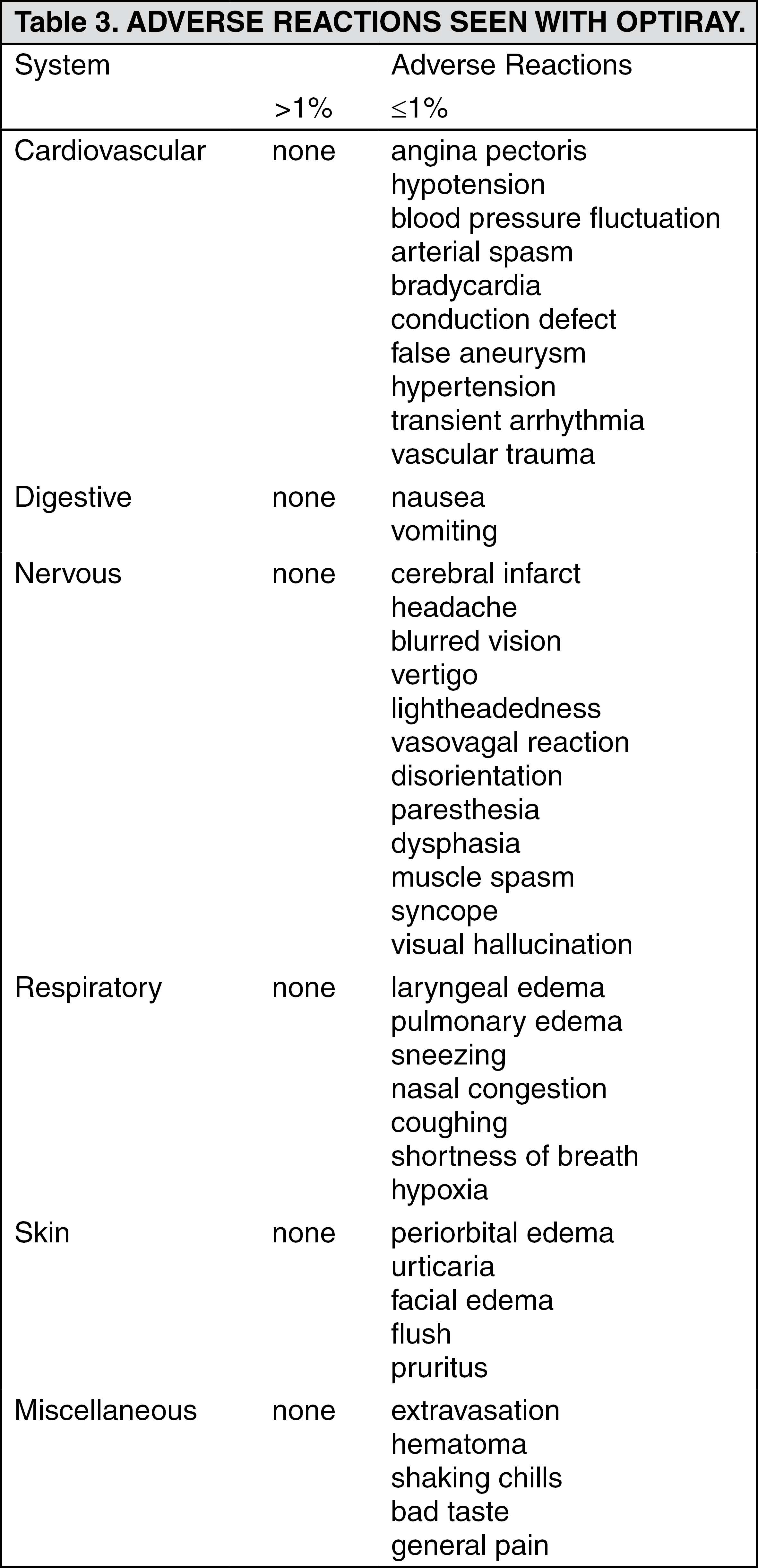
The following table of reactions is based upon clinical trials with Optiray formulations in 1506 patients, regardless of their direct attributability to the drug or the procedure.
Adverse reactions to specific procedures are also dealt with under Dosage & Administration. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn addition to the previously reported reactions, the following may occur with any contrast agent, including Optiray: Cardiovascular System: Hypoxia, heart block, bundle branch block, coronary thrombosis, cyanosis, hypertensive crisis, peripheral vasodilation, acute vascular insufficiency, circulatory collapse, hypotensive shock, cardiogenic shock.
Central Nervous System: Photomas, persistent blindness, taste perversion, anxiety, tinnitus, motor dysfunction, convulsion, somnolence, confusion, psychotic reaction, stiff neck, hemiparesis, hemiplegia, nystagmus, restlessness, tremors, aphasia, paralysis, coma and death.
Allergic Type Reaction: Purpura, conjunctivitis, lacrimation, erythematous, bullous or pleomorphic rashes, laryngospasm, bronchospasm, apnea, cyanosis, edema of glottis, laryngeal edema, angioneurotic edema, peripheral edema, anaphylactic shock. These allergic type reactions can progress into anaphylaxis, coma and death.
Renal System: Transient proteinuria, hematuria and rarely oliguria, anuria and renal failure.
Other Reactions: Diarrhea, dry mouth, pallor, venous and arterial thrombosis and rarely thrombophlebitis, rare cases of disseminated intravascular coagulation, neutropenia.
Pediatrics: In controlled clinical trials involving 128 patients for pediatric angiocardiography, contrast enhanced computed tomography of the head and body, and intravenous excretory urography, adverse reactions following the use of Optiray 320 were generally less frequent than with adults. Adverse reactions reported were as follows: fever (1.6%), nausea (0.8%), muscle spasm (0.8%), LV pressure change (0.8%).
Related to Procedure: Extravasation, perforation, rupture, dissection of blood vessels, hemorrhage, hematoma, false aneurysm, muscle spasm, arterial spasm, vascular trauma, ecchymosis and tissue necrosis, dislodgement of atheromatous plaques, thrombophlebitis, thrombosis embolization, injury to nerves and neighbouring organs, brachial plexus palsy following axillary artery injections.
TREATMENT OF ADVERSE REACTIONS TO CONTRAST MEDIA: Contrast media should be administered only by physicians thoroughly familiar with the emergency treatment of all adverse reactions to contrast media. The assistance of other trained personnel such as cardiologists, internists and anesthetists is required in the management of severe reactions.
A guideline for the treatment of adverse reactions is presented as follows. This outline is not intended to be a complete manual on the treatment of adverse reactions to contrast media or on cardio-pulmonary resuscitation. The physician should refer to the appropriate texts on the subject.
It is also realized that institutions or individual practitioners will already have appropriate systems in effect and that circumstances may dictate the use of additional or different measures.
For Minor Allergic Reactions (if considered necessary): The intravenous or intramuscular administration of an antihistamine such as diphenhydramine HCl 25-50 mg is generally sufficient (contraindicated in epileptics). The resulting drowsiness makes it imperative to ensure that out-patients do not drive or go home unaccompanied.
Major or Life-threatening Reactions: A major reaction may be manifested by signs and symptoms of cardiovascular collapse, severe respiratory difficulty and nervous system dysfunction. Convulsions, coma and cardio-respiratory arrest may ensue. The following measures should be considered: 1. Start emergency therapy immediately - carefully monitoring vital signs.
2. Have emergency resuscitation team summoned - do not leave patient unattended.
3. Ensure patent airway - guard against aspiration.
4. Commence artificial respiration if patient is not breathing.
5. Administer oxygen, if necessary.
6. Start external cardiac massage in the event of cardiac arrest.
7. Establish route for i.v medication by starting infusion of appropriate solution (5% dextrose in water).
8. Judiciously administer specific drug therapy as indicated by the type and severity of the reaction.
Careful monitoring is mandatory to detect adverse reactions of all drugs administered: a) Soluble hydrocortisone 500-1000 mg i.v. for all acute allergic anaphylactic reactions.
b) Adrenaline 1:1000 solution (in the presence of anoxia it may cause ventricular fibrillation; CAUTION in patients on adrenergic beta blockers. See Precautions).
i) 0.2-0.4 mL subcutaneously for severe allergic reactions.
ii) in extreme emergency 0.1 mL per minute, appropriately diluted, may be given intravenously until desired effect is obtained. Do not exceed 0.4 mL.
iii) in case of cardiac arrest 0.1-0.2 mL, appropriately diluted, may be given intracardially.
c) In hypotension (carefully monitoring blood pressure): i) Phenylephrine HCl 0.1-0.5 mg appropriately diluted slowly i.v. or by slow infusion OR; ii) Noradrenalin 4 mL of 0.2% solution in 1000 mL of 5% dextrose by slow drip infusion.
d) Sodium bicarbonate 5%, 50 mL i.v. every 10 minutes as needed to combat post-arrest acidosis.
e) Atropine 0.4-0.6 mg i.v. to increase heart rate in sinus bradycardia. May reverse 2nd or 3rd degree block.
f) To control convulsions: i) Pentobarbital Sodium 50 mg in fractional doses slowly i.v. (contraindicated if cyanosis is present) OR; ii) Diazepam 5-10 mg slowly i.v. titrating the dose to the response of the patient.
9. Defibrillation, administration of antiarrhythmics and additional emergency measures and drugs may be required.
10. The patient should be transferred to the intensive care unit when feasible for further monitoring and treatment.
View ADR Monitoring Form