


 Sign Out
Sign Out

The serious adverse reactions observed more frequently (≥5%) with lenalidomide in maintenance than placebo were: Pneumonias (10.6%; combined term) from IFM 2005-02; Lung infection (9.4% [9.4% after the start of maintenance treatment]) from CALGB 100104.
In the IFM 2005-02 study, the adverse reactions observed more frequently with lenalidomide maintenance than placebo were neutropenia (60.8%), bronchitis (47.4%), diarrhoea (38.9%), nasopharyngitis (34.8%), muscle spasms (33.4%), leucopenia (31.7%), asthenia (29.7%), cough (27.3%), thrombocytopenia (23.5%), gastroenteritis (22.5%) and pyrexia (20.5%).
In the CALGB 100104 study, the adverse reactions observed more frequently with lenalidomide maintenance than placebo were neutropenia (79.0% [71.9% after the start of maintenance treatment]), thrombocytopenia (72.3% [61.6%]), diarrhoea (54.5% [46.4%]), rash (31.7% [25.0%]), upper respiratory tract infection (26.8% [26.8%]), fatigue (22.8% [17.9%]), leucopenia (22.8% [18.8%]) and anemia (21.0% [13.8%]).
Newly diagnosed multiple myeloma: patients who are not eligible for transplant treated with lenalidomide in combination with low dose dexamethasone: The serious adverse reactions observed more frequently (≥5%) with lenalidomide in combination with low dose dexamethasone (Rd and Rd18) than with melphalan, prednisone and thalidomide (MPT) were: Pneumonia (9.8%); Renal failure (including acute) (6.3%).
The adverse reactions observed more frequently with Rd or Rd18 than MPT were: diarrhoea (45.5%), fatigue (32.8%), back pain (32.0%), asthenia (28.2%), insomnia (27.6%), rash (24.3%), decreased appetite (23.1%), cough (22.7%), pyrexia (21.4%), and muscle spasms (20.5%).
Multiple myeloma: patients with at least one prior therapy: In two Phase III placebo-controlled studies, 353 patients with multiple myeloma were exposed to the lenalidomide/dexamethasone combination and 351 to the placebo/dexamethasone combination. The most serious adverse reactions observed more frequently in lenalidomide/dexamethasone than placebo/dexamethasone combination were: Venous thromboembolism (deep vein thrombosis, pulmonary embolism); Grade 4 neutropenia.
The observed adverse reactions which occurred more frequently with lenalidomide and dexamethasone than placebo and dexamethasone in pooled multiple myeloma clinical trials (MM-009 and MM-010) were fatigue (43.9%), neutropenia (42.2%), constipation (40.5%), diarrhoea (38.5%), muscle cramp (33.4%), anemia (31.4%), thrombocytopenia (21.5%), and rash (21.2%).
Tabulated list of adverse reactions: The adverse reactions observed in patients treated with lenalidomide are listed as follows by system organ class and frequency. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. Frequencies are defined as: very common (≥ 1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data).
Adverse reactions have been included under the appropriate category in the table as follows according to the highest frequency observed in any of the main clinical trials.
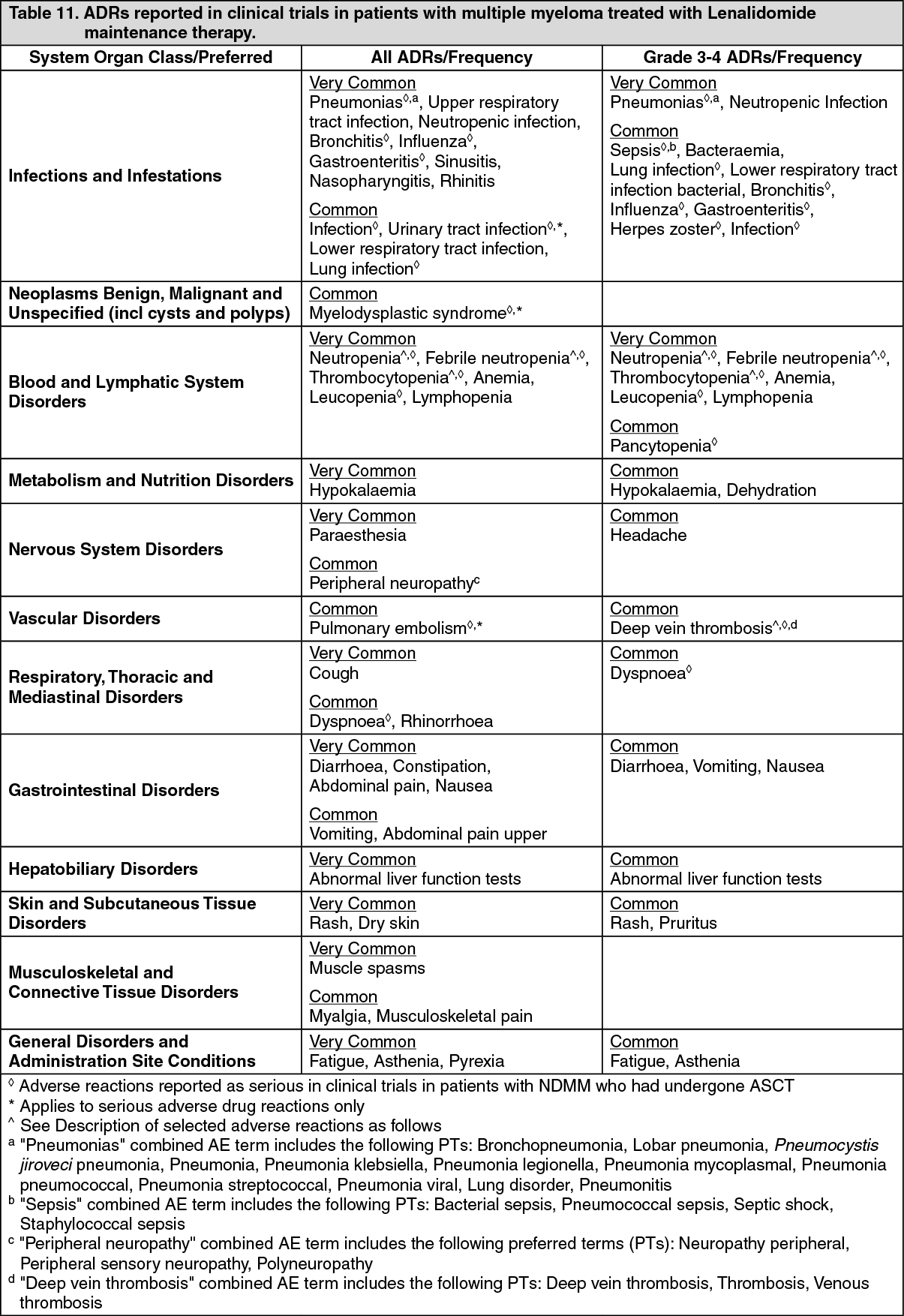
Tabulated summary for monotherapy in MM: The following table is derived from data gathered during NDMM studies in patients who have undergone ASCT treated with lenalidomide maintenance. The data were not adjusted according to the longer duration of treatment in the lenalidomide-containing arms continued until disease progression versus the placebo arms in the pivotal multiple myeloma studies. (See Table 11.)
 Click on icon to see table/diagram/image
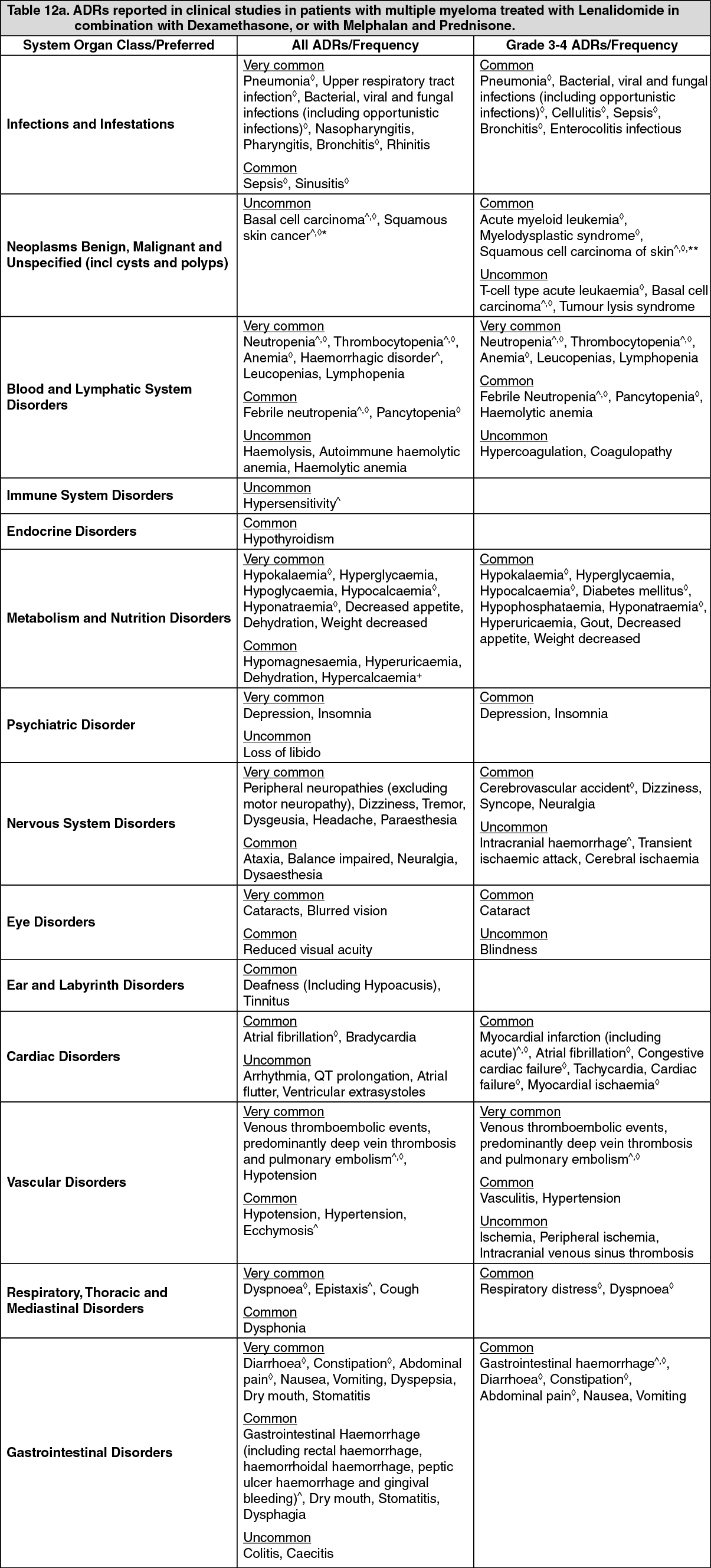
Click on icon to see table/diagram/imageTabulated summary for combination therapy in MM: The following table is derived from data gathered during the multiple myeloma studies with combination therapy. The data were not adjusted according to the longer duration of treatment in the lenalidomide containing arms continued until disease progression versus the comparator arms in the pivotal multiple myeloma studies. (See Tables 12a and 12b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image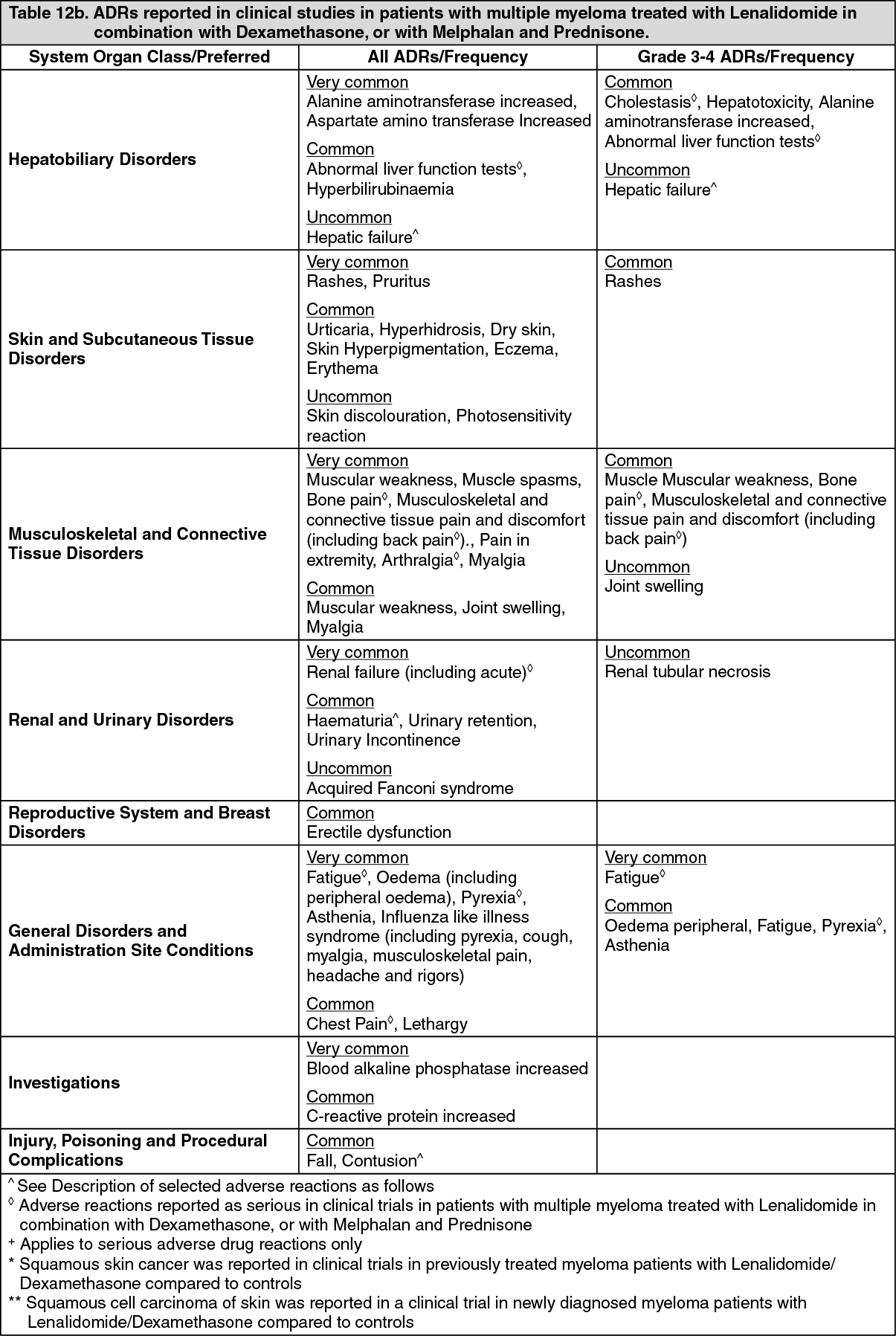 Click on icon to see table/diagram/image
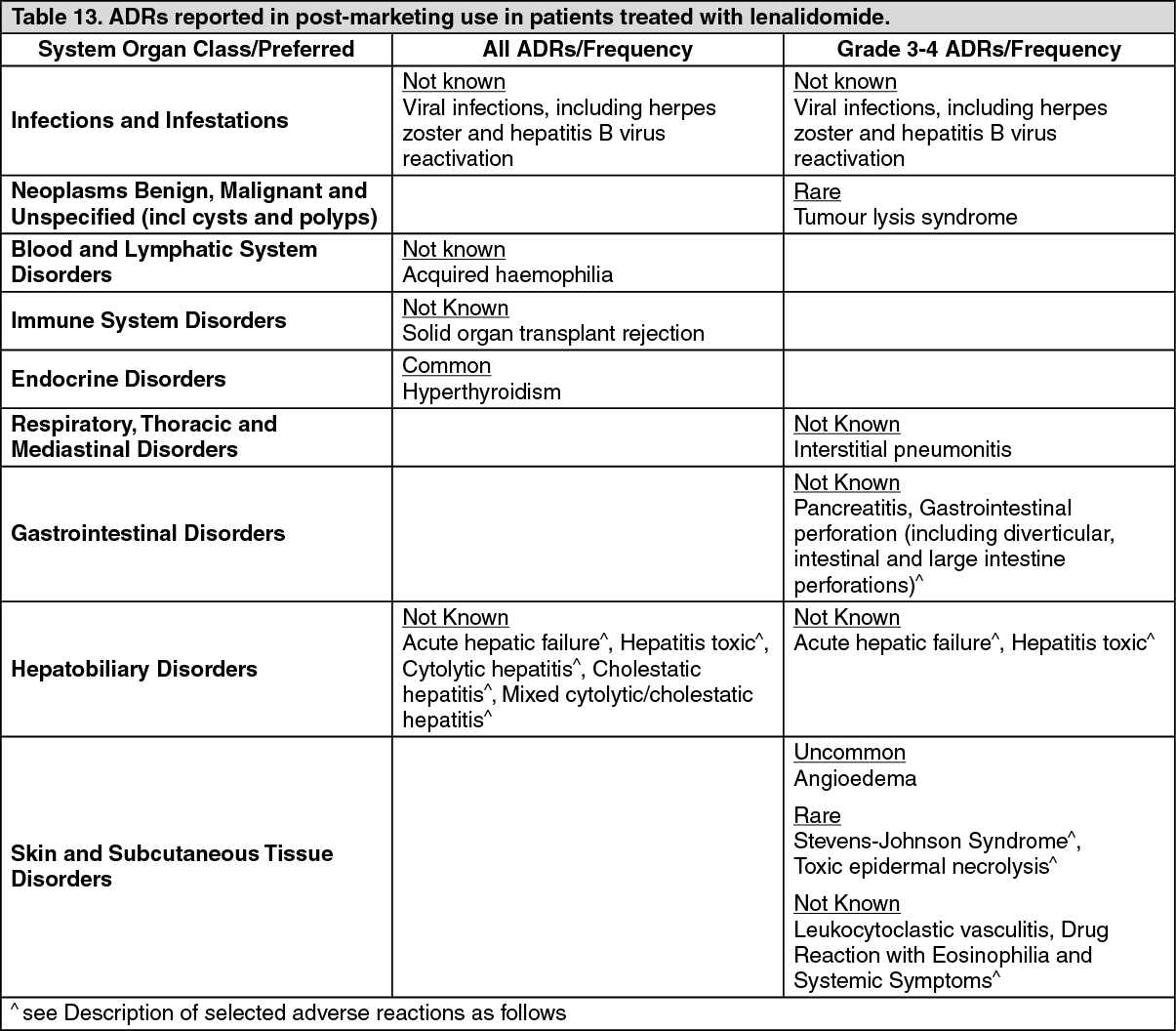
Click on icon to see table/diagram/imageTabulated summary of post-marketing adverse reactions: In addition to the previously mentioned adverse reactions identified from the pivotal clinical trials, the following table is derived from data gathered from post-marketing data. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Teratogenicity: Lenalidomide is structurally related to thalidomide. Thalidomide is a known human teratogenic active substance that causes severe life-threatening birth defects. Lenalidomide induced in monkeys malformations similar to those described with thalidomide. If lenalidomide is taken during pregnancy, a teratogenic effect of lenalidomide in humans is expected.
Neutropenia and thrombocytopenia: Newly diagnosed multiple myeloma: patients who have undergone ASCT treated with lenalidomide maintenance: Lenalidomide maintenance after ASCT is associated with a higher frequency of grade 4 neutropenia compared to placebo maintenance (32.1% vs 26.7% [16.1% vs 1.8% after the start of maintenance treatment] in CALGB 100104 and 16.4% vs 0.7% in IFM 2005-02, respectively). Treatment-emergent AEs of neutropenia leading to lenalidomide discontinuation were reported in 2.2% of patients in CALGB 100104 and 2.4% of patients in IFM 2005-02, respectively. Grade 4 febrile neutropenia was reported at similar frequencies in the lenalidomide maintenance arms compared to placebo maintenance arms in both studies (0.4% vs 0.5% [0.4% vs 0.5% after the start of maintenance treatment] in CALGB 100104 and 0.3% vs 0% in IFM 2005-02, respectively).
Lenalidomide maintenance after ASCT is associated with a higher frequency of grade 3 or 4 thrombocytopenia compared to placebo maintenance (37.5% vs 30.3% [17.9% vs 4.1% after the start of maintenance treatment] in CALGB 100104 and 13.0% vs 2.9% in IFM 2005-02, respectively).
Newly diagnosed multiple myeloma: patients who are not eligible for transplant treated with lenalidomide in combination with low dose dexamethasone: The combination of lenalidomide with low dose dexamethasone in newly diagnosed multiple myeloma patients is associated with a lower frequency of grade 4 neutropenia (8.5% in Rd and Rd18, compared with MPT (15%). Grade 4 febrile neutropenia was observed infrequently (0.6% in Rd and Rd18 compared with 0.7% in MPT).
The combination of lenalidomide with low dose dexamethasone in newly diagnosed multiple myeloma patients is associated with a lower frequency of grade 3 and 4 thrombocytopenia (8.1% in Rd and Rd18) compared with MPT (11%).
Multiple myeloma: patients with at least one prior therapy: The combination of lenalidomide with dexamethasone in multiple myeloma patients is associated with a higher incidence of grade 4 neutropenia (5.1% in lenalidomide/dexamethasone-treated patients compared with 0.6% in placebo/dexamethasone-treated patients). Grade 4 febrile neutropenia episodes were observed infrequently (0.6% in lenalidomide/dexamethasone-treated patients compared to 0.0% in placebo/dexamethasone treated patients).
The combination of lenalidomide with dexamethasone in multiple myeloma patients is associated with a higher incidence of grade 3 and grade 4 thrombocytopenia (9.9% and 1.4%, respectively, in lenalidomide/dexamethasone-treated patients compared to 2.3% and 0.0% in placebo/dexamethasone-treated patients).
Venous thromboembolism: An increased risk of DVT and PE is associated with the use of the combination of lenalidomide with dexamethasone in patients with multiple myeloma, and to a lesser extent in patient with multiple myeloma treated with lenalidomide monotherapy (see Interactions).
Concomitant administration of erythropoietic agents or previous history of DVT may also increase thrombotic risk in these patients.
Myocardial infarction: Myocardial infarction has been reported in patients receiving lenalidomide, particularly in those with known risk factors.
Haemorrhagic disorders: Haemorrhagic disorders are listed under several system organ classes: Blood and lymphatic system disorders; nervous system disorders (intracranial haemorrhage); respiratory, thoracic and mediastinal disorders (epistaxis); gastrointestinal disorders (gingival bleeding, haemorrhoidal haemorrhage, rectal haemorrhage); renal and urinary disorders (haematuria); injury, poisoning and procedural complications (contusion) and vascular disorders (ecchymosis).
Allergic reactions: Cases of allergic reaction/hypersensitivity reactions have been reported. A possible cross-reaction between lenalidomide and thalidomide has been reported in the literature.
Severe skin reactions: Severe cutaneous reactions including SJS, and TEN and DRESS have been reported with the use of lenalidomide. Patients with a history of severe rash associated with thalidomide treatment should not receive lenalidomide.
Second primary malignancies: In clinical trials in previously treated myeloma patients with lenalidomide/dexamethasone compared to controls, mainly comprising of basal cell or squamous cell skin cancers.
Acute myeloid leukaemia (AML): Multiple myeloma: Cases of AML have been observed in clinical trials of newly diagnosed multiple myeloma in patients taking lenalidomide treatment in combination with melphalan or immediately following high dose melphalan and ASCT. This increase was not observed, in clinical trials of newly diagnosed multiple myeloma in patients taking lenalidomide in combination with low dose dexamethasone compared to thalidomide in combination with melphalan and prednisone.
Hepatic disorders: The following post-marketing adverse reactions have been reported (frequency unknown): acute hepatic failure and cholestasis (both potentially fatal), toxic hepatitis, cytolytic hepatitis, mixed cytolytic/cholestatic hepatitis.
Rhabdomyolysis: Rare cases of rhabdomyolysis have been observed, some of them when lenalidomide is administered with a statin.
Thyroid disorders: Cases of hypothyroidism and cases of hyperthyroidism have been reported.
Gastrointestinal disorders: Gastrointestinal perforations have been reported during treatment with lenalidomide. Gastrointestinal perforations may lead to septic complications and may be associated with fatal outcome.
View ADR Monitoring Form