


 Sign Out
Sign Out

 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEnsure that patients with pre-existing renal insufficiency are not volume depleted; discontinue GAMUNEX-C if renal function deteriorates.
For patients at risk of renal dysfunction or thrombosis, administer GAMUNEX-C at the minimum infusion rate practicable.
Intravenous or Subcutaneous Administration: PI: DO NOT ADMINISTER SUBCUTANEOUSLY FOR ITP PATIENTS. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGAMUNEX-C consists of 9%-11% protein in 0.16-0.24 M glycine. The buffering capacity of GAMUNEX-C is 35.0 mEq/L (0.35 mEq/g protein). A dose of 1 g/kg body weight therefore represents an acid load of 0.35 mEq/kg body weight. The total buffering capacity of whole blood in a normal individual is 45-50 mEq/L of blood, or 3.6 mEq/kg body weight. Thus, the acid load delivered with a dose of 1 g/kg of GAMUNEX-C would be neutralized by the buffering capacity of whole blood alone, even if the dose was infused instantaneously.
PI: As there are significant differences in the half-life of IgG among patients with primary humoral immunodeficiencies, the frequency and amount of immunoglobulin therapy may vary from patient to patient. The proper amount can be determined by monitoring clinical response.
Intravenous (IV): The dose of GAMUNEX-C for patients with PI is 300 to 600 mg/kg body weight (3-6 mL/kg) administered every 3 to 4 weeks. The dosage may be adjusted over time to achieve the desired trough levels and clinical responses.
The recommended initial infusion rate is 1 mg/kg/min (0.01 mL/kg/min). If the infusion is well-tolerated, the rate may be gradually increased to a maximum of 8 mg/kg/min (0.08 mL/kg/min). For patients judged to be at risk for renal dysfunction or thrombosis, administer GAMUNEX-C at the minimum infusion rate practicable. (See Precautions.)
If a patient routinely receives a dose of less than 400 mg/kg of GAMUNEX-C every 3 to 4 214 weeks (less than 4 mL/kg), and is at risk of measles exposure (i.e., traveling to a measles 215 endemic area), administer a dose of at least 400 mg/kg (4 mL/kg) just prior to the expected 216 measles exposure. If a patient has been exposed to measles, a dose of 400 mg/kg (4 mL/kg) 217 should be administered as soon as possible after exposure.
Subcutaneous (SC): The dose should be individualized based on the patient's clinical response to GAMUNEX-C therapy and serum IgG trough levels. Begin treatment with GAMUNEX-C one week after the patient's last IGIV infusion. See below under "Initial Weekly Dose". Prior to switching treatment from IGIV to GAMUNEX-C, obtain the patient's serum IgG trough level to guide subsequent dose adjustments. See below under "Dose Adjustment".
Establish the initial weekly dose of GAMUNEX-C by converting the monthly IGIV dose into a weekly equivalent and increasing it using a dose adjustment factor. The goal is to achieve a systemic serum IgG exposure (Area Under the Concentration-Time Curve [AUC]) not inferior to that of the previous IGIV treatment. If the patient has not been previously treated with IV GAMUNEX-C, convert the monthly IGIV dose by multiplying by 1.37, then dividing this dose into weekly doses based on the patient's previous IGIV treatment interval. Monitor the patient's clinical response, and adjust dose accordingly.
Initial Weekly Dose: To calculate the initial weekly dose of subcutaneous administration of GAMUNEX-C, multiply the previous IGIV dose in grams by the dose adjustment factor of 1.37; then divide this by the number of weeks between doses during the patient's IGIV treatment (i.e., 3 or 4). (See Equation.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDose Adjustment: Over time, the dose may need to be adjusted to achieve the desired clinical response and serum IgG trough level. To determine if a dose adjustment may be considered, measure the patient's serum IgG trough level on IGIV and as early as 5 weeks after switching from IGIV to subcutaneous. The target serum IgG trough level on weekly SC treatment is projected to be the last IGIV trough level plus 340 mg/dL. To determine if further dose adjustments are necessary, monitor the patient's IgG trough level every 2 to 3 months.
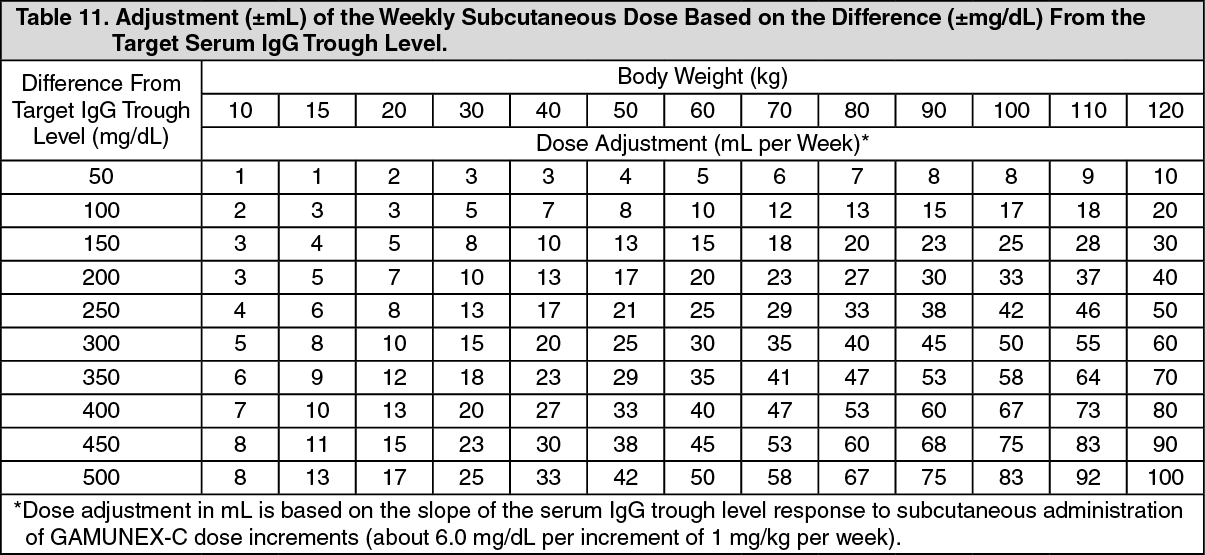
To adjust the dose based on trough levels, calculate the difference (in mg/dL) of the patient's serum IgG trough level from the target IgG trough level (the last IGIV trough level + 340 mg/dL). Then find this difference in Table 11 and the corresponding amount (in mL) by which to increase or decrease the weekly dose based on the patient's body weight. However, the patient's clinical response should be the primary consideration in dose adjustment. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor example, if a patient with a body weight of 70 kg has an actual IgG trough level of 900 mg/dL and the target level is 1000 mg/dL, this results in a difference of 100 mg/dL. Therefore, increase the weekly dose of subcutaneous dose by 12 mL.
Monitor the patient's clinical response, and repeat the dose adjustment as needed.
Dosage requirements for patients switching to GAMUNEX-C from another Immune Globulin Subcutaneous (IGSC) product have not been studied. If a patient on GAMUNEX-C does not maintain an adequate clinical response or a serum IgG trough level equivalent to that of the previous IGSC treatment, the physician may want to adjust the dose. For such patients, Table 11 also provides guidance for dose adjustment to achieve a desired IGSC trough level.
ITP: DO NOT ADMINISTER SUBCUTANEOUSLY (see Precautions): GAMUNEX-C may be administered at a total dose of 2 g/kg, divided in two doses of 1 g/kg (10 mL/kg) given on two consecutive days or into five doses of 0.4 g/kg (4 mL/kg) given on five consecutive days. If after administration of the first of two daily 1 g/kg (10 mL/kg) doses, an adequate increase in the platelet count is observed at 24 hours, the second dose of 1 g/kg (10 mL/kg) body weight may be withheld.
Forty-eight ITP subjects were treated with 2 g/kg GAMUNEX-C, divided in two 1 g/kg doses (10 mL/kg) given on two successive days. With this dose regimen 35/39 subjects (90%) responded with a platelet count from less than or equal to 20 x 109/L to more than or equal to 50 x 109/L within 7 days after treatment. The high dose regimen (1 g/kg x 1-2 days) is not recommended for individuals with expanded fluid volumes or where fluid volume may be a concern.
The recommended initial infusion rate is 1 mg/kg/min (0.01 mL/kg/min). If the infusion is well-tolerated, the rate may be gradually increased to a maximum of 8 mg/kg/min (0.08 mL/kg/min). For patients judged to be at risk for renal dysfunction or thrombosis, administer GAMUNEX-C at the minimum infusion rate practicable (see Precautions).
CIDP: GAMUNEX-C may be initially administered as a total loading dose of 2 g/kg (20 mL/kg) given in divided doses over two to four consecutive days. GAMUNEX-C may be administered as a maintenance infusion of 1 g/kg (10 mL/kg) administered over 1 day or divided into two doses of 0.5 g/kg (5 mL/kg) given on two consecutive days, every 3 weeks.
The recommended initial infusion rate is 2 mg/kg/min (0.02 mL/kg/min). If the infusion is well tolerated, the rate may be gradually increased to a maximum of 8 mg/kg/min (0.08 mL/kg/min). For patients judged to be at risk for renal dysfunction or thrombosis, administer GAMUNEX-C at the minimum infusion rate practicable (see Precautions).
Administration: Administer intravenously for PI, ITP and CIDP.
GAMUNEX-C may also be administered subcutaneously for the treatment of PI.
Administer GAMUNEX-C at room temperature.
Inspect GAMUNEX-C visually for particulate matter and discoloration prior to administration, whenever the solution and container permit.
Do not use if turbid and/or if discoloration is observed.
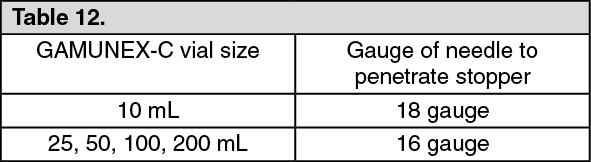
Intravenous: Use only 18 gauge needles to penetrate the stopper for dispensing product from the 10 mL vial.
Use 16 gauge needles or dispensing pins only with 25 mL vial sizes and larger.
Insert needles or dispensing pins only once and be within the stopper area delineated by the raised ring.
Penetrate the stopper perpendicular to the plane of the stopper within the ring. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUse promptly any vial that has been opened.
Discard partially used vials.
If dilution is required, GAMUNEX-C may be diluted with 5% dextrose in water (D5/W). Do not dilute with saline. Infuse GAMUNEX-C using a separate line by itself, without 313 mixing with other intravenous fluids or medications the subject might be receiving. The GAMUNEX-C infusion line can be flushed with 5% dextrose in water (D5/W) or 0.9% sodium chloride for injection.
Subcutaneous for PI Only: Instructions for Administration: Prior to use, allow the solution to reach ambient room temperature.
DO NOT SHAKE.
Do not use if the solution is cloudy or has particulates.
Check the product expiration date on the vial. Do not use beyond the expiration date.
1. Use aseptic technique when preparing and administering GAMUNEX-C for injection.
2. Remove the protective cap from the vial to expose the central portion of the rubber stopper.
3. Wipe the rubber stopper with alcohol and allow to dry.
4. Using a sterile syringe and needle, prepare to withdraw GAMUNEX-C by first injecting air into the vial that is equivalent to the amount of GAMUNEX-C to be withdrawn. Then withdraw the desired volume of GAMUNEX-C. If multiple vials are required to achieve the desired dose, repeat this step.
5. Follow the manufacturer's instructions for filling the pump reservoir and preparing the pump, administration tubing and Y-site connection tubing, if needed. Be sure to prime the administration tubing to ensure that no air is left in the tubing or needle by filling the tubing/needle with GAMUNEX-C.
6. Select the number and location of injection sites.
7. Cleanse the injection site(s) with antiseptic solution using a circular motion working from the center of the site and moving to the outside. Sites should be clean, dry, and at least two inches apart.
8. Grasp the skin between two fingers and insert the needle into the subcutaneous tissue.
9. Repeat priming and needle insertion steps using a new needle, administration tubing and a new infusion site. Secure the needle in place by applying sterile gauze or transparent dressing over the site.
10. If using multiple, simultaneous injection sites, use Y-site connection tubing and secure to the administration tubing.
11. Infuse GAMUNEX-C following the manufacturer's instructions for the pump.
Rate of Administration: Intravenous: Following initial infusion (see table 13), the infusion rate may be gradually increased to a maximum of 0.08 mL/kg per minute (8 mg/kg per minute) as tolerated. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMonitor patient vital signs throughout the infusion. Slow or stop infusion if adverse reactions occur. If symptoms subside promptly, the infusion may be resumed at a lower rate that is comfortable for the patient.
Certain severe adverse drug reactions may be related to the rate of infusion. Slowing or stopping the infusion usually allows the symptoms to disappear promptly.
Ensure that patients with pre-existing renal insufficiency are not volume depleted. For patients at risk of renal dysfunction or thrombosis, administer GAMUNEX-C at the minimum infusion rate practicable and discontinue GAMUNEX-C if renal function deteriorates.
Subcutaneous for PI Only: For PI, it is recommended that GAMUNEX-C is infused at a rate of 20 mL/hr per infusion site.
In the SC clinical study, the mean volume administered per infusion site was 34 mL (17-69 mL) and the majority of infusions were administered at a rate of 20 mL/hr per site. Multiple simultaneous infusion sites were enabled by administration tubing and Y-site connection tubing. Most subjects utilized 4 infusion sites per infusion with abdomen and thighs being the most commonly used sites. The maximum number of infusion sites is 8. Injection sites should be at least 2 inches apart.