Pharmacology: Pharmacodynamics: Mechanism of action: Ceftazidime inhibits bacterial peptidoglycan cell wall synthesis following attachment to penicillin binding proteins (PBPs), which leads to bacterial cell lysis and death. This broad spectrum cephalosporin is active against many important Gram-negative and Gram-positive bacterial pathogens
in vitro. Avibactam is a non β-lactam, β-lactamase inhibitor that acts by forming a covalent adduct with the enzyme that is stable to hydrolysis. It inhibits both Ambler class A and class C β-lactamases, including extended-spectrum β-lactamases (ESBLs), KPC carbapenemases, and AmpC enzymes. Avibactam also inhibits the class D carbapenemase OXA-48, which does not significantly hydrolyze ceftazidime. Avibactam has no clinically relevant
in vitro antibacterial activity. Avibactam did not induce transcription of
bla
AmpC in
Enterobacter cloacae, Citrobacter freundii or
Pseudomonas aeruginosa in vitro at concentrations used to treat patients.
Mechanism of resistance: Ceftazidime-avibactam is not active against metallo-β-lactamase-producing bacteria. Bacterial resistance mechanisms that could potentially affect ceftazidime-avibactam include mutant or acquired PBPs, decreased outer membrane permeability to either compound, active efflux of either compound, mutated or acquired β-lactamase enzymes insensitive to avibactam and able to hydrolyze ceftazidime.
Cross-resistance: An absence of cross-resistance between ceftazidime-avibactam and fluoroquinolones or aminoglycosides has been demonstrated
in vitro using molecularly-characterized clinical isolates. Some isolates resistant to ceftazidime (and other cephalosporins) or to carbapenems are susceptible to ceftazidime-avibactam. There is cross-resistance with β-lactam antibacterial agents, including carbapenems, when the mechanism is production of metallo-β-lactamases, such as VIM-2.
Interaction with other antimicrobial agents: In vitro interaction tests with ceftazidime-avibactam show ceftazidime-avibactam has little potential to antagonize or be antagonized by other antibiotics of various classes (e.g. metronidazole, tobramycin, levofloxacin, vancomycin, linezolid, colistin, tigecycline).
Susceptibility testing: The prevalence of acquired resistance may vary geographically and with time for selected species. Local information on resistance is desirable, particularly when treating severe infections.
The susceptibility to ceftazidime-avibactam of a given clinical isolate should be determined by standard methods. Interpretations of test results should be made in accordance with local infectious diseases and clinical microbiology guidelines.
Minimum Inhibitory Concentration (MIC) breakpoints established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) for ceftazidime-avibactam are as follows: (See Table 1.)
 Click on icon to see table/diagram/image
Pharmacokinetic/pharmacodynamic relationship:
Click on icon to see table/diagram/image
Pharmacokinetic/pharmacodynamic relationship: The antimicrobial activity of ceftazidime-avibactam against specific pathogens has been shown to best correlate with the percent time of free-drug concentration above the ceftazidime-avibactam minimum inhibitory concentration over the dose interval (%
fT >MIC of ceftazidime-avibactam) for ceftazidime, and the percent time of the free drug concentration above a threshold concentration over the dose interval (%
fT>C
T) for avibactam.
Clinical efficacy against specific pathogens: Efficacy has been demonstrated in clinical studies against the pathogens, listed under each indication, that were susceptible to ceftazidime-avibactam
in vitro.
Complicated intra-abdominal infections: Gram-negative micro-organisms:
Citrobacter freundii; Enterobacter cloacae; Escherichia coli; Klebsiella oxytoca; Klebsiella pneumoniae; Pseudomonas aeruginosa.
Complicated urinary-tract infections: Gram-negative micro-organisms:
Escherichia coli; Klebsiella pneumoniae; Proteus mirabilis; Enterobacter cloacae; Pseudomonas aeruginosa.
Hospital-acquired pneumonia including ventilator-associated pneumonia: Gram-negative micro-organisms:
Enterobacter cloacae; Escherichia coli; Klebsiella pneumoniae; Proteus mirabilis; Serratia marcescens; Pseudomonas aeruginosa.
Clinical efficacy has not been established against the following pathogens that are relevant to the approved indications although
in vitro studies suggest that they would be susceptible to ceftazidime-avibactam in the absence of acquired mechanisms of resistance.
Gram-negative micro-organisms:
Citrobacter koseri; Enterobacter aerogenes; Morganella morganii; Proteus vulgaris; Providencia rettgeri.
Ceftazidime-avibactam is active
in vitro against
Streptococcus pyogenes and
Streptococcus agalactiae, but not generally active against other clinically-important Gram-positive bacteria including methicillin-resistant
Staphylococcus aureus (MRSA).
Clinical efficacy and safety: Complicated intra-abdominal infections: A total of 1058 adults with complicated intra-abdominal infections (defined as infections that require surgical intervention and extend beyond the hollow viscus into the intraperitoneal space) were randomised and received treatment in two identical randomised, multi-centre, multinational, double-blind studies (RECLAIM 1 and RECLAIM 2) comparing ceftazidime-avibactam (2 g of ceftazidime and 0.5 g of avibactam) administered intravenously over 2 hours every 8 hours plus metronidazole (0.5 g) to meropenem (1 g) administered intravenously over 30 minutes. Treatment duration was 5 to 14 days. The modified intent-to-treat (MITT) population included all patients who met the disease definition of cIAI and received at least 1 dose of the study drug. The clinically evaluable (CE) population included patients who had an appropriate diagnosis of cIAI and excluded patients with a bacterial species typically not expected to respond to both study drugs (i.e.
Acinetobacter baumannii or
Stenotrophomonas spp.) and/or who had an important protocol deviation impacting the assessment of efficacy.
The primary efficacy endpoint was the clinical response at the Test of Cure (TOC) visit in the co-primary populations of the CE and MITT patients in Table 2 as follows. (See Table 2.)
Click on icon to see table/diagram/image
Clinical cure rates at TOC by pathogen in the microbiologically Modified Intent to Treat (mMITT) population for Gram-negative aerobes are shown in Table 3 as follows. (See Table 3.)
Click on icon to see table/diagram/image
A further 432 adults with complicated intra-abdominal infections were randomised and received treatment in a multi-centre, double-blind study (RECLAIM 3) conducted in 3 Asian countries (China, Republic of Korea and Vietnam). The patient population and key aspects of the study design were identical to RECLAIM apart from the primary efficacy endpoint of clinical response at the TOC visit being solely in the CE population (see Table 4 as follows).
Click on icon to see table/diagram/image
Clinical cure rates at TOC by pathogen in the microbiologically modified Intent to Treat (mMITT) population for Gram-negative aerobes are shown in Table 5 as follows. (See Table 5.)
Click on icon to see table/diagram/image
Among patients with baseline bacteraemia who were enrolled in any of the phase 3 cIAI studies (RECLAIM, RECLAIM3 or REPRISE), clinical cure at TOC in the subset of patients with bacteraemia due to aerobic Gram-negative pathogens was observed in 9/11 (81.8%) patients treated with CAZ-AVI + MTZ and 9/10 (90.0%) patients treated with comparators (meropenem or best-available therapy). The most common Gram-negative baseline pathogens isolated from the blood were
E. coli and
P. aeruginosa. A favourable per-pathogen microbiological response at TOC was reported in 9/11 (81.8%) CAZ-AVI and 6/6 (100.0%) comparator-treated patients with
E. coli bacteraemia; and 3/4 (75.0%) CAZ-AVI and 2/2 (100.0%) comparator-treated patients with
P. aeruginosa bacteraemia.
Complicated urinary tract infections: A total of 1020 adults with documented complicated urinary tract infection (cUTI) (737 with acute pyelonephritis and 283 with cUTI without acute pyelonephritis) were randomised and received treatment in a phase III multicentre, double-blind, comparative study. Treatment was with either ceftazidime-avibactam (2 g/0.5 g) IV over 2 hours every 8 hours or doripenem 0.5 g IV over 60 mins every 8 hours. There was an optional switch to oral therapy for patients who had clinical improvement as defined in the study protocol after a minimum of 5 days IV treatment. Total duration of antibiotic therapy (IV plus oral) was 10 days (optionally up to 14 if bacteraemic). The mMITT population included all patients with a confirmed cUTI diagnosis, received at least 1 dose of study treatment and had a study-qualifying pre-treatment urine culture containing 10
5 CFU/mL of a Gram-negative pathogen and no more than 2 species of microorganisms. Any patient with a Gram-positive pathogen, or a bacterial species not expected to respond to both study drugs was excluded.
The primary efficacy endpoint was per-patient microbiological response at the TOC visit in the mMITT analysis set. (See Table 6.)
Click on icon to see table/diagram/image
Favourable microbiological response rates at TOC by pathogen in the mMITT population are shown in Table 7 as follows. (See Table 7.)
Click on icon to see table/diagram/image
Among patients with baseline bacteraemia who were enrolled in any of the phase 3 cUTI studies (RECAPTURE or REPRISE), clinical cure at TOC in the subset of patients with bacteraemia due to aerobic Gram-negative pathogens was observed in 28/28 (100.0%) patients treated with CAZ-AVI and 25/29 (86.2%) patients treated with comparators (doripenem or best-available therapy). For the endpoint of per-patient microbiological response at TOC, a favourable response at TOC was reported in 26/28 (92.9%) patients treated with CAZ-AVI and 20/29 (69.0%) patients treated with comparator. The most commonly isolated pathogen was
E. coli. A total of 21/23 (91.3%) patients in the CAZ-AVI group and 19/23 (82.6%) in the comparator group had a favourable per-pathogen microbiological response for
E. coli, which was the most common pathogen.
Hospital-acquired pneumonia: A total of 808 adults with nosocomial pneumonia (35% with VAP) were randomised and received treatment in a phase III double-blind, comparative study of ceftazidime-avibactam (2 g/0.5 g) IV over 2 hours every 8 hours or meropenem 1 g IV over 30 mins every 8 hours. Treatment duration was 7 to 14 days. The clinically modified intent to treat (cMITT) population included patients who met the minimum disease criteria, received at least 1 dose of study treatment and who had properly obtained baseline respiratory or blood cultures demonstrating Gram-negative pathogens excluding patients with monomicrobial Gram-negative infections with species not expected to respond to both study drugs (e.g.
Acinetobacter species or
Stenotrophomonas species). The cMITT also included patients in whom no etiologic pathogens were identified from respiratory or blood cultures at baseline. The CE at TOC analyses set was the clinically evaluable subset of the cMITT.
The primary efficacy endpoint was the clinical response at the TOC visit in the co-primary populations of the cMITT and CE at TOC. See Table 8 as follows.
Click on icon to see table/diagram/image
All-cause mortality rates at Day 28 (cMITT) was 8.4% (30/356) and 7.3% (27/370) ceftazidime-avibactam and meropenem treated patients, respectively.
Clinical cure rate and favourable microbiological response rate at TOC by pathogen in mMITT for Gram-negative aerobes are shown in Tables 9 and 10. (See Tables 9 and 10.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For HAP/VAP patients enrolled with baseline bacteraemia, clinical cure at TOC in the subset of patients with bacteraemia due to aerobic Gram negative pathogens was observed in 10/15 (66.7%) patients treated with CAZ-AVI and 5/8 (62.5%) patients treated with meropenem. Although patient numbers were small for any given pathogen, favourable per-pathogen microbiological response rates in this sub-group were broadly similar to those of the overall population.
Among patients enrolled with baseline bacteraemia in the Phase 3 program across all indications combined (cIAI, cUTI or HAP/VAP), clinical cure at TOC in the subset of patients with bacteraemia due to aerobic Gram-negative pathogens was observed in 47/54 (87.0%) patients treated with CAZ-AVI ± MTZ and 39/47 (83.0%) patients treated with comparators. For the two most commonly occurring pathogens in this sub-group, a favourable per-pathogen microbiological response at TOC was reported in 32/37 (86.5%) CAZ-AVI ± MTZ and 29/33 (87.9%) comparator-treated patients with
E. coli bacteraemia; and 6/11 (54.5%) CAZ-AVI ± MTZ and 3/6 (50.0%) comparator-treated patients with
P. aeruginosa bacteraemia.
Paediatric population: Ceftazidime-avibactam has been evaluated in paediatric patients aged 3 months to <18 years in two Phase 2 single-blind, randomised, comparative clinical studies, one in patients with cIAI and one in patients with cUTI (Doses provided in Table 16). Patients aged ≥3 months to <1 year must have been born at term (defined as gestational age ≥37 weeks). Patients treated with ceftazidime-avibactam in the cIAI trial also received metronidazole (administered per local label; suggested dose: 10 mg/kg every 8 hours, administered IV over 20 to 30 minutes). The primary objective in each study was to assess safety and tolerability of ceftazidime-avibactam (+/- metronidazole). Secondary objectives included assessment of PK and efficacy; efficacy was a descriptive endpoint in both studies.
cIAI:
A total of 83 paediatric patients with cIAI were randomised (3:1) and received treatment with either ceftazidime-avibactam plus metronidazole (n=61) (doses provided in Table 16), or meropenem (n=22), 20 mg/kg IV every 8 hours. The paediatric age groups who received CAZ-AVI plus metronidazole were as follows: 12 to <18 years (n=22), 6 to <12 years (n=33), 3 to <6 years (n=6). No patients less than 2 years of age received CAZ-AVI plus metronidazole. After a minimum of 72 hours of IV treatment, there was an optional switch to oral therapy for patients who had clinical improvement, as defined in the study protocol. The total duration of antibiotic therapy (IV plus oral) was between 7 and 15 days. TOC assessments were performed 8 to 15 days after the last dose of study drug (IV or oral).
The majority of patients (87%) had appendiceal perforation or peri-appendiceal abscess (52/61, 85.2% ceftazidime-avibactam plus metronidazole; 20/22, 90.9% meropenem). The CE population included patients who had a confirmed diagnosis of cIAI and received a minimum duration of IV study drug, and excluded patients who had a clinical response of indeterminate and/or an important protocol deviation impacting the assessment of efficacy. The microbiological intent-to treat (micro-ITT) population included 69 patients (50 ceftazidime-avibactam plus metronidazole, 19 meropenem) who had at least one baseline intra-abdominal pathogen. Favourable clinical response rates at TOC are presented in Table 11. (See Table 11.)
Click on icon to see table/diagram/image
The predominant pathogens isolated at baseline were
E. coli (55/69, 79.7%) and
P. aeruginosa 23/69 (33.3%). Favourable clinical response rates at TOC by baseline pathogen in the micro-ITT population are presented in Table 12. (See Table 12.)
Click on icon to see table/diagram/image
cUTI: A total of 95 paediatric patients with cUTI were randomised (3:1) and received treatment with either ceftazidime-avibactam (n=67) (doses provided in Table 16), or cefepime (n=28), dosed per local prescribing information (maximum dose 2 g). The paediatric age groups who received CAZ-AVI were as follows: 12 to <18 years (n=13), 6 to <12 years (n=17), 2 to <6 years (n=11), 1 to <2 years (n=12), and 3 months to <1 year of age (n=14). After a minimum of 72 hours of IV treatment, there was an optional switch to oral therapy for patients who had clinical improvement, as defined in the study protocol. The total duration of antibiotic therapy (IV plus oral) was between 7 and 14 days. TOC assessments were performed 8 to 15 days after the last dose of study drug (IV or oral).
The majority of patients (83.2%) had acute pyelonephritis (55/67, 82.1% ceftazidime-avibactam; 24/28, 85.7% cefepime). The micro-ITT population included 77 randomised patients (54 ceftazidime-avibactam, 23 cefepime) who had at least 1 Gram-negative typical pathogen known to cause cUTI and no Gram-positive pathogen in the urine at baseline. Favourable clinical, microbiological and combined clinical and microbiological response rates at TOC in the micro-ITT population are presented in Table 13. (See Table 13.)
Click on icon to see table/diagram/image
The predominant baseline pathogen was
E. coli (71/77, 92.2%). Favourable microbiological response rates by baseline pathogen at TOC in the micro-ITT population are presented in Table 14. (See Table 14.)
Click on icon to see table/diagram/image
Pharmacokinetics: Distribution: The human protein binding of both ceftazidime and avibactam is low, approximately 10% and 8%, respectively. The steady-state volumes of distribution of ceftazidime and avibactam were comparable, about 17 L and 22 L, respectively in healthy adults following multiple doses of 2 g/0.5 g ceftazidime-avibactam infused over 2 hours every 8 hours.
Pharmacokinetic parameters of ceftazidime and avibactam following single and multiple dose administration of CAZ-AVI were similar to those determined when ceftazidime or avibactam were administered alone. Both ceftazidime and avibactam penetrate into human bronchial epithelial lining fluid (ELF) to the same extent with concentrations around 30% that of plasma, and a similar concentration time profile between ELF and plasma.
Ceftazidime and avibactam plasma exposure were comparable across patients with different indications, cIAI, cUTI and NP.
Penetration of ceftazidime into the intact blood-brain barrier is poor, resulting in low levels of ceftazidime in the CSF in the absence of inflammation. However, concentrations of 4 to 20 mg/L or more are achieved in the CSF when the meninges are inflamed. Avibactam penetration of the blood brain barrier has not been studied clinically, however, in rabbits with inflamed meninges, CSF exposures of ceftazidime and avibactam were 43% and 38% of plasma AUC, respectively. For ceftazidime, concentrations in excess of the MIC for common pathogens can be achieved in tissues such as bone, heart, bile, sputum, aqueous humour, synovial, pleural and peritoneal fluids. Ceftazidime crosses the placenta readily, and is excreted in the breast milk. Avibactam penetrates into the subcutaneous tissue at the site of skin infections, with tissue concentrations approximately equal to free drug concentrations in plasma.
Biotransformation: Ceftazidime is not metabolized. No metabolism of avibactam was observed in human liver preparations (microsomes and hepatocytes). Unchanged avibactam was the major drug-related component in human plasma and urine following dosing with [
14C]-avibactam.
Elimination: The terminal half-life (t½) of both ceftazidime and avibactam is about 2 h after IV administration. Ceftazidime is excreted unchanged into the urine by glomerular filtration; approximately 80 - 90% of the dose is recovered in the urine within 24 h. Avibactam is excreted unchanged into the urine with a renal clearance of approximately 158 mL/min, suggesting active tubular secretion in addition to glomerular filtration; approximately 97% of the dose is recovered in the urine, 95% within 12 h. Less than 1% of ceftazidime is excreted via the bile and less than 0.25% of avibactam is excreted into faeces.
Linearity/non-linearity: The pharmacokinetics of both ceftazidime and avibactam are approximately linear across the dose range studied (0.05 g to 2 g) for a single IV administration. No appreciable accumulation of ceftazidime or avibactam was observed following multiple IV infusions of 2 g/0.5 g of ceftazidime-avibactam administered every 8 hours for up to 11 days in healthy adults with normal renal function.
Special populations: Patients with renal impairment: Elimination of ceftazidime and avibactam is decreased in patients with moderate or severe renal impairment, and end stage renal disease including patients undergoing haemodialysis; the dose should be reduced in patients with CrCl ≤50 mL/min) (see Dosage & Administration).
Patients with hepatic impairment: Mild to moderate hepatic impairment had no effect on the pharmacokinetics of ceftazidime in individuals administered 2 g IV every 8 hours for 5 days, provided renal function was not impaired. The pharmacokinetics of ceftazidime in patients with severe hepatic impairment has not been established. The pharmacokinetics of avibactam in patients with any degree of hepatic impairment has not been studied.
As ceftazidime and avibactam do not appear to undergo significant hepatic metabolism, the systemic clearance of either drug is not expected to be significantly altered by hepatic impairment. Therefore, no dosage adjustment of ceftazidime-avibactam is recommended for patients with hepatic impairment (see Dosage & Administration).
Elderly patients: The reduced clearance observed in elderly patients was primarily due to age-related decrease in renal clearance of ceftazidime. The mean elimination half-life ranged from 3.5 to 4 hours following single or 7 days repeated every 12 hours dosing of 2 g IV bolus injections in elderly patients 80 years or older.
Following single dose IV administration of 0.5 g avibactam as a 30-minute IV infusion, the elderly had a slower terminal half-life of avibactam, which may be attributed to age related decrease in renal clearance. Dosage adjustment for ceftazidime-avibactam is not required in elderly subjects (≥65 years of age) with CrCl >50 mL/min.
Paediatric patients: The pharmacokinetics of ceftazidime and avibactam were evaluated in paediatric patients from 3 months to <18 years of age with suspected or confirmed infections following a single dose of ceftazidime 50 mg/kg and avibactam 12.5 mg/kg for patients weighing <40 kg or Zavicefta 2g/0.5g (ceftazidime 2 grams and avibactam 0.5 grams) for patients weighing ≥40 kg. Plasma concentrations of ceftazidime and avibactam were similar across all four age cohorts in the study (3 months to < 2 years, 2 to <6 years, 6 to <12 years, and 12 to <18 years). Ceftazidime and avibactam AUC
0-t and C
max values in the two older cohorts (children from 6 to <18 years), which had more extensive pharmacokinetic sampling, were similar to those observed in healthy adult subjects with normal renal function that received Zavicefta 2 g/0.5 g. Data from this study and the two Phase 2 paediatric studies in patients with cIAI and cUTI were pooled with PK data from adults (Phase 1 to Phase 3) to update the population PK model, which was used to conduct simulations to assess PK/PD target attainment. Results from these simulations demonstrated that the recommended dose regimens for paediatric patients with cIAI, cUTI and HAP/VAP, including dose adjustments for patients with renal impairment, result in systemic exposure and PK/PD target attainment values that are similar to those in adults at the approved Zavicefta dose of 2 g/0.5 g administered over 2 hours, every 8 hours.
There is limited experience with the use of ceftazidime plus avibactam in the paediatric groups of 3 months to <6 years. The recommended dosing regimens are based on simulations conducted using the final population PK models. Simulations demonstrated that the recommended dose regimens result in comparable exposures to other age groups with PK/PD target attainment >90%. Based on data from the completed paediatric clinical trials, at the recommended dose regimens, there was no evidence of over or under exposure in the subjects aged 3 months to <6 years.
In addition, there is very limited data in paediatric patients aged 3 months to <2 years with impaired renal function (CrCl ≤50 mL/min/1.73 m
2), with no data in severe renal impairment from the completed paediatric clinical trials. Population PK models for ceftazidime and avibactam were used to conduct simulations for patients with impaired renal function.
Gender: The pharmacokinetics of ceftazidime-avibactam was similar between males and females. No dose adjustment is required based on sex.
Race: Based on a population pharmacokinetic analysis, no dose adjustment of ceftazidime-avibactam is required based on race.
Toxicology: Preclinical safety data: Genetic toxicology: For ceftazidime a mouse Micronucleus test and an Ames test were both negative for mutagenic effects. Carcinogenicity studies have not been conducted. In genotoxicity assays with avibactam, there was no induction of gene mutation in the
in vitro bacterial reverse mutation tests, nor were there any indications of genotoxicity in an
in vitro unscheduled DNA synthesis test in rat liver cells or an
in vitro micronucleus test in mouse lymphoma cells. In cultured human lymphocytes, statistically significant increases in chromosomal aberrations were observed under a single treatment condition (44h harvest time, -S9). As these findings were not replicated in an independent study, the results are considered to be of limited biological relevance. When administered up to the limit dose of 2 g/kg IV, avibactam was negative in a rat
in vivo micronucleus assay. Carcinogenicity studies have not been conducted. No genetic toxicology studies have been conducted on ceftazidime-avibactam.
Reproductive toxicology: Reproduction studies have been performed with ceftazidime in mice and rats at doses up to 40 times the human dose and have revealed no evidence of impaired fertility or harm to the fetus. A slightly increased post-implantation loss was observed at avibactam dose of 1000 mg/kg/day and lower mean fetal weight with slightly retarded ossification of a small number of bones was observed at avibactam doses of 300 mg/kg/day and above in pregnant rabbits. In the rat, no adverse effects were observed on embryofetal development or fertility. Following administration of avibactam throughout pregnancy and lactation in the rat, there was no effect on pup survival, growth or development, however there was an increase in incidence of dilation of the renal pelvis and ureters in less than 10% of the rat pups at maternal exposures greater than or equal to approximately 1.5 times human therapeutic exposures. No reproductive toxicology studies have been conducted on ceftazidime-avibactam.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image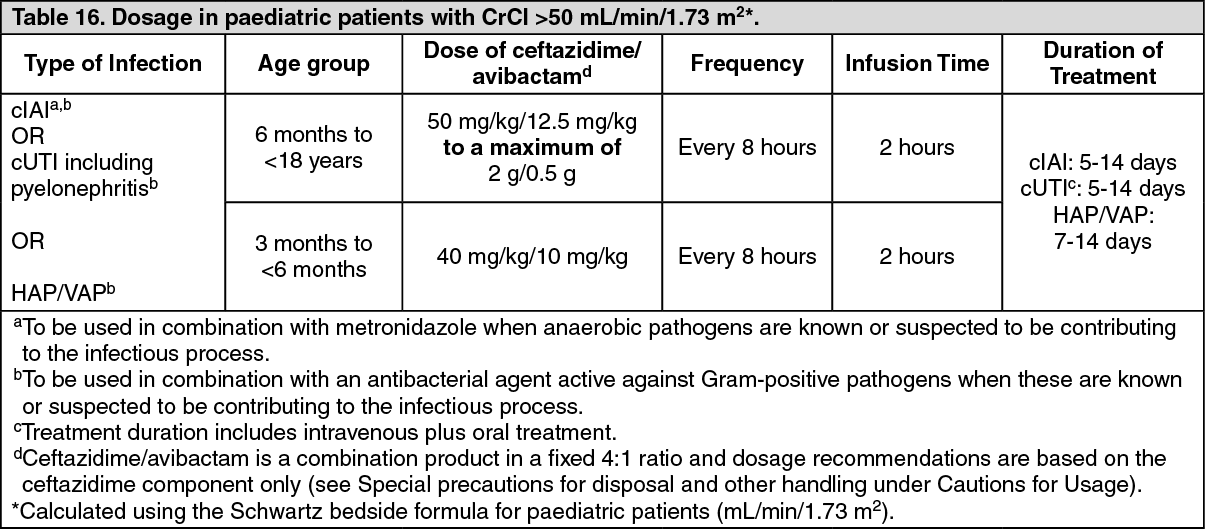 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image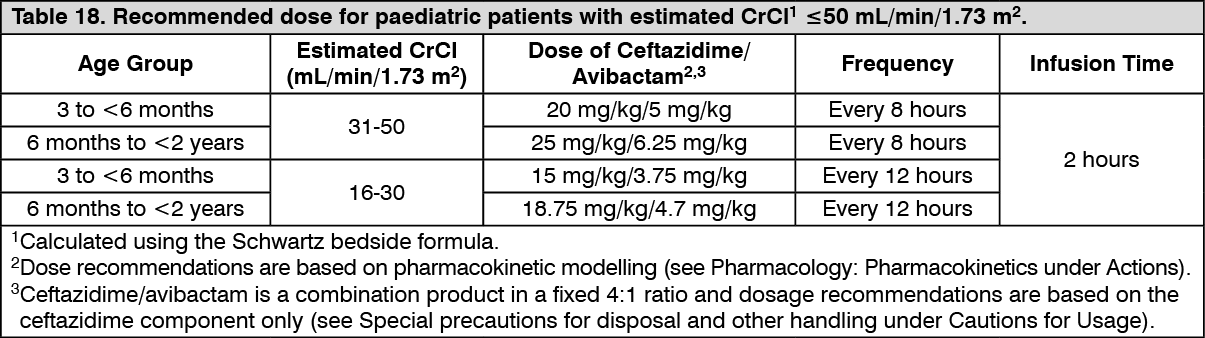 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
