


 Sign Out
Sign Out


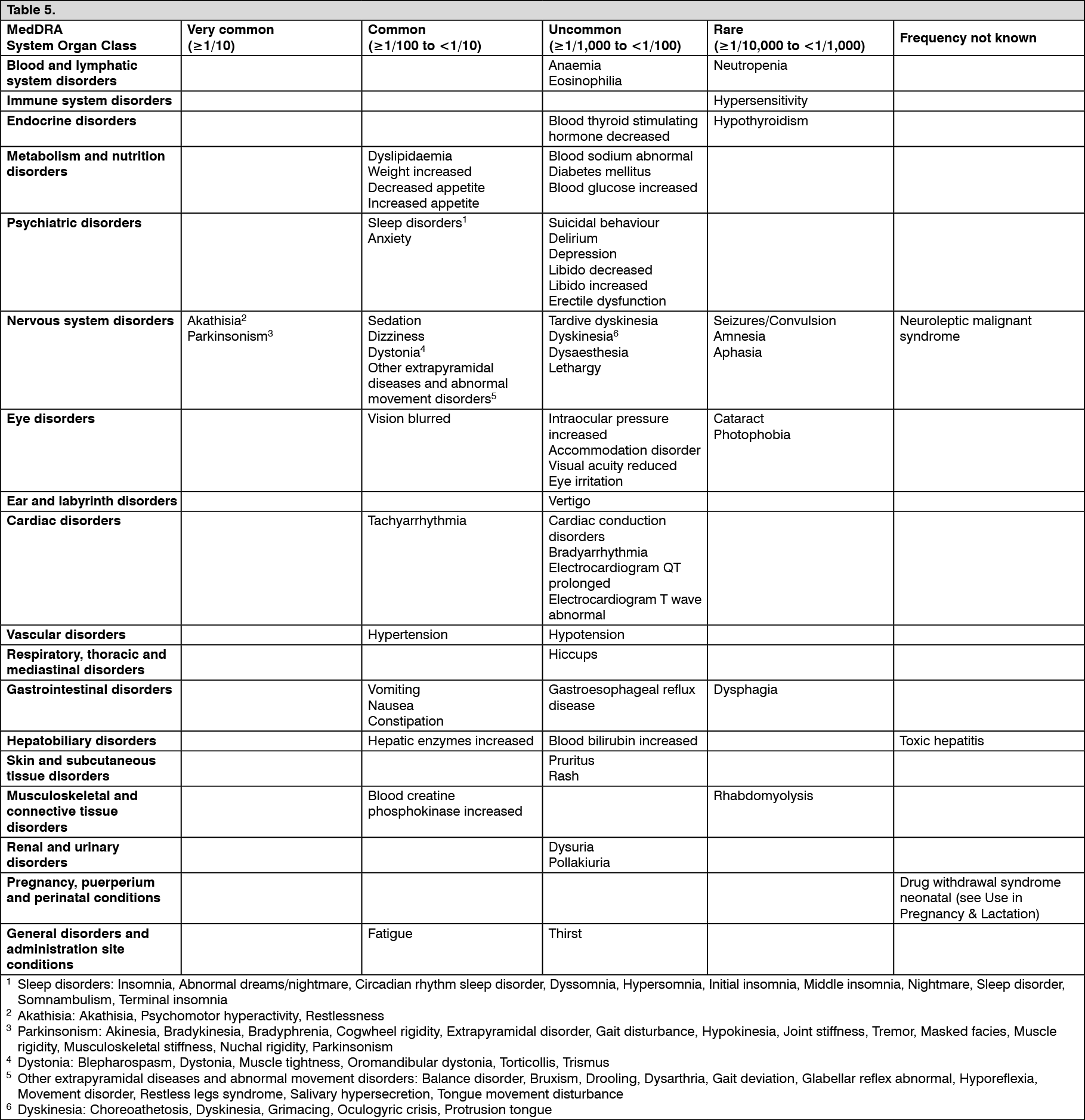
Tabulated list of adverse reactions: ADRs are shown by indication, system organ class and by preferred term.
Adverse reactions are ranked by frequency, the most frequent first, using the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000) very rare (<1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness.
Schizophrenia: The safety profile of cariprazine has been evaluated in around 2000 cariprazine-treated patients with schizophrenia in therapeutic dose range from 1.5 mg to 6 mg based on several short-term and long-term clinical studies. (See Table 5.)
 Click on icon to see table/diagram/image
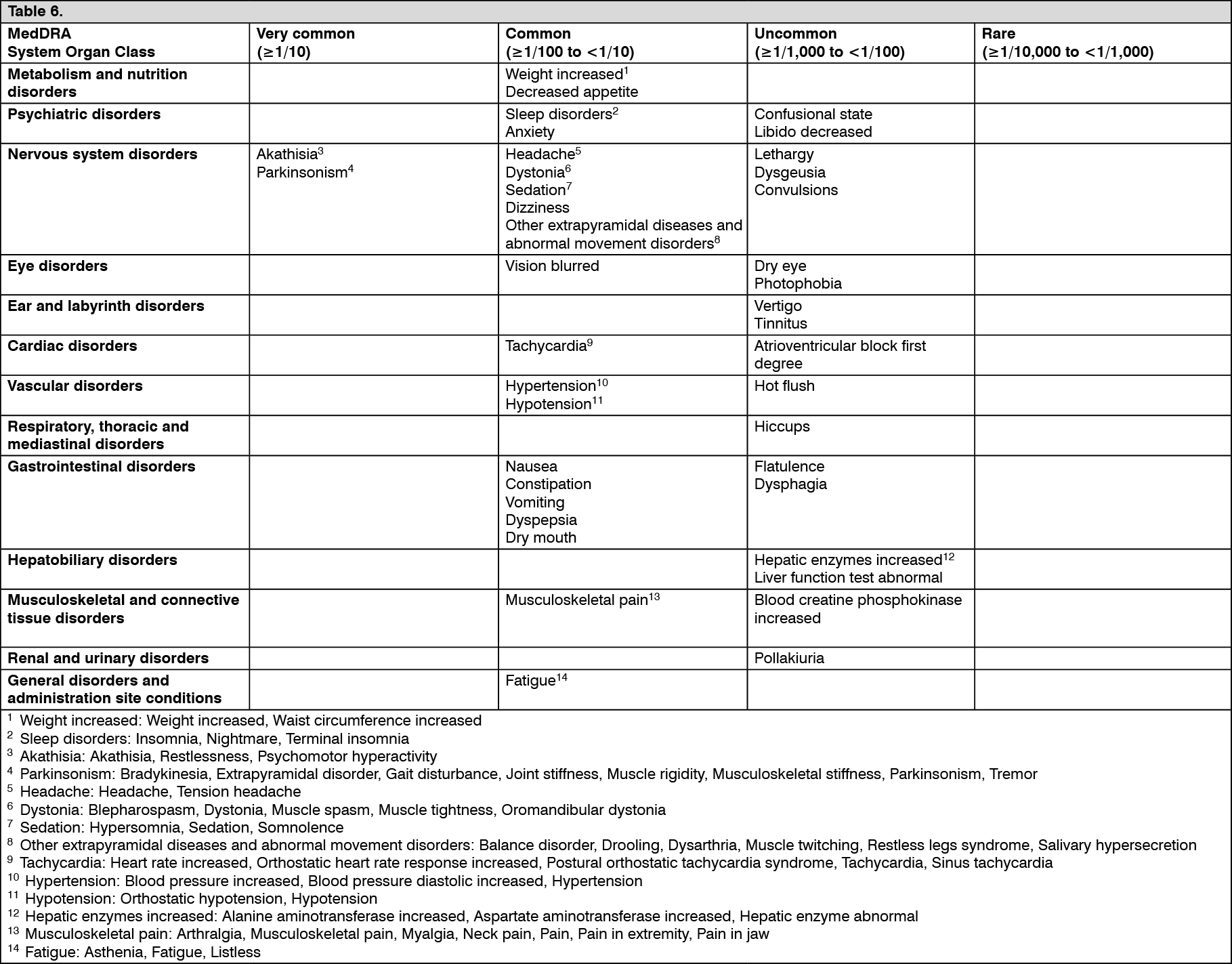
Click on icon to see table/diagram/imageManic or mixed episodes associated with Bipolar I disorder: The safety profile of cariprazine has been evaluated in around 500 cariprazine-treated patients with manic or mixed episodes associated with Bipolar I disorder in therapeutic dose range from 3 mg to 6 mg based on several short-term and one long-term clinical studies. (See Table 6.)
 Click on icon to see table/diagram/image
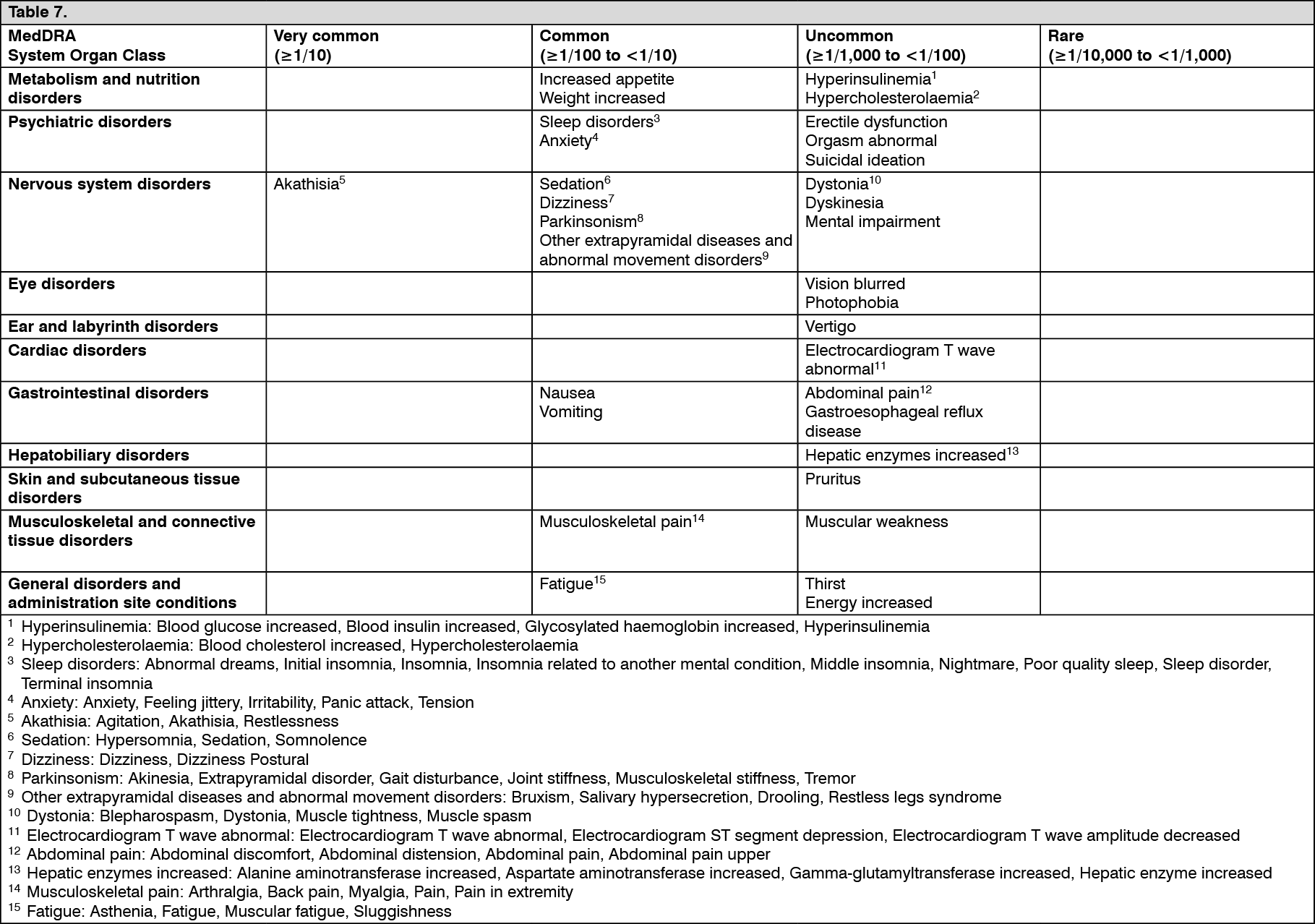
Click on icon to see table/diagram/imageBipolar Depression: The safety profile of cariprazine has been evaluated in around 1,000 cariprazine-treated patients with bipolar depression in therapeutic dose range from 1.5 mg to 3 mg based on studies. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Lens opacity/Cataract: Development of cataracts was observed in cariprazine non-clinical studies (see Pharmacology: Toxicology under Actions). Therefore, cataract formation was closely monitored with slit lamp examinations in the clinical studies and patients with existing cataracts were excluded. During the schizophrenia clinical development program of cariprazine, few cataract cases were reported, characterized with minor lens opacities with no visual impairment (13/3192; 0.4%). Some of these patients had confounding factors. The most commonly reported ocular adverse event was blurred vision (placebo: 1/683; 0.1%, cariprazine: 22/2048; 1.1%). In the short-term bipolar mania and depression studies the most commonly reported ocular adverse event was also blurred vision (placebo: 5/433; 1,2%, cariprazine 10/255; 3,9% and placebo 2/545; 0,4%, cariprazine 11/1014; 1,1% respectively). In the pooled mania studies the most commonly reported ocular adverse event was also blurred vision (17/485; 3,5%). No adverse event of cataract in the therapeutic dose range were reported in bipolar mania nor in bipolar depression studies.
Extrapyramidal symptoms (EPS): In the short-term schizophrenia studies the incidence of EPS was observed in 27%; 11.5%; 30.7% and 15.1% in patients treated with cariprazine, placebo, risperidone and aripiprazole respectively. Akathisia was reported in 13.6%; 5.1%; 9.3% and 9.9% in patients treated with cariprazine, placebo, risperidone and aripiprazole respectively. Parkinsonism was experienced in 13.6%; 5.7%; 22.1% and 5.3% in patients treated with cariprazine, placebo, risperidone and aripiprazole respectively. Dystonia was observed in 1.8%; 0.2%; 3.6% and 0.7% in patients on cariprazine, placebo, risperidone and aripiprazole, respectively.
In the placebo-controlled part of the long-term maintenance of effect study in schizophrenia EPS was 13.7% in the cariprazine group compared to 3.0% in the placebo treated patients. Akathisia was reported in 3.9% in patients treated with cariprazine, versus 2.0% in the placebo group. Parkinsonism was experienced in 7.8% and 1.0% in cariprazine and placebo group respectively.
In the schizophrenia negative symptom study EPS was reported in 14.3% in the cariprazine group and 11.7% in the risperidone treated patients. Akathisia was reported in 10.0% in patients treated with cariprazine and 5.2% in the risperidone group. Parkinsonism was experienced in 5.2% and 7.4% in cariprazine and risperidone treated patients respectively. Most EPS cases were mild to moderate in intensity and could be handled with common anti-EPS medicinal products. The rate of discontinuation due to EPS related ADRs was low.
In 3-week bipolar mania studies, the incidence of reported adverse drug reactions related to extrapyramidal symptoms (EPS), excluding akathisia and restlessness, was 27.5% for cariprazine-treated patients versus 11.3% for placebo treated patients. The incidence of akathisia and restlessness was 23.5% for cariprazine treated patients versus 5.5% for placebo-treated patients. The incidence of parkinsonism was 18.4% for cariprazine treated patients versus 8.6% for placebo treated patients.
In the controlled bipolar depression studies, the incidence of reported adverse drug reactions related to EPS was 16.3% for cariprazine-treated patients versus 7.3% for placebo-treated patients. Akathisia was reported in 13.4% in patients treated with cariprazine and 6.4% in the placebo group. Parkinsonism was experienced in 3.1% and 1.7% in cariprazine and placebo-treated patients respectively.
Venous thromboembolism (VTE): Cases of VTE, including cases of pulmonary embolism and cases of deep vein thrombosis have been reported with antipsychotics - Frequency unknown.
Elevated liver transaminases: Elevated liver transaminases (Alanine Aminotransferase [ALT], Aspartate Aminotransferase [AST]) are frequently observed with antipsychotic treatment. In the cariprazine clinical studies in schizophrenia the incidence of ALT, AST elevation adverse events occurred in 2.2% of cariprazine-, 1.6% of risperidone- and 0.4% of placebo-treated patients. None of the cariprazine-treated patients hadany liver damage.
In mania studies the incidence of hepatic enzymes increased related adverse events was 1.7% in cariprazine group and 1.2% in placebo group. In bipolar depression studies the incidence of hepatic enzymes increased related adverse events was 1.3% in cariprazine group and 0.7% in placebo group.
Weight changes: In the short-term studies, there were slightly greater mean increases in body weight in the cariprazine group compared to the placebo group; 1 kg and 0.3 kg, respectively. In the long term maintenance of effect study in schizophrenia, there was no clinically relevant difference in change of body weight from baseline to end of treatment (1.1 kg for cariprazine and 0.9 kg for placebo). In the open-label phase of the study during 20 weeks cariprazine treatment 9.0% of patients developed potentially clinically significant (PCS) weight gain (defined as increase ≥7%) while during the double-blind phase, 9.8% of the patients who continued with cariprazine treatment had PCS weight gain versus 7.1% of the patients who were randomized to placebo after the 20 week open-label cariprazine treatment. In the negative symptom study, the mean change of body weight was -0.3 kg for cariprazine and +0.6 kg for risperidone and PCS weight gain was observed in 6% of the cariprazine group while 7.4% of the risperidone group.
In short-term mania studies the mean change of body weight was similar in placebo and cariprazine group +0.2 kg and +0.5 kg respectively. In long-term mania study, the mean change from baseline to endpoint in body weight was approximately 1 kg. 9.3% of patients had PCS weight gain (≥7% increase from baseline) in the long-term mania study.
In bipolar depression studies the mean change of body weight was no clinically relevant difference in change of body weight from baseline to end of treatment (-0.1 kg for placebo, 0.7 kg for cariprazine 1.5 mg, and 0.4 kg for cariprazine 3 mg).
QT-prolongation: With cariprazine no QT interval prolongation was detected compared to placebo in a clinical study designed to assess QT prolongation (see Pharmacology: Pharmacodynamics under Actions). In other clinical studies, only a few, non-serious, QT-prolongations have been reported with cariprazine. During the long-term, open-label treatment period in, 3 patients (0.4%) had QTcB >500 msec, one of whom also had QTcF >500 msec. A >60 msec increase from baseline was observed in 7 patients (1%) for QTcB and in 2 patients (0.3%) for QTcF. In the long-term, maintenance of effect study in schizophrenia, during the open-label phase, >60 msec increase of from baseline was observed in 12 patients (1.6%) for QTcB and in 4 patients (0.5%) for QTcF. During the double-blind treatment period, >60 msec increases from baseline in QTcB were observed in 3 cariprazine-treated patients (3.1%) and 2 placebo-treated patients (2%). In short-term mania studies one patient in the cariprazine group and 2 patients in the placebo group had a postbaseline QTcB interval value >500 msec. No patient had a QTcF interval >500 msec. In long-term mania studies, no cariprazine-treated patient had a postbaseline QTcB or QTcF interval >500 msec. No serious adverse events associated with ECG findings were reported.
In bipolar depression studies few patients in both the cariprazine modal daily dose groups and the placebo treatment group had QTcB and QTcF increases >60 msec from baseline to any time during the double-blind treatment period: overall cariprazine 0.9% (10/1167) versus placebo 0.4% (2/510) and overall cariprazine 0.2% (2/1167) versus placebo 0% (0/510), respectively.
View ADR Monitoring Form