Pharmacotherapeutic group: Intestinal antiinflammatory agents; aminosalicylic acid and similar agents.
ATC code: A07EC02.
Pharmacology: Pharmacodynamics: Mechanism of action: The mechanism of the anti-inflammatory action is unknown. The results of in-vitro studies indicate that inhibition of lipoxygenase may play a role. Effects on prostaglandin concentrations in the intestinal mucosa have also been demonstrated. Mesalazine (5-aminosalicylic acid/5-ASA) may also function as a radical scavenger of reactive oxygen compounds.
Pharmacodynamic effects: Gastro-resistant tablet & Gastro-resistant prolonged-release granules: Mesalazine, orally administered, acts predominantly locally at the gut mucosa and in the submucous tissue from the luminal side of the intestine. It is important, therefore, that mesalazine is available at the regions of inflammation. Systemic bioavailability/plasma concentrations of mesalazine therefore are of no relevance for therapeutic efficacy, but rather a factor for safety.
Gastro-resistant tablet: In order to fulfil these criteria, Salofalk tablets are coated with Eudragit L; they are thus gastro-resistant and the release of mesalazine is pH-dependent.
Gastro-resistant prolonged-release granules: In order to realise this, Salofalk granules are gastric juice resistant and release mesalazine in a pH dependent manner, due to an Eudragit L coating, and prolonged manner, due to the matrix granule structure.
Suppository/Enema: On reaching the intestinal lumen, rectally administered mesalazine has largely local effects on the intestinal mucosa and submucosal tissue.
Clinical trial information: Gastro-resistant prolonged-release granules: The criteria used to evaluate the efficacy of the substance in the therapy of ulcerative colitis are frequency of bowel movements, rectal haemorrhage, abdominal pain, general well-being, temperature, extraintestinal manifestations, ESR, and haemoglobin. These criteria have been summarised in the clinical activity index (CAI) to evaluate the efficacy of treatment for ulcerative colitis.
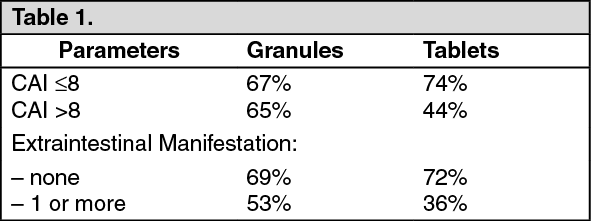
The safety and efficacy of Salofalk granules (1.5 g to 3 g 5-ASA/day) was compared against mesalazine tablets (Salofalk 500 mg tablets, 1.5 g to 3.0 g 5-ASA/day) in a double-blind randomised multi-centre study in 233 patients with mild to moderately active ulcerative colitis over a period of 8 weeks. The primary efficacy criterion, complete response rate (per protocol analysis, PP) was very similar in the granules (68%) and the tablets (70%) groups. The efficacy analysis (PP) showed that more patients treated with mesalazine tablets (47%) had to increase the dose from 1.5 g mesalazine/day to 3.0 g mesalazine/day compared to patients treated with granules (38%). Similar results were obtained by the ITT (intention-to-treat) analysis: 39% of the granules group, 45% of the tablets group, i.e., more patients came into remission (49%) with the 1.5 g 5-ASA/day from granules than from tablets (43%). Granules, therefore, in total were at least as efficacious and as well tolerated as the tablets at the same dose. Subgroup analyses showed that the response rates to granules were higher in patients with high baseline disease activity (CAI>8) and with 1 or more extraintestinal manifestations than the tablets: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In another study, the efficacy and safety of Salofalk granules of different dosages (1.5 g, 3.0 g, 4.5 g/day) were compared in 321 patients with mild to moderately active ulcerative colitis in a double-blind manner for a treatment period of 8 weeks. Complete response (CAI ≤ 4) was obtained by 50% in the 1.5 g dose group, by 66% in the 3.0 g group (in comparison to 1.5 g: p = 0.014) and by 55% in the 4.5 g group (in comparison to 1.5 g: not significant, p=0.318). The 3.0 g/day dose appears to be the optimal dose.
In a double-blind, randomised comparative study, the efficacy and tolerability of once daily (o.d.) 3.0 g Salofalk granules was compared with three time daily (t.i.d.) 1.0 g Salofalk granules in 380 patients with active ulcerative colitis over a period of eight weeks. The data show that for Salofalk granules, a daily dose of 3 g mesalazine given o.d. is therapeutically equivalent to the conventional t.i.d. dosage regimen for the induction of remission (CAI ≤ 4) in patients with mild-to-moderate ulcerative colitis. The clinical remission rate in the PP analysis set (primary analysis) was 84.4% in the o.d. group and 81.3% in the t.i.d. group. The resulting p-value for the noninferiority test (pre-defined margin: -15%) was 0.0007 with a 95% CI of [-11.4%, 17.6%]. Remission rates in ITT analysis set were very similar, 80.8% in the o.d. group and 77.4% in the t.i.d. group. ITT test result (p = 0.0007) and 95% CI (-11.4%, 18.1%) agreed with the PP analysis. Once daily dosing of Salofalk granules was as safe and well tolerated as three times daily dosing of Salofalk granules.
Results of the various studies show that oral delayed release Salofalk granules are well tolerated in patients with ulcerative colitis.
Pharmacokinetics: General aspects/considerations of mesalazine: Absorption: Mesalazine absorption is highest in the proximal gut regions and lowest in distal gut areas.
Biotransformation: Mesalazine is metabolised both pre-systemically by the intestinal mucosa and the liver to the pharmacologically inactive N-acetyl-5-aminosalicylic acid (N-Ac-5-ASA). The acetylation seems to be independent of the acetylator phenotype of the patient. Some acetylation also occurs through the action of colonic bacteria. Protein binding of mesalazine and N-Ac-5-ASA is 43% and 78%, respectively.
Elimination: Mesalazine and its metabolite N-Ac-5-ASA are eliminated via the faeces (major part), renally (varies between 20% and 50%, dependent on kind of application, pharmaceutical preparation and route of mesalazine release, respectively) and biliary (minor part). Renal excretion predominantly occurs as N-Ac-5-ASA. About 1% of total orally administered mesalazine dose is excreted into breast milk, mainly as N-Ac-5-ASA.
Salofalk 500 mg tablets specific: Distribution: A combined pharmacoscintigraphic/pharmacokinetic study showed that Salofalk 500 mg, gastro-resistant tablets, reach the ileocoecal region after approximately 3-4 hours in fasting subjects and reach the ascending colon within approximately 4-5 hours. The total transit time in the colon is approximately 17 hours.
Absorption: Release of mesalazine from Salofalk 500 mg, gastro-resistant tablets, begins after a lag-phase of approximately 3-4 hours. Peak plasma concentrations are reached after approximately 5 hours (ileocoecal region) and, at 3 x 500 mg mesalazine/day under steady-state conditions, are 3.0 ± 1.6 μg/ml for mesalazine and 3.4 ± 1.6 μg/ml for the metabolite, N-Ac-5-ASA.
Elimination: The total renal elimination rate for mesalazine and N-Ac-5-ASA over 24 hours during multiple intake (3 x 1 Salofalk 500 mg, gastro-resistant tablets, for 2 days; 1 gastro-resistant tablet on the third day = examination day) was approximately 60%. The non-metabolised mesalazine fraction after oral administration was approximately 10%.
Salofalk suppositories specific: Distribution: Scintigraphic studies with technetium-labelled Salofalk 500 mg suppositories showed peak spread of the suppository that had melted due to body temperature after 2 - 3 hours. The spread was limited primarily to the rectum and rectosigmoid junction. Salofalk suppositories are thus particularly suitable for treating proctitis (ulcerative colitis of the rectum).
Absorption:
After both a single administration and after several weeks of long-term treatment with 500 mg mesalazine three times daily as Salofalk suppositories, peak plasma concentrations of 5-ASA were in the range of 0.1 to 1.0 μg/ml, those of the main metabolite N-Ac-5-ASA were in the range of 0.3 to 1.6 μg/ml. Peak plasma concentrations of 5-ASA are partially reached within the first hour of application.
Elimination: After a single rectal dose of 500 mg mesalazine as Salofalk suppositories approx. 11% (within 72 hours) was recovered in the urine, and after several weeks of long-term treatment with 500 mg mesalazine three times daily as Salofalk suppositories, approx. 13% of the 5-ASA dose administered was recovered in the urine. Approximately 10% of a single administered dose was eliminated via the bile.
Salofalk 2 g/30 ml/4 g/60 ml enemas specific: Distribution: An imaging study in patients with mild-to-moderate acute ulcerative colitis showed that the rectal suspension at the start of treatment and at remission after 12 weeks is distributed mainly in the rectum and sigmoid colon and to a lesser extent in the descending colon.
Absorption and elimination: No specific pharmacological studies on Salofalk 2 g/30 ml enemas are available.
In a study with Salofalk 4 g/60 ml enemas in ulcerative colitis patients in remission, peak plasma concentrations of 0.92 μg/ml 5-ASA and 1.62 μg/ml N-Ac-5-ASA were achieved after approximately 11-12 hours under steady-state conditions. The elimination rate was approximately 13% (45-hour value), with most (approximately 85%) being eliminated in the form of the metabolite, N-Ac-5-ASA.
The steady-state plasma concentrations of 5-ASA and N-Ac-5-ASA in children with chronic inflammatory bowel disease under treatment with Salofalk 2 g/30 ml enemas were 0.2-1.0 μg/ml and 0.4-2.0 μg/ml respectively whereas with Salofalk 4 g/60 ml enemas were 0.5-2.8 μg/ml and 0.9-4.1 μg/ml respectively.
Salofalk granules specific: Distribution: Owing to the granule size of approx. 1 mm, transit from the stomach to the small intestine is fast.
A combined pharmacoscintigraphic/pharmacokinetic study showed that the compound reaches the ileocaecal region within approx. 3 hours and the ascending colon within approx. 4 hours. The total transit time in the colon amounts to about 20 hours.
Approximately 80% of an administered oral dose is estimated to be available in the colon, sigmoid colon and rectum.
Absorption: Mesalazine release from Salofalk granules starts after a lag phase of about 2-3 hours. Peak plasma concentrations are reached at about 4-5 hours. The systemic bioavailability of mesalazine after oral administration is estimated to be approximately 15-25%.
Food intake delays absorption by 1 to 2 hours but does not change the rate and extent of absorption.
Elimination: From a 3 x 500 mg daily mesalazine dose in long-term therapy, a total renal elimination of mesalazine and N-Ac-5-ASA under steady state conditions was calculated to be about 25%. The unmetabolised excreted mesalazine part was less than 1% of the oral dose. The elimination half-life in this study was 4.4 hours.
Toxicology: Preclinical safety data: Preclinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, genotoxicity, carcinogenicity (rat) or toxicity to reproduction. Kidney toxicity (renal papillary necrosis and epithelial damage of the proximal tubule (pars convoluta) or the whole nephron) has been seen in repeat-dose toxicity studies with high oral doses of mesalazine. The clinical relevance of this finding is unknown.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out
