Adult: Treatment of extensively drug-resistant, treatment-intolerant, or nonresponsive multidrug-resistant pulmonary tuberculosis in combination with bedaquiline and linezolid: 200 mg once daily for 26 weeks. Duration of therapy may be extended beyond 26 weeks as necessary. The entire combination regimen must be discontinued if either bedaquiline or pretomanid is discontinued for any reason or if linezolid is permanently discontinued during the initial 4 consecutive weeks of treatment. Consequently, if linezolid is discontinued after the initial 4 weeks of consecutive treatment, the regimen may be continued with only bedaquiline and pretomanid.
Administration
Should be taken with food. Swallow whole w/ water.
Contraindications
Hypersensitivity. Patient for whom bedaquiline and/or linezolid are contraindicated.
Special Precautions
Patient at risk of QT prolongation (e.g. history of torsades de pointes, congenital long QT syndrome, hypothyroidism, bradyarrhythmia, uncompensated heart failure, hypocalcaemia, hypomagnesaemia, hypokalaemia). Hepatic impairment. Pregnancy and lactation.
Adverse Reactions
Significant: QT prolongation, hepatotoxicity, myelosuppression (e.g. anaemia, leucopenia, pancytopenia, neutropenia, thrombocytopenia), peripheral or optic neuropathy, and lactic acidosis. Cardiac disorders: Palpitations, sinus tachycardia. Ear and labyrinth disorders: Deafness. Eye disorders: Visual impairment, eye pain or irritation. Gastrointestinal disorders: Nausea, vomiting, diarrhoea, constipation, dyspepsia, abdominal pain, GERD, gastritis, pancreatitis, abdominal distension, haematemesis, dysgeusia. General disorders and administration site conditions: Fatigue, asthenia, malaise. Hepatobiliary disorders: Hyperbilirubinaemia, hepatomegaly, jaundice. Infections and infestations: Fungal infection, oral candidiasis, oral fungal infection. Investigations: Increased transaminases, GGT, amylase, lipase, alkaline phosphatase, creatine phosphokinase, urea, creatinine, uric acid, weight loss. Metabolism and nutrition disorders: Hypoglycaemia, decreased appetite, acidosis, dehydration, hypocalcaemia, hypovolaemia, hypomagnesaemia. Musculoskeletal and connective tissue disorders: Musculoskeletal pain, spasms, stiffness. Nervous system disorders: Headache, dizziness, seizure. Psychiatric disorders: Insomnia, anxiety, depression. Reproductive system and breast disorders: Erectile dysfunction, metrorrhagia. Respiratory, thoracic and mediastinal disorders: Cough, epistaxis, pleuritic chest pain, haemoptysis, lower respiratory tract infection. Skin and subcutaneous tissue disorders: Acne, pruritus, xeroderma, rash, dry skin, alopecia, allergic dermatitis, skin hyperpigmentation. Vascular disorders: Hypotension or hypertension.
Patient Counseling Information
This drug may occasionally cause dizziness and visual impairment, if affected, do not drive or operate machinery.
Monitoring Parameters
Monitor ECG prior to initiation of treatment, then at 2, 12, and 24 weeks after starting treatment; CBC, LFTs (e.g. ALT, AST, alkaline phosphatase, bilirubin) at baseline, at 2 weeks, and then monthly during the treatment; serum Ca, Mg, and K at baseline (repeat if with QT prolongation). Assess for lactic acidosis; monitor bicarbonate and lactic acid levels in patient with recurrent nausea or vomiting. Monitor for signs and symptoms of hepatotoxicity (e.g. nausea, anorexia, fatigue, dark urine, elevations of LFTs, hepatomegaly, liver tenderness, jaundice). Monitor visual function.
Drug Interactions
Reduced systemic exposure with moderate or strong CYP3A4 inducers (e.g. carbamazepine, phenytoin, efavirenz, etravirine, rifampicin, rifapentine, rifabutin). May reduce the efficacy of CYP2C8, 2C9, and 2C19 substrates (e.g. mephenytoin, paclitaxel, warfarin). May increase the concentrations of OAT3 substrates (e.g. benzylpenicillin, ciprofloxacin, indometacin, methotrexate) leading to enhanced adverse effects. May increase the exposure of sensitive OATP1B3 substrates (e.g. valsartan, statins), BCRP substrates (e.g. glyburide, prazosin, rosuvastatin, sulfasalazine), and P-gp substrates (e.g. dabigatran, digoxin, etexilate, verapamil).
Food Interaction
Food, particularly high-fat or high-caloric meals, increases peak plasma concentration and AUC. Increased hepatotoxic effect with alcohol. Reduced systemic exposure with St. John’s wort.
Action
Description: Mechanism of Action: Pretomanid, a nitroimidazooxazine antimycobacterial which inhibits mycolic acid biosynthesis, and blocking of the cell wall production, resulting in cell death of actively replicating Mycobacterium tuberculosis. It acts as a respiratory poison against nonreplicating bacteria under anaerobic conditions following nitric oxide release. Pharmacokinetics: Absorption: Food, particularly high-fat or high-caloric meal, increases peak plasma concentration and AUC. Time to peak plasma concentration: 4.5 hours. Distribution: Plasma protein binding: Approx 86.4%. Metabolism: Metabolised via multiple reductive and oxidative pathways; partially metabolised by CYP3A4 (approx 20%). Excretion: Via urine (53%, primarily as metabolites; approx 1% as unchanged drug); faeces (38%, primarily as metabolites). Elimination half-life: 16 hours.
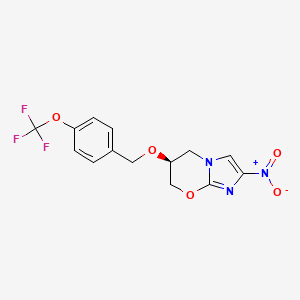
Chemical Structure
Pretomanid Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 456199, Pretomanid. https://pubchem.ncbi.nlm.nih.gov/compound/Pretomanid. Accessed Feb. 23, 2024.
J04AK08 - pretomanid ; Belongs to the class of other drugs used in the systemic treatment of tuberculosis.
References
Anon. Pretomanid. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 20/11/2023.Anon. Pretomanid. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 20/11/2023.Dovprela 200 mg Tablet (Mylan Products Ltd). MHRA. https://products.mhra.gov.uk. Accessed 20/11/2023.Pretomanid Tablet (Mylan Specialty L.P.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 20/11/2023.Pretomanid. Gold Standard Drug Database in ClinicalKey [online]. Elsevier Inc. https://www.clinicalkey.com. Accessed 20/11/2023.



 Sign Out
Sign Out