


 Sign Out
Sign Out


Clinical experience: Pharmacokinetics and Safety of NOXAFIL Delayed Release Tablets in Patients: Study 5615 was a non-comparative multi-center study performed to evaluate the pharmacokinetic properties, safety, and tolerability of posaconazole tablet. Study 5615 was conducted in a similar patient population to that previously studied in the pivotal posaconazole oral suspension clinical program. The pharmacokinetics and safety data from Study 5615 were bridged to the existing data (including efficacy data) with the oral suspension.
Study 5615 enrolled a total of 230 subjects. Part 1 of the study was designed to select a dose for further study in Part 2, after first evaluating pharmacokinetics, safety, and tolerability in the neutropenic patient population at high risk of a fungal infection. Part 2 of the study was designed to evaluate posaconazole tablet in a more diverse patient population, and to confirm the exposure of posaconazole tablet in additional subjects at risk of a fungal infection. Posaconazole tablet was administered without regard to food intake in both Part 1 and Part 2 of the study.
The subject population for Part 1 included subjects with acute myelogenous leukemia (AML) or myelodysplastic syndrome (MDS) who had recently received chemotherapy and had developed or were anticipated to develop significant neutropenia. Two different dosing groups were evaluated in Part 1: 200 mg BID on Day 1, followed by 200 mg QD thereafter (Part 1A) and 300 mg BID on Day 1, followed by 300 mg QD thereafter (Part 1B).
The subject population in Part 2 included: 1) patients with AML or MDS who had recently received chemotherapy and had developed or were anticipated to develop significant neutropenia, or 2) patients who had undergone a HSCT and were receiving immunosuppressive therapy for prevention or treatment of GVHD. These types of patients had been previously studied in a pivotal controlled trial of posaconazole oral suspension. Based on the pharmacokinetics and safety results of Part 1, all subjects in Part 2 received 300 mg BID on Day 1, followed by 300 mg QD thereafter.
The total subject population had a mean age of 51 years (range = 19-78 years), 93% were White, the major ethnicity was not Hispanic or Latino (84%), and 62% were male. The study treated 110 (48%) subjects with AML (new diagnosis), 20 (9%) subjects with AML (first relapse), 9 (4%) subjects with MDS, and 91 (40%) subjects with HSCT, as the primary diseases at study entry.
Serial PK samples were collected on Day 1 and at steady-state on Day 8 for all Part 1 subjects and a subset of Part 2 subjects. This serial PK analysis demonstrated that 90% of the subjects treated with the 300 mg QD dose attained steady state Cav between 500-2500 ng/mL. [Cav was the average concentration of posaconazole at steady state, calculated as AUC/dosing interval (24 hours).] Subjects with AML/MDS with neutropenia following chemotherapy or HSCT subjects receiving immunosuppressive therapy to prevent or treat GVHD who received 300 mg QD achieved a mean Cav at steady state of 1580 ng/mL. The PK findings from the pivotal study (Study 5615) support a 300 mg daily dose of posaconazole tablet for use in prophylaxis.
Pharmacokinetics and Safety of NOXAFIL Oral Suspension in Patients: Other serious fungal pathogens: NOXAFIL oral suspension has been shown to be effective against the following additional pathogens when other therapy had been ineffective or when the patient had developed intolerance of the prior therapy: Zygomycosis: Successful responses to NOXAFIL oral suspension therapy were noted in 7/13 of patients with zygomycete infections. Sites of infection included the sinuses, lung, and skin. Most of the patients had underlying haematological malignancies, half of which required a bone marrow transplant. One-half of the patients were enrolled with intolerance to previous therapy and the other one-half as a result of disease that was refractory to prior therapy. Three patients were noted to have disseminated disease, one of which had a successful outcome after failing amphotericin B therapy.
Fusarium spp.: 11 of 24 patients were successfully treated with NOXAFIL oral suspension. 4 of the responders had disseminated disease and one patient had disease localized to the eye; the remainder had a variety of sites of infection. 7 of 24 patients had profound neutropenia at baseline. In addition, 3/5 patients with infection due to F. solani which is typically resistant to most antifungal agents, were successfully treated.
Cryptococcus: 15 of 31 patients were successfully treated with NOXAFIL oral suspension. Most of the patients were HIV infected with refractory cryptococcal meningitis.
Chromoblastomycosis/Mycetoma: 9 of 11 patients were successfully treated with NOXAFIL oral suspension. 5 of these patients had chromoblastomycosis due to Fonsecaea pedrosoi and 4 had mycetoma, mostly due to Madurella species.
Coccidioidomycosis: The efficacy of NOXAFIL in the primary treatment of non-meningeal coccidioidomycosis was demonstrated in 15 clinically evaluable patients enrolled in an open-label, non-comparative trial to receive NOXAFIL 400 mg daily for 6 months. Most patients were otherwise healthy and had infections at a variety of sites. A satisfactory response (defined as an improvement of at least 50% of the Cocci score as defined by the BAMSG Coccidioidomycosis trial group) was seen in 12 of 15 patients (80%) after an average of 4 months of NOXAFIL treatment. In a separate open-label, non-comparative trial, the safety and efficacy of NOXAFIL 400 mg twice a day was assessed in 16 patients with coccidioidomycosis infection refractory to standard treatment. Most had been treated with amphotericin B (including lipid formulations) and/or itraconazole or fluconazole for months to years prior to NOXAFIL treatment. At the end of treatment with NOXAFIL, a satisfactory response (complete or partial resolution of signs and symptoms present at baseline) as determined by an independent panel was achieved for 11/16 (69%) of patients. One patient with CNS disease that had failed fluconazole therapy had a successful outcome following 12 months of NOXAFIL therapy.
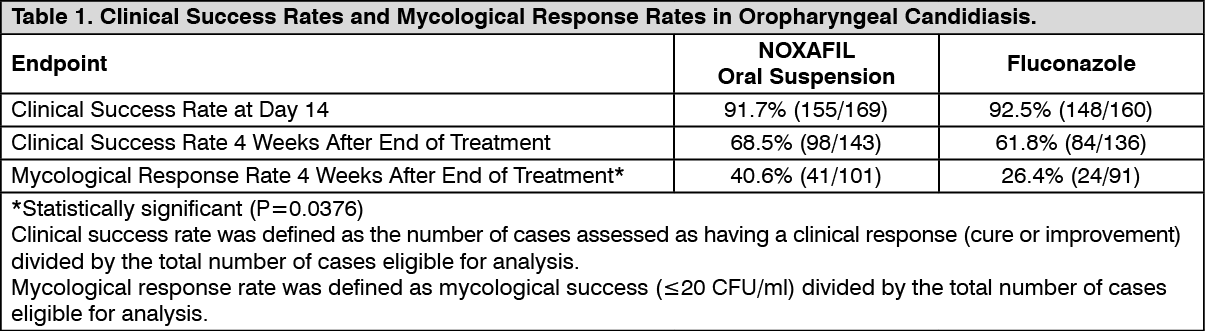
Treatment of Azole-susceptible Oropharyngeal Candidiasis (OPC): A randomised, double-blind, controlled study was completed in HIV-infected patients with azole-susceptible oropharyngeal candidiasis. The primary efficacy variable was the clinical success rate (defined as cure or improvement) after 14 days of treatment. Patients were treated with NOXAFIL or fluconazole oral suspension (both NOXAFIL and fluconazole were given as follows: 100 mg twice a day for 1 day followed by 100 mg once a day for 13 days).
The clinical and mycological response rates from the previous study are shown in the Table 1 as follows.
NOXAFIL and fluconazole demonstrated equivalent clinical success rates at Day 14 as well as 4 weeks after the end of treatment. However, NOXAFIL oral suspension demonstrated a significantly better sustained mycological response rate than fluconazole. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment of Azole-refractory Oropharyngeal Candidiasis (rOPC) (Studies 330 and 298): The primary efficacy parameter in Study 330 was the clinical success rate (cure or improvement) after 4 weeks of treatment. HIV-infected patients were treated with NOXAFIL oral suspension 400 mg twice a day with an option for further treatment during a 3-month maintenance period. A 75% (132/176) clinical success rate and a 36.5% (46/126) mycological response rate (≤20 CFU/ml) were achieved after 4 weeks of NOXAFIL treatment. Clinical success rates ranged from 71% to 100%, inclusive, for all azole-resistant Candida species identified at baseline, including C. glabrata and C. krusei.
Of the total patients treated in this study, 43 had azole-refractory esophageal candidiasis, either alone or in combination with OPC. All patients with azole-refractory EC had endoscopically confirmed EC at baseline. The clinical success rate after 4 weeks was 74.4%.
In Study 298 the primary efficacy endpoint was the clinical success rate (cure or improvement) after 3 months of treatment. A total of 100 HIV-infected patients with OPC and/or EC were treated with NOXAFIL 400 mg twice a day for up to 15 months. Sixty of these patients had been previously treated in Study 330. An 85.6% (77/90) clinical success rate overall (cure or improvement) was achieved after 3 months of NOXAFIL treatment; 80.6% (25/31) for previously untreated subjects.
The mean exposure to NOXAFIL based on the actual days dosed was 102 days (range: 1-544 days). Sixty-seven percent (67%, 10/15) of patients treated with NOXAFIL for at least 12 months had continued clinical success at the last assessment.
Of the patients treated in Study 298, 15 with azole-refractory EC had been previously treated in Study 330. Sixty-seven percent (67%, 10/15) were considered cured by the end of treatment and 33% (5/15) were considered improved. For those patients, treatment durations ranged from 81 to 651 days.
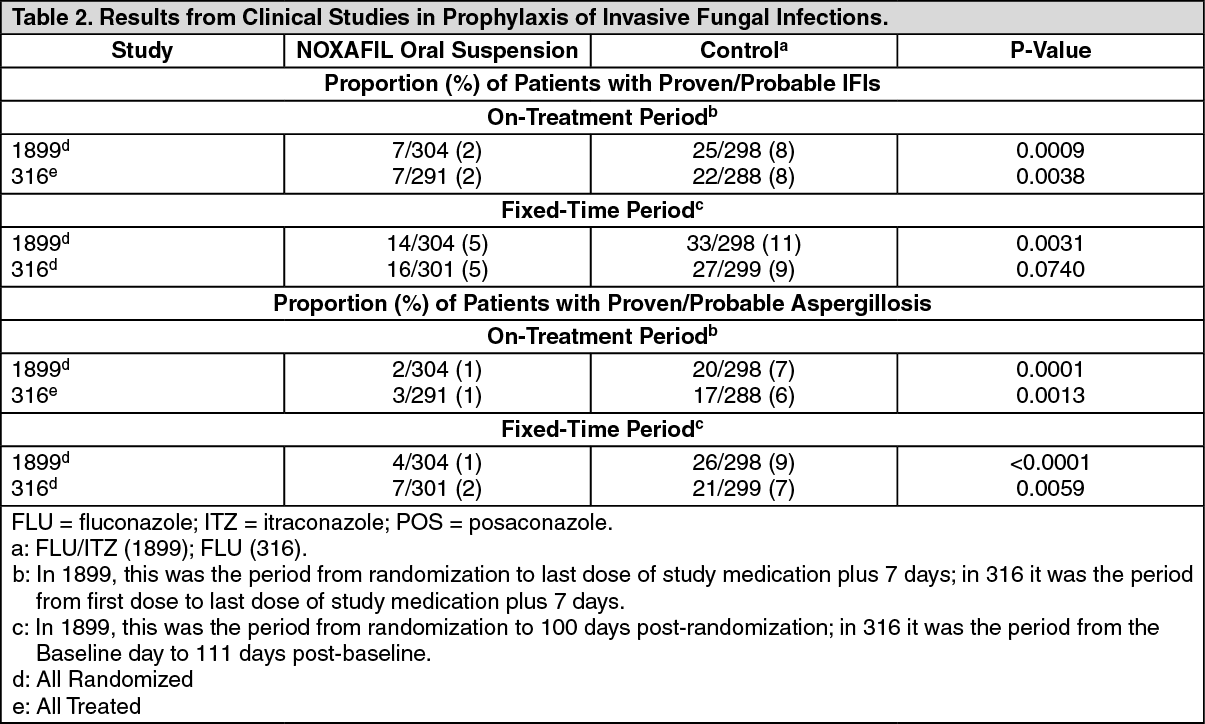
Prophylaxis of Invasive Fungal Infections (IFIs) (Studies 316 and 1899): Two large, randomised, controlled studies were conducted using NOXAFIL oral suspension as prophylaxis for the prevention of IFIs among patients at high risk.
Study 316 was a randomised, double-blind trial that compared NOXAFIL oral suspension (200 mg three times a day) with fluconazole capsules (400 mg once daily) as prophylaxis against invasive fungal infections in allogeneic HSCT recipients with graft versus host disease (GVHD). The primary efficacy endpoint was the incidence of proven/probable IFIs at 16 weeks post-randomization as determined by an independent, blinded external expert panel. A key secondary endpoint was the incidence of proven/probable IFIs during the on-treatment period (first dose to last dose of study medication + 7 days). The mean duration of therapy was comparable between the two treatment groups (80 days, NOXAFIL; 77 days, fluconazole).
Study 1899 was a randomised, evaluator-blinded study that compared NOXAFIL oral suspension (200 mg three times a day) with fluconazole suspension (400 mg once daily) or itraconazole oral solution (200 mg twice a day) as prophylaxis against IFIs in neutropenic patients who were receiving cytotoxic chemotherapy for acute myelogenous leukemia or myelodysplastic syndromes. The primary efficacy endpoint was the incidence of proven/probable IFIs as determined by an independent, blinded external expert panel during the on-treatment period. A key secondary endpoint was the incidence of proven/probable IFIs at 100 days post-randomization. The mean duration of therapy was comparable between the two treatment groups (29 days, NOXAFIL; 25 days, fluconazole/itraconazole).
In both prophylaxis studies, aspergillosis was the most common breakthrough infection. There were significantly fewer breakthrough Aspergillus infections in patients receiving NOXAFIL prophylaxis when compared to control patients receiving fluconazole or itraconazole. See Table 2 for results from both studies. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn Study 1899, a significant decrease in all cause mortality in favour of NOXAFIL was observed [POS 49/304 (16%) vs. FLU/ITZ 67/298 (22%) p= 0.048]. Based on Kaplan-Meier estimates, the probability of survival up to day 100 after randomization, was significantly higher for NOXAFIL recipients; this survival benefit was demonstrated when the analysis considered all causes of death (P=0.0354) (figure) as well as IFI-related deaths (P=0.0209). (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn Study 316, overall mortality was similar (POS, 25%; FLU, 28%); however, the proportion of IFI-related deaths was significantly lower in the POS group (4/301) compared with the FLU group (12/299; P= 0.0413).
Pharmacokinetics: Absorption: NOXAFIL delayed release tablets are absorbed with a median Tmax of 4 to 5 hours and exhibit dose proportional pharmacokinetics after single and multiple dosing up to 300 mg. Following a single dose administration of 300 mg posaconazole tablets after a high fat meal to healthy volunteers, the AUC0-72 hours and Cmax were higher compared to administration under fasted condition (51% and 16% for AUC0-72 hours and Cmax respectively).
Posaconazole plasma concentrations following administration of posaconazole tablets may increase over time in some patients. The reason for this time-dependency is not completely understood.
The absolute availability of the oral tablet is approximately 54%.
NOXAFIL delayed release tablets can be given once daily after a BID dosing on Day 1.
NOXAFIL oral suspension is absorbed with a median Tmax of 3 hours (patients) and 5 hours (healthy volunteers). The pharmacokinetics of NOXAFIL oral suspension are linear following single and multiple dose administration of up to 800 mg. No further increases in exposure were observed when oral suspension doses above 800 mg daily were administered to patients and healthy volunteers. Dividing the total NOXAFIL oral suspension daily dose (800 mg) as 400 mg twice a day results in a 184% higher exposure relative to once-a-day administration in patients. Exposure further increased when NOXAFIL was given as 200 mg four times daily.
Effect of food on oral absorption in healthy volunteers: NOXAFIL delayed release tablets can be taken without regard to food.
The AUC of NOXAFIL oral suspension is about 2.6 times greater when administered with a nonfat meal or nutritional supplement (14 gm fat) and 4 times greater when administered with a high-fat meal (~ 50 gm fat) relative to the fasted state. NOXAFIL oral suspension should be administered with food or a nutritional supplement.
Distribution: NOXAFIL delayed release tablets have a mean apparent volume of distribution of 394 L (42%), ranging between 294-583 L among the studies in healthy volunteers.
NOXAFIL oral suspension has a large apparent volume of distribution (1,774 L) suggesting extensive penetration into the peripheral tissues.
NOXAFIL is highly protein bound (>98.0%), predominantly to serum albumin.
Metabolism: NOXAFIL does not have any major circulating metabolites and its concentrations are unlikely to be altered by inhibitors of CYP450 enzymes. Of the circulating metabolites, the majority are glucuronide conjugates of NOXAFIL with only minor amounts of oxidative (CYP450 mediated) metabolites observed. The excreted metabolites in urine and feces account for approximately 17% of the administered radiolabeled dose.
Excretion: NOXAFIL is predominantly excreted in the feces (77% of the radiolabeled dose) with the major component eliminated as parent drug (66% of the radiolabeled dose). Renal clearance is a minor elimination pathway, with 14% of the radiolabeled dose excreted in urine (<0.2% of the radiolabeled dose is parent drug).
NOXAFIL delayed release tablet is eliminated with a mean half-life (t½) ranging between 26 and 31 hours and a mean apparent clearance ranging from 7.5 to 11 L/hr.
NOXAFIL oral suspension is slowly eliminated with a mean half-life (t½) of 35 hours (range 20 to 66 hours) and apparent total body clearance (Cl/F) of 32 L/hr. Steady-state is attained following 7 to 10 days of multiple dose administration.
Summary of the mean pharmacokinetic parameters in patients: The general pharmacokinetic findings across the clinical program in both healthy volunteers and patients were consistent, in that NOXAFIL was slowly absorbed and slowly eliminated with an extensive volume of distribution.
Exposure following multiple administration of NOXAFIL delayed release tablets (200 or 300 mg) QD was 1.3 times higher in healthy volunteers than in patients.
The exposure to NOXAFIL following administration of 400 mg oral suspension twice a day was ~ 3 times higher in healthy volunteers than in patients, without additional safety findings at the higher concentrations.
Pharmacokinetics in Special Populations: Children (<18 years): Use of NOXAFIL delayed release tablet in patients 13 to 17 years of age is supported by evidence from adequate and well-controlled studies of NOXAFIL oral suspension.
Following administration of 800 mg per day of NOXAFIL oral suspension as a divided dose for treatment of invasive fungal infections, mean trough plasma concentrations from 12 patients 8-17 years of age (776 ng/ml) were similar to concentrations from 194 patients 18-64 years of age (817 ng/ml). Similarly, in the prophylaxis studies, the mean steady-state NOXAFIL average concentration (Cav) was comparable among ten children (13-17 years of age) to Cav achieved in adults (≥18 years of age).
In a study of 136 neutropenic pediatric patients 11 months - 17 years treated with posaconazole oral suspension, approximately 50% met the prespecified target (Day 7 Cav between 500 ng/mL-2500 ng/mL).
In general, exposures tended to be higher in the older patients (7 to <18 years) than in younger patients (2 to <7 years).
Gender: The pharmacokinetics of NOXAFIL are comparable in men and women. No adjustment in the dosage of NOXAFIL is necessary based on gender.
Geriatric: Of the 230 patients treated with NOXAFIL delayed release tablets, 38 (17%) were greater than 65 years of age. The pharmacokinetics of NOXAFIL delayed release tablets are comparable in young and elderly subjects. No overall differences in safety were observed between the geriatric patients and younger patients; therefore, no dosage adjustment is recommended for geriatric patients.
An increase in Cmax (26%) and AUC (29%) was observed in elderly subjects (24 subjects ≥65 years of age) receiving NOXAFIL oral suspension relative to younger subjects (24 subjects 18 - 45 years of age). However, in a population pharmacokinetic analysis (Study 1899) age did not influence the pharmacokinetics of posaconazole oral suspension. Further, in clinical efficacy trials, the safety profile of NOXAFIL oral suspension between the young and elderly patients was similar. Therefore, no dose adjustment is required for age.
Race: There is insufficient data among different races with NOXAFIL delayed release tablets.
Results from a multiple dose study in healthy volunteers (n=56) indicated that there was only a slight decrease (16%) in the AUC and Cmax of NOXAFIL oral suspension in Black subjects relative to Caucasian subjects, therefore, no dose adjustment for race is required.
Weight: Pharmacokinetic modeling for NOXAFIL suggests that patients weighing greater than 120 kg may have lower NOXAFIL exposure. It is, therefore, suggested to closely monitor for breakthrough fungal infections in patients weighing more than 120 kg.
Patients, in particular those receiving posaconazole after HSCT, who have a low body weight (<60 kg) are more likely to experience higher plasma concentrations of posaconazole and should be closely monitored for adverse events.
Renal insufficiency: Following single dose administration, there was no effect of mild and moderate renal insufficiency (n=18, Clcr ≥20 ml/min/1.73 m2) on NOXAFIL pharmacokinetics, therefore, no dose adjustment is required. In subjects with severe renal insufficiency (n=6, Clcr <20 ml/min/1.73 m2), the exposure of NOXAFIL was highly variable (96% CV) compared to the exposure in the other renal groups (<40% CV). However, as NOXAFIL is not significantly renally eliminated, an effect of severe renal insufficiency on the pharmacokinetics of NOXAFIL is not expected and no dose adjustment is recommended. NOXAFIL is not removed by hemodialysis. Due to the variability in exposure, patients with severe renal impairment should be monitored closely for breakthrough fungal infections.
Similar recommendations apply to NOXAFIL delayed release tablets; however, a specific study has not been conducted with NOXAFIL delayed release tablets.
Hepatic insufficiency: In a small number of subjects (n=12) studied with hepatic insufficiency (Child-Pugh class A, B or C), Cmax values generally decreased with the severity of hepatic dysfunction (545, 414 and 347 ng/ml for the mild, moderate, and severe groups, respectively), even though the Cmax values (mean 508 ng/ml) for the normal subjects were consistent with previous trials in healthy volunteers. In addition, an increase in half-life was also associated with a decrease in hepatic function (26.6, 35.3, and 46.1 hours for the mild, moderate, and severe groups, respectively), as all groups had longer half-life values than subjects with normal hepatic function (22.1 hours). Due to the limited pharmacokinetic data in patients with hepatic insufficiency; no recommendation for dose adjustment can be made.
Similar recommendations apply to NOXAFIL delayed release tablets; however, a specific study has not been conducted with NOXAFIL delayed release tablets.
Toxicology: Preclinical Information: As observed with other azole antifungal agents, effects related to inhibition of steroid hormone synthesis were seen in repeated-dose toxicity studies with NOXAFIL. Adrenal suppressive effects were observed in toxicity studies in rats and dogs at exposures equal to or greater than those obtained at therapeutic doses in humans.
Reproduction, peri- and postnatal development studies were conducted in rats. At exposures lower than those obtained at therapeutic doses in humans, NOXAFIL caused skeletal variations and malformations, dystocia, increased length of gestation, reduced mean litter size and postnatal viability. In rabbits, NOXAFIL was embryotoxic at exposures greater than those obtained at therapeutic doses. As observed with other azole antifungal agents, these effects on reproduction were considered related to a treatment-related effect on steroidogenesis.
NOXAFIL was not genotoxic in in vitro and in vivo studies. Carcinogenicity studies did not reveal special hazards for humans.
Microbiology: NOXAFIL has been shown in vitro to be active against the following micro-organisms: Aspergillus species (A. fumigatus, A. flavus, A. terreus, A. nidulans, A. niger, A. ustus, A. ochraceus), Candida species (C. albicans, C. glabrata, C. krusei, C. parapsilosis), Cryptococcus neoformans, Coccidioides immitis, Fonsecaea pedrosoi, Histoplasma capsulatum, Pseudallescheria boydii and species of Alternaria, Exophiala, Fusarium, Ramichloridium, Rhizomucor, Mucor, and Rhizopus. NOXAFIL also exhibits in vitro activity against the following yeasts and moulds: Candida dubliniensis, C. famata, C. guilliermondii, C. lusitaniae, C. kefyr, C. rugosa, C. tropicalis, C. zeylanoides, C. inconspicua, C. lipolytica, C. norvegensis, C. pseudotropicalis, Cryptococcus laurentii, Kluyveromyces marxianus, Saccharomyces cerevisiae, Yarrowia lipolytica, species of Pichia, and Trichosporon, Aspergillus sydowii, Bjerkandera adusta, Blastomyces dermatitidis, Epidermophyton floccosum, Paracoccidioides brasiliensis, Scedosporium apiospermum, Sporothrix schenckii, Wangiella dermatitidis and species of Absidia, Apophysomyces, Bipolaris, Curvularia, Microsporum, Paecilomyces, Penicillium, and Trichophyton. However, the safety and effectiveness of NOXAFIL in treating clinical infections due to these microorganisms have not been established in clinical trials.
In vitro NOXAFIL exhibits broad-spectrum antifungal activity against some yeasts and moulds not generally responsive to azoles, or resistant to other azoles: species of Candida (including C. albicans isolates resistant to fluconazole, voriconazole and itraconazole, C. krusei and C. glabrata which are inherently less susceptible to fluconazole, C. lusitaniae which is inherently less susceptible to amphotericin B), Aspergillus (including isolates resistant to fluconazole, voriconazole, itraconazole and amphotericin B), organisms not previously regarded as being susceptible to azoles such as the zygomycetes (e.g., species of Absidia, Mucor, Rhizopus and Rhizomucor).
In vitro NOXAFIL exhibited fungicidal activity against species of: Aspergillus, dimorphic fungi (Blastomyces dermatitidis, Histoplasma capsulatum, Penicillium marneffei, Coccidioides immitis), some species of Candida.
In animal infection models NOXAFIL was active against a wide variety of fungal infections caused by moulds or yeasts. However, there was no consistent correlation between minimum inhibitory concentration and efficacy.
Specimens for fungal culture and other relevant laboratory studies (including histopathology) should be obtained prior to therapy to isolate and identify causative organism(s). Therapy may be instituted before the results of the cultures and other laboratory studies are known. However, once these results become available, antifungal therapy should be adjusted accordingly.
Drug Resistance: C. albicans strains resistant to NOXAFIL could not be generated in the laboratory; spontaneous laboratory Aspergillus fumigatus mutants exhibiting a decrease in susceptibility to NOXAFIL arose at a frequency of 1x10-8 to 1x10-9. Clinical isolates of Candida albicans and Aspergillus fumigatus exhibiting significant decreases in NOXAFIL susceptibility are rare. In those rare instances where decreased susceptibility was noted, there was no clear correlation between decreased susceptibility and clinical failure. Clinical success has been observed in patients infected with organisms resistant to other azoles; consistent with these observations NOXAFIL was active in vitro against many Aspergillus and Candida strains that developed resistance to other azoles and/or amphotericin B. Breakpoints for NOXAFIL have not been established for any fungi.
Antifungal medicinal product combinations: When combinations of NOXAFIL with either amphotericin B or caspofungin were tested in vitro and in vivo there was little or no antagonism and in some instances there was an additive effect. The clinical significance of these results is unknown.