Pharmacotherapeutic group: meningococcal vaccines.
ATC code: J07AH08.
Pharmacology: Pharmacodynamics: Mechanism of action: Anti-capsular meningococcal antibodies protect against meningococcal diseases via complement mediated bactericidal activity.
MenQuadfi induces the production of bactericidal antibodies specific to the capsular polysaccharides of
Neisseria meningitidis serogroups A, C, W, and Y.
Immunogenicity: The immunogenicity of a single dose of MenQuadfi for primary vaccination in toddlers (12-23 months of age), children and adolescents (2-17 years of age), adults (18-55 years of age) and older adults (56 years and above) was assessed in six pivotal studies and in one post licensure supportive study in toddlers (12-23 months of age). The immunogenicity of a single dose of MenQuadfi for booster vaccination (subjects 15 to 55 years of age) was assessed in one pivotal study. In addition, antibody persistence after primary vaccination and immunogenicity of a booster dose was assessed in one post licensure supportive study in children (4-5 years of age).
Primary immunogenicity analyses were conducted by measuring serum bactericidal activity (SBA) using human serum as the source of exogenous complement (hSBA). Rabbit complement (rSBA) data are available in subsets in all age groups and generally follows the trends observed with human complement (hSBA) data. In addition, all subjects were assessed for primary immunogenicity measured by hSBA and rSBA for serogroup C in MEQ00065 study [NCT03890367].
Clinical data on the persistence of antibody response 3 years after primary vaccination with MenQuadfi at 12-23 months of age are available in children 4-5 years of age. Clinical data on booster vaccination with MenQuadfi in those children are also available.
Toddlers 12 to 23 month of age: Immunogenicity in subjects 12 through 23 months of age was evaluated in three clinical studies (MET51 [NCT02955797], MET57 [NCT03205371] and MEQ00065 [NCT03890367]).
MET51 was conducted in subjects who were either meningococcal vaccine naïve or had been primed with monovalent meningococcal C conjugate vaccines in their first year of life (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Response in subjects previously vaccinated with MenC conjugate vaccines in their first year of life: The majority of monovalent meningococcal C conjugate vaccine primed toddlers (12-23 months of age) in study MET51 (NCT02955797) had hSBA titres ≥1:8 in the MenQuadfi group (N=198) (≥86.7%) and in MenACWY-TT group (N=99) (≥85.7%) at D30 post-vaccination. These toddlers received during their infancy MenC-TT or MenC-CRM vaccines. Post-vaccination seroprotection rates were comparable between MenQuadfi and MenACWY-TT for all serogroups regardless of the priming background.
In MenC-CRM primed subjects the GMTs for serogroup A were lower in the MenQuadfi group (n=49) than in the MenACWY-TT group (n=25) [12.0 (8.23; 17.5) vs 42.2 (25.9; 68.8)]. After administration of Menquadfi seroprotection rates (hSBA titres ≥1:8) for subjects primed with MenC-CRM were lower but still comparable for serogroups A, Y and W compared with those in the MenACWY-TT group [A: 68.8% (53.7; 81.3) vs 96.0% (79.6; 99.9)]; Y: 95.8% (85.7; 99.5) vs 80.0% (59.3; 93.2); W: 68.1% (52.9; 80.9) vs 79.2% (57.8; 92.9)]. The rates for serogroup C were comparable in both groups [95.7% (85.5; 99.5) vs 92.0% (74.0; 99.0)]. The clinical relevance of these results is unknown. This aspect might be considered for individuals at high risk for MenA infection who received MenC-CRM vaccine in their first year of life.
MET57 (NCT03205371) was conducted in meningococcal vaccine naïve toddlers 12 through 23 months of age to assess the immunogenicity of the concomitant administration of MenQuadfi with paediatric vaccines (MMR+V, DTaP-IPV-HB-Hib or PCV-13). Overall, the post-vaccination hSBA seroprotection rates in subjects who received MenQuadfi was high for all serogroups (between 88.9% and 100%). Seroresponse and seroprotection rates for serogroup A were comparable when MenQuadfi was co-administered with PCV-13 and alone (56.1%, [95% CI 48.9; 63.2] and 83.7% [95% CI 77.7; 88.6] vs 71.9% [95%CI 61.8; 80.6] and 90.6% [95% CI 82.9; 95.6]). There were differences in the hSBA GMTs for serogroup A when MenQuadfi was co-administered with PCV-13 (n=196) compared with MenQuadfi administered alone (n=96) (24.6 [95% CI 20.2; 30.1] and 49.0 [95% CI 36.8; 65.3]).) The clinical relevance of these results is unknown but this observation might be taken into consideration for individuals at high risk for MenA infection and consequently vaccinations with MenQuadfi and PCV13 might be performed separately.
MEQ00065 (NCT03890367) study was conducted in meningococcal vaccine naïve toddlers 12 through 23 months of age to assess the immunogenicity of serogroup C using hSBA and rSBA assays following administration of a single dose of MenQuadfi compared to MenACWY-TT or to MenC-TT.
Superiority of MenQuadfi was demonstrated in comparison to MenACWY-TT vaccine for the hSBA seroprotection rate and hSBA and rSBA GMTs to meningococcal serogroup C. Non-inferiority was demonstrated for the rSBA seroprotection rate to meningococcal serogroup C.
Superiority of MenQuadfi was also demonstrated in comparison to MenC-TT vaccine for the rSBA and hSBA GMTs to meningococcal serogroup C and non-inferiority was demonstrated for the rSBA and hSBA seroprotection rates to meningococcal serogroup C (see table 2).
Click on icon to see table/diagram/image
Immunogenicity booster and persistence response: MET62 (NCT03476135) evaluated the antibody persistence of a primary dose, immunogenicity and the safety of a booster dose of MenQuadfi in children 4-5 years of age. These children were primed with a single dose of MenQuadfi or MenACWY-TT 3 years before as part of the phase II study MET54 when they were 12-23 months old. The antibody persistence prior to the MenQuadfi booster dose and the booster immune response were assessed according to the vaccine (MenQuadfi or MenACWY-TT) children had received 3 years ago (see table 3).
For all serogroups, hSBA GMTs were higher at D30 post-primary dose than at D0 pre-booster dose for MenQuadfi or MenACWY-TT. The pre-booster GMTs were higher than the pre-primary dose, indicative of long-term persistence of immune response.
After the booster dose, seroprotection rates were nearly 100% for all serogroups in children primed with MenQuadfi. (See Table 3.)
Click on icon to see table/diagram/image
Children 2 through 9 years of age: Immunogenicity in subjects 2 through 9 years of age was evaluated in study MET35 (NCT03077438) (stratified by ages 2 through 5 and 6 through 9 years) comparing seroresponses following administration of either MenQuadfi or MenACWY-CRM.
Overall, for subjects 2 through 9 years of age, immune non-inferiority, based on hSBA seroresponse, was demonstrated for MenQuadfi as compared to MenACWY-CRM for all four serogroups. (See Table 4.)
Click on icon to see table/diagram/image
Children and adolescents 10 through 17 years of age: Immunogenicity in subjects aged 10 through 17 years of age was evaluated in two studies comparing seroresponses following administration of MenQuadfi compared to either MenACWY-CRM (MET50[NCT02199691]) or MenACWY-DT (MET43[NCT02842853]).
MET50 was conducted in meningococcal vaccine naïve subjects and seroresponse was evaluated following administration with either MenQuadfi alone, MenACWY-CRM alone, MenQuadfi co- administered with Tdap and HPV or Tdap and HPV alone. (See Table 5.)
Click on icon to see table/diagram/image
Study MET43 was performed to evaluate the immunogenicity of MenQuadfi compared to
MenACWY-DT in children, adolescents and adults (10-55 years of age). (See Table 6.)
Click on icon to see table/diagram/image
Adults 18 through 55 years of age: Immunogenicity in subjects from 18 through 55 years of age was evaluated in study MET43 (NCT02842853) comparing MenQuadfi to MenACWY-DT. (See Table 7.)
Click on icon to see table/diagram/image
Adults 56 years of age and older: Immunogenicity in adults ≥ 56 years of age (mean 67.1 years, range 56.0 - 97.2 years) was assessed in study MET49 (NCT02842866) comparing the immunogenicity of MenQuadfi to MenACWY polysaccharide vaccine. (See Table 8.)
Click on icon to see table/diagram/image
Booster response: Study MET56 (NCT02752906) compared the immunogenicity of a booster dose of MenQuadfi with a booster dose of MenACWY-DT in subjects at least 15 years of age. These subjects were primed with a quadrivalent meningococcal conjugate vaccine (MenACWY-CRM (11.3%) or with MenACWY-DT (86.3%)) 4 to 10 years earlier.
At baseline, hSBA seroprotection and GMT were similar for serogroups A, C, W, and Y. (See Table 9.)
Click on icon to see table/diagram/image
Clinical data on the persistence of antibody response 3 years after primary vaccination with MenQuadfi at 12-23 months of age are available in children 4-5 years of age. Clinical data on booster vaccination with MenQuadfi in those children are also available.
Pharmacokinetics: No pharmacokinetic studies have been performed.
Toxicology: Preclinical safety data: Non-clinical safety data revealed no special risks for humans based on a developmental and reproductive toxicity study in female rabbits.
The administration of MenQuadfi to female rabbits at a full human dose showed no effects on mating performance, female fertility, no teratogenic potential, and no effect on pre- or post-natal development.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image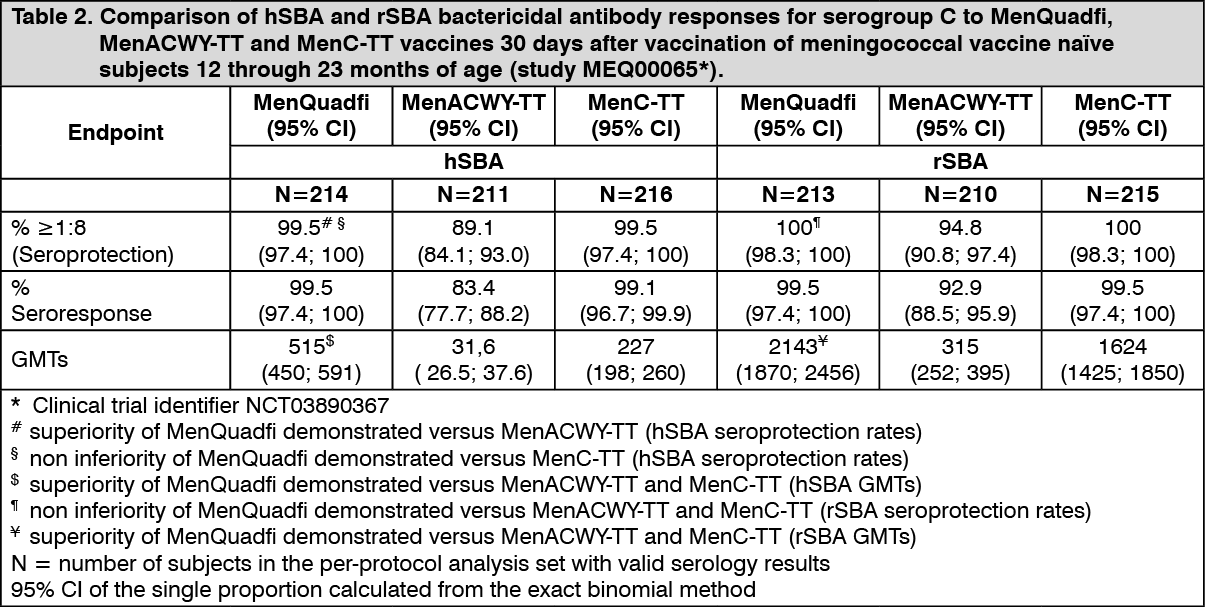 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
