Iron (III) hydroxide polymaltose complex.
FC tablet: Each film-coated tablet contains 100 mg iron as iron (III) hydroxide polymaltose complex.
Syrup: 1 ml of syrup contains 10 mg of iron as iron (III)-hydroxide polymaltose complex (IPC).
Oral drops: Qualitative and quantitative composition: 1 ml (20 drops) contains 50 mg of iron as iron (III)-hydroxide polymaltose complex (IPC).
Excipients/Inactive Ingredients: FC tablet: Crospovidone, hydroxypropylcellulose, hydroxypropyl methylcellulose, iron oxide red (E172), iron oxide yellow (E172), macrogol 6000, magnesium stearate, microcrystalline cellulose, titanium dioxide (E172).
Syrup: Purified water, sorbitol solution (70%), sucrose, ethanol, cream essence, methyl hydroxybenzoate (E218), propyl hydroxybenzoate (E216) and sodium hydroxide.
Oral drops: Purified water, sucrose, cream essence, sodium methyl hydroxybenzoate (E219), sodium propyl hydroxybenzoate (E217) and sodium hydroxide.
Pharmacotherapeutical group: iron preparation. ATC Code: B03AB05.
Oral drops: Maltofer drops are an iron preparation for the treatment of iron deficiency without anaemia and iron deficiency anaemia.
Iron is an important constituent of haemoglobin, myoglobin, and iron-containing enzymes. In general, iron deficiency can cause chronic fatigue, lack of concentration and reduced mental performance, irritability, anxiety, headache, loss of appetite, susceptibility to infection, conspicuous paleness, cracks at the corners of the mouth (rhagades), dry skin and brittle hair and nails.
In the iron (III)-hydroxide polymaltose complex, the polynuclear iron (III)-hydroxide core is superficially surrounded by a number of non-covalently bound polymaltose molecules resulting in an overall average molecular weight of approximately 50 kDa. The polynuclear core of IPC has a structure similar to that of the physiological iron storage protein, ferritin. IPC is a stable complex and does not release large amounts of iron under physiological conditions. Because of its size, the extent of diffusion of IPC through the membrane of the mucosa is about 40 times less than that of the hexaquo-iron (II) complex. Iron from IPC is taken up in the gut via an active mechanism. In contrast to iron (II) salts, IPC does not have pro-oxidative properties.
Mechanism of action: The polynuclear iron (III) hydroxide core in IPC is surrounded at its surface by a number of non-covalently bound polymaltose molecules, which leads to an average total molecular weight of around 50 kDa. The polynuclear iron core of IPC has a structure similar to that of the physiological iron storage protein ferritin. IPC is a stable complex and releases no large quantities of iron under physiological conditions. Due to its size, the magnitude of IPC diffusion taking place through the mucosa is around 40 times less than in most water-soluble iron (II) salts present in aqueous solution as a hexaaqua iron (II) complex. Iron is absorbed in the intestines from IPC through an active mechanism.
Pharmacodynamics: The iron absorbed is bound to transferrin and is used for Hb synthesis in the bone marrow or stored primarily in the liver bound to ferritin.
Clinical Efficacy: The efficacy of Maltofer compared to a placebo or similar preparations with different iron formulations in terms of normalising haemoglobin values and replenishing iron stores has been demonstrated in numerous clinical studies in infants, children, adolescents and adults. Both solid and liquid galenic forms of IPC were used in these studies. The primary goal of an oral iron replacement is to maintain the body's own iron stores within normal limit values (to prevent an iron deficiency, e.g. in case of increased requirements), replenish iron stores or correct existing iron deficiency anaemia.
Clinical studies in adults: A total of 11 controlled clinical studies have been carried out with IPC mono-preparations in comparison with a placebo and/or oral iron (II) preparations. A total of more than 900 patients were involved, and approximately 500 of these patients received IPC mono-preparations. The patient population studied demonstrated no relevant differences in haematological and iron parameters (haemoglobin (Hb), mean red blood cell haemoglobin (MCV), serum ferritin) at the start of treatment. The oral iron replacement with IPC at a dose of 100-200 mg iron/day for several weeks up to a maximum of 6 months demonstrated a clinically relevant increase in iron and haematological parameters at the end of treatment compared to those at the start of treatment. The improvement in haematological parameters (Hb, MCV, serum ferritin) after a 12 week treatment with IPC was comparable to treatment with iron (II) sulphate.
The efficacy of IPC compared to iron (II) sulphate was investigated on the basis of a meta-analysis of 6 prospective, randomised clinical studies in adult patients with iron deficiency anaemia. The total number of patients included in the study was 557; 319 patients received IPC and 238 patients iron (II) sulphate. The pooled mean haemoglobin values at the start of treatment were 10.35 ±0.92 g/dL (IPC) and 10.20 ±0.93 g/dL (iron (II) sulphate). After an average treatment period of 8 to 13 weeks with equivalent posology, mean haemoglobin values were determined 12.13 ±1.19 g/dL (IPC) and 11.94 ±1.84 g/dL (iron (II) sulphate), p=0.93 increases in haemoglobin were greater after a longer treatment duration for both iron formulations.
Clinical studies in children and adolescents: The use of Maltofer in children and adolescents (18 years old or younger) was investigated in a number of clinical studies involving over 1000 patients. The efficacy of Maltofer in terms of improving iron values compared to the placebo or comparable preparations with different iron formulations was thereby confirmed.
Pharmacokinetics: Absorption: Studies with radio-labelled IPC show a good correlation between iron absorption and build-up of iron in haemoglobin. The relative absorption of iron correlates with the degree of iron deficiency (i.e. the greater the iron deficiency, the higher the iron absorption). In contrast to iron (II) salts, it was determined that food had no negative effect on the bioavailability of iron from Maltofer: significantly increased bioavailability of iron with concomitant ingestion of food was demonstrated in a clinical study, while three other studies showed a positive trend but no clinically significant effects.
Elimination: Iron that is not absorbed is eliminated in the faeces.
Toxicology: Preclinical data: Non-clinical data obtained for IPC does not reveal any special hazards for humans based on conventional studies of individual dose toxicity and repeated dose toxicity, genotoxicity or reproduction and development toxicity.
Other information: The LD50 of IPC, which was determined in animal trials with mice and rats, was higher than an orally administered dose of 2,000 mg of iron per kg of body weight.
FC tablet: Treatment of iron deficiency. Prevention of iron deficiency during pregnancy.
Syrup: Treatment of iron deficiency without anaemia and iron deficiency anaemia. Prophylactic therapy of iron deficiency during pregnancy.
Oral drops: Treatment of iron deficiency without anaemia and iron deficiency anaemia.
Prophylactic therapy of iron deficiency to cover the recommended daily dietary allowances (RDA) during pregnancy and lactation, for children, adolescents and adults (e.g. vegetarians and elderly).
FC tablet: Treatment of Iron Deficiency with Reduced Number of Red Blood Cells in Adults and Children over 12 Years: 1 to 3 tablets once daily or divided into separate doses for about 3 to 5 months.
After normalisation of the red blood pigment (haemoglobin) value, continue with 1 tablet once daily for several weeks. This will replenish the iron stores.
Treatment of Iron Deficiency with Reduced Number of Red Blood Cells in Pregnancy: 2 to 3 tablets once daily or divided into separate doses.
After normalisation of the red blood pigment value, continue with 1 tablet once daily until, at least, the end of pregnancy. This will replenish the iron stores and provide the increased amount of iron required during pregnancy.
Treatment of Iron Deficiency with Normal Number of Red Blood Cells in Adults, Pregnancy, and Children over 12 years, and Prevention of Iron Deficiency in Pregnancy: 1 tablet once daily for 1 to 2 months
.
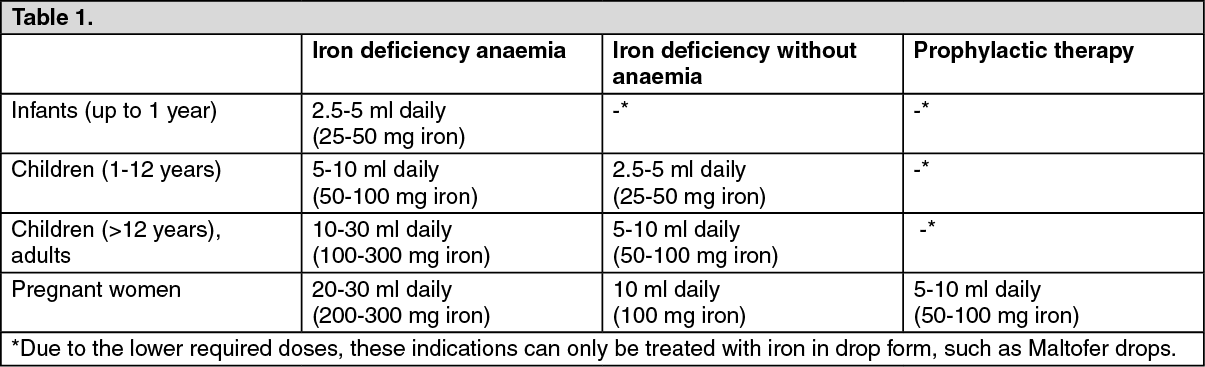
Syrup: Posology: Dosage and duration of therapy are dependent upon the extent of iron deficiency.
Iron deficiency anaemia: the therapy takes about 3-5 months until a normalisation of the haemoglobin value is achieved. Afterwards the therapy should be continued for several weeks, or for pregnant women, at least until the end of the pregnancy with a dosage such as described for iron deficiency without anaemia in order to replenish the iron stores.
Iron deficiency without anaemia: the therapy takes about 1-2 months. (See Table 1.)
 Click on icon to see table/diagram/image
Oral drops: Posology:
Click on icon to see table/diagram/image
Oral drops: Posology: Dosage and duration of therapy are dependent upon the extent of iron deficiency.
Iron deficiency anaemia: the therapy takes about 3-5 months until a normalisation of the haemoglobin value is achieved. Afterwards the therapy should be continued for several weeks, or for pregnant women, at least until the end of the pregnancy with a dosage such as described for iron deficiency without anaemia in order to replenish the iron stores.
Iron deficiency without anaemia: the therapy takes about 1-2 months. (See Tables 2 and 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Method of administration: The daily dosage can be divided into separate doses or can be taken all at one time. Maltofer should be taken during or immediately after a meal. Maltofer syrup/oral drops can be mixed with fruit and vegetable juices or with bottle-feed. The slight discolouration of the mixture does not affect either the efficacy of the product nor the taste of the drink to which it is added.
Syrup: The supplied measuring cup is used for an exact administration of the dosage.
Oral drops: Maltofer drops, the bottle needs to be held upside down and vertical. The drops should flow immediately. If this does not happen, tap the bottle gently until a drop forms. Do not shake the bottle.
Syrup & Oral drops: There are no reported cases of overdose leading to acute iron toxicity nor iron overload.
Syrup: In cases of overdosage neither intoxication nor iron overload have been reported to date.
FC tablet: All cases of iron overload and disturbances in utilization of iron.
Allergy to iron (III)-hydroxide polymaltose complex or any of the other ingredients of Maltofer.
An iron overload in the body.
Disturbed use of iron by the body.
Reduced number of red blood cells (anaemia), not caused by iron deficiency, such as due to increased red blood cell breakdown, vitamin B12 deficiency.
Syrup & Oral drops: Known hypersensitivity or intolerance to iron (III)-hydroxide polymaltose complex or any of the excipients.
Iron overload (e.g. haemochromatosis, haemosiderosis).
Disturbances in iron utilisation (e.g. anaemia from lead-poisoning, sidero-achrestic anaemia, thalassaemia).
Anaemia not caused by iron deficiency (e.g. haemolytic anaemia or megaloblastic anaemia due to vitamin B12 deficiency).
Syrup & Oral drops: Infections or tumours may cause anaemia. Since iron can be utilised only after correcting the primary disease, a benefit/risk evaluation is advisable.
During treatment with Maltofer, there may be dark discolouration of the faeces (stools).
Syrup: 1 mL of Maltofer syrup contains 1.2 mg of sodium. This corresponds to 0.06% of the WHO-recommended maximum daily intake of 2 g of sodium for adults.
Maltofer syrup contains small quantities of ethanol (alcohol) of less than 100 mg per 30 mL (maximum daily dose).
Maltofer syrup contains methyl hydroxybenzoate (E218) and propyl hydroxybenzoate (E216). These can cause allergic reactions, even delayed reactions.
Information for diabetics: Maltofer syrup contains 280 mg sorbitol and 200 mg sucrose corresponding to 0.04 bread units per 1 ml syrup.
Sorbitol can cause gastrointestinal disorders and has a slight laxative effect. Patients with hereditary fructose intolerance (HFI) should not take/receive this medicinal product. Sucrose can be harmful to the teeth.
Oral drops: 1 mL of Maltofer droplets contains 6 mg of sodium. This corresponds to 0.3% of the WHO-recommended maximum daily intake of 2 g of sodium for adults.
Maltofer droplets contain sodium methyl hydroxybenzoate (E219) and sodium propyl hydroxybenzoate (E217). These can cause allergic reactions, even delayed reactions.
Information for diabetics: Maltofer drops contain 50 mg of sucrose per 1 ml of drops (=20 drops), equivalent to 0.01 bread units per ml (20 drops).
Patients with a rare hereditary fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase deficiency should not use this medicinal product. Sucrose can be harmful to the teeth.
FC tablet: Driving and Using Machines: Maltofer has no or negligible influence on the ability to drive and use machines.
Use in Children 12 Years and Younger: Maltofer tablets are not recommended for this age group. Other iron medicines are more suitable, such as Maltofer oral drops and Maltofer syrup.
Use in Pregnancy & Use in Lactation: FC tablet: Based on the available data, negative influence on the foetus or the woman during pregnancy or breast-feeding is unlikely. However, as a precaution: If the patient is pregnant or breast-feeding, thinking may be pregnant or are planning to have a baby ask doctor or pharmacist for advice before taking this medicine.
Pregnancy: Syrup & Oral drops: Clinical data of exposed pregnancies exhibited no undesirable effects on pregnancy or on the health of the foetus or newborn infant (see Pharmacology under Actions). Data from epidemiological studies is not available. Animal studies did not show any reproductive toxicity (see Pharmacology: Toxicology: Preclinical data under Actions). Caution is advised for use during pregnancy. As a precautionary measure, Maltofer should only be taken after consulting a doctor.
Breast-feeding: Syrup & Oral drops: It is not known whether iron from the iron (III)-hydroxide polymaltose complex is excreted in human milk. Human milk naturally contains iron bound to lactoferrin. As a precautionary measure, Maltofer should only be taken during breast-feeding after consulting a doctor.
Syrup & Oral drops: The safety and tolerability of Maltofer has been evaluated in a Meta-analyisis of 24 publications or clinical study reports encompassing a total number of 1473 exposed patients.
Discoloured faeces are a well-known adverse drug reaction of oral iron medications but this is considered of no clinical relevance and is underreported. Other commonly seen side effects were gastrointestional disorders (Nausea, Constipation, Diarrhoea and abdominal pain). (See Table 4.)
Click on icon to see table/diagram/image
FC tablet: Side effects can occur with the following frequency:
Very common (may affect more than 1 in 10 people): Discoloured stool (dark discolouration of the faeces may occur during treatment with
Maltofer, however, this is harmless).
Common (may affect up to 1 in 10 people): Diarrhoea, nausea, indigestion.
Uncommon (may affect up to 1 in 100 people): Vomiting, constipation, abdominal pain, tooth discolouration, skin rash, itching, headache.
FC tablet: Concomitant use with injectable iron medicines is not recommended.
Syrup & Oral drops: Interactions of IPC with tetracycline or aluminium hydroxide were investigated in 3 human studies (crossover design, 22 patients per study). No significant reduction in the absorption of tetracycline was observed. The plasma tetracycline concentration did not fall below the minimum inhibitory concentration level necessary for bacteriostatic serum levels. Iron absorption from IPC was not reduced by aluminium hydroxide or tetracycline.
Iron (III) hydroxide polymaltose complex can therefore be administered at the same time as tetracycline or other phenolic compounds, as well as aluminium hydroxide.
Studies in rats with tetracycline, aluminium hydroxide, acetylsalicylate, sulphasalazine, calcium carbonate, calcium acetate and calcium phosphate in combination with vitamin D3, bromazepam, magnesium aspartate, D-penicillamine, methyldopa, paracetamol and auranofin have not shown any interactions with IPC.
Similarly, no interactions with food constituents such as phytic acid, oxalic acid, tannin, sodium alginate, choline and choline salts, vitamin A, vitamin D3 and vitamin E, soya oil and soya flour were observed in in vitro studies with IPC.
These results suggest that IPC can be taken during or immediately after food intake.
The haemoccult test (selective for Hb) for the detection of occult blood is not impaired and therefore there is no need to interrupt iron therapy.
Concomitant administration of parenteral and oral iron is not recommended since the absorption of oral iron would be inhibited.
FC tablet: Do not store above 30°C. Protect from light.
Syrup & Oral drops: Do not store above 30°C.
Keep the glass bottle in the original package (i.e. outer carton) in order to protect from light.
B03AB05 - ferric oxide polymaltose complexes ; Belongs to the class of oral iron trivalent preparations. Used in the treatment of anemia.
Maltofer FC tab 100 mg
100's;30's
Maltofer oral drops 50 mg/mL
30 mL x 1's ($14.3/box)
Maltofer syr 50 mg/5 mL
150 mL x 1's ($18/box)



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image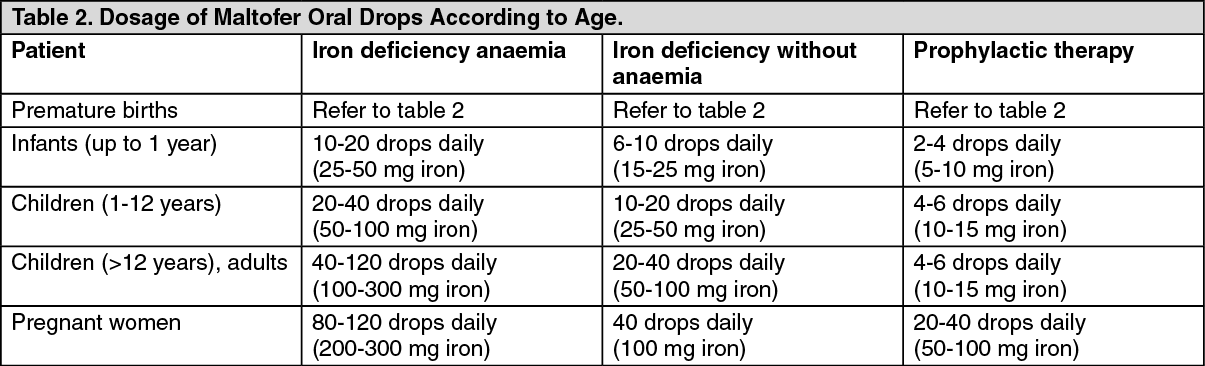 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image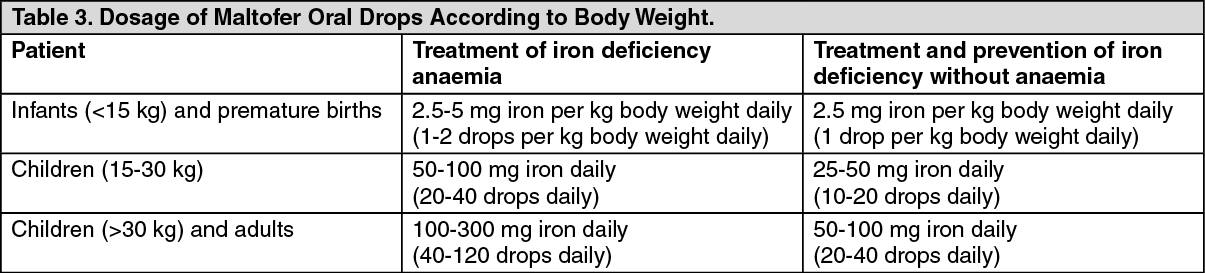 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image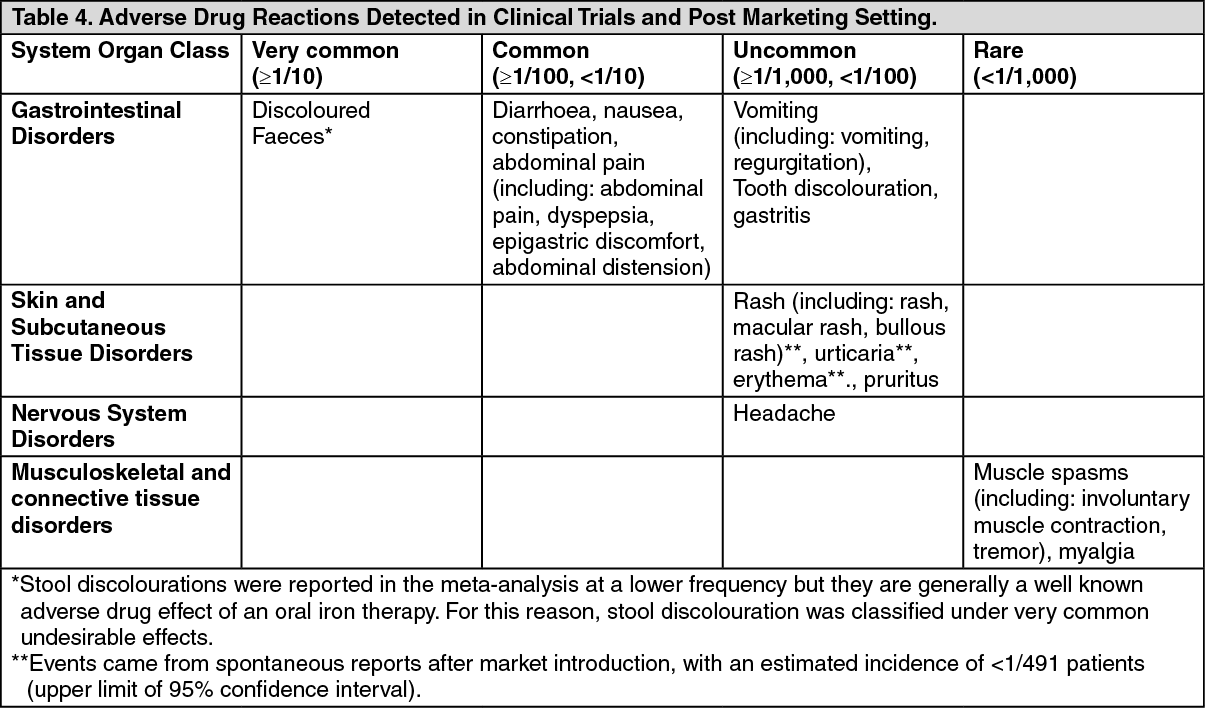 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
