Pharmacotherapeutic group: Drugs for treatment of hyperkalaemia and hyperphosphatemia.
ATC code: V03AE10.
Pharmacology: Pharmacodynamics: Mechanism of action: LOKELMA is a non-absorbed, non-polymer inorganic powder with a uniform micropore structure that preferentially captures potassium in exchange for hydrogen and sodium cations. LOKELMA is highly selective for potassium ions, even in the presence of other cations such as calcium and magnesium,
in vitro. LOKELMA captures potassium throughout the entire GI tract and reduces the concentration of free potassium in the GI lumen, thereby lowering serum potassium levels and increasing faecal potassium excretion to resolve hyperkalaemia.
Pharmacodynamic effects: LOKELMA reduces serum potassium levels as soon as 1 hour after ingestion and serum potassium concentrations continue to decline over the 48-hour treatment period. Sodium zirconium cyclosilicate has no effect on serum calcium, magnesium, and sodium levels. In patients not continuing treatment, potassium levels increase. There is a close correlation between starting serum potassium levels and effect size; patients with higher starting serum potassium levels have greater reductions in serum potassium.
In a study of healthy subjects given LOKELMA 5 g or 10 g once daily for four days, dose-dependent reduction in serum potassium concentration and total urinary potassium excretion were accompanied by mean increases in faecal potassium excretion. No statistically significant changes in urinary sodium excretion were observed.
LOKELMA has also been shown to bind ammonium
in vitro and
in vivo, thereby removing ammonium and increasing serum bicarbonate levels. LOKELMA treated-patients experienced an increase of 1.1 mmol/L at 5 g once daily, 2.3 mmol/L at 10 g once daily, and 2.6 mmol/L at 15 g once daily in bicarbonate compared with a mean increase of 0.6 mmol/L for those receiving placebo. LOKELMA demonstrated a reduction in serum aldosterone levels (range: -30% to -31%) compared with the placebo group (+14%). No effect on systolic and diastolic blood pressure has been observed.
In addition, mean reductions in BUN (blood urea nitrogen) were observed in the 5 g (-1.1 mg/dl) and 10 g (-2.0 mg/dl) three times daily groups compared with small mean increases in the placebo (0.8 mg/dl) and low dose LOKELMA (0.3 mg/dl) groups.
Clinical efficacy and safety: The potassium-lowering effects of LOKELMA have been demonstrated in three randomised, double-blind, placebo-controlled trials in patients with hyperkalaemia. All three studies tested the initial effect of LOKELMA to correct hyperkalaemia during a 48-hour period and two studies also tested maintenance of normokalaemia effect obtained. In addition, two open-label maintenance studies tested long-term safety of LOKELMA. The maintenance studies included patients with chronic kidney disease (58%), heart failure (10%), diabetes mellitus (62%), and RAAS inhibitor therapy (68%). One thousand seven hundred sixty patients have received doses of LOKELMA; 507 exposed for at least 360 days. In addition, the efficacy and safety of LOKELMA was studied in a double-blind placebo-controlled trial of 196 chronic haemodialysis patients with hyperkalaemia, who received doses of LOKELMA for 8 weeks. In the studies, LOKELMA reduced serum potassium and maintained normal serum potassium levels regardless of the underlying cause of hyperkalaemia, age, sex, race, comorbid disease, or concomitant use of RAAS inhibitors. No dietary restrictions were imposed; patients were instructed to continue their usual diet without any specified alterations.
A two-phase, randomised, double-blind placebo-controlled study: In this study, 753 patients (mean age 66 years, range 22 to 93 years) with hyperkalaemia (5.0 - ≤6.5 mmol/L, baseline potassium average 5.3 mmol/L) were randomised to receive LOKELMA 1.25 g, 2.5 g, 5 g, or 10 g or placebo three times a day for the initial 48 hours.
LOKELMA showed dose-dependent reductions in serum potassium at the 2.5 g, 5 g, and 10 g doses within hours of administration of the first dose (Table 1). Statistically significant reductions in potassium were observed 1 hour after the first 10 g dose of LOKELMA. Mean serum potassium reduction was -0.7 mmol/L and 86% of patients had normal potassium values within 48 hours at the 10 g dose. Patients with higher starting potassium levels had a greater response to LOKELMA. Patients with pre-treatment potassium levels in excess of 5.5 mmol/L (average baseline 5.8 mmol/L) saw an average decrease of 1.1 mmol/L at 48 hours while those with starting potassium levels at or below 5.3 mmol/L had an average decrease of 0.6 mmol/L at the highest dose. Potassium reduction was similar among patients with chronic kidney disease, heart failure, diabetes mellitus, and those taking RAAS inhibitor therapy (angiotensin receptor blockers, angiotensin converting enzyme inhibitors, aldosterone antagonists). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients achieving normokalaemia (potassium levels between 3.5 and 5.0 mmol/L) were then re-randomised to active drug at the same dose level or placebo administered once daily for 12 days (Table 2). This phase of the study met the predefined efficacy endpoints at the 2.5 g, 5 g, and 10 g doses when compared with their respective placebo groups. Efficacy was consistent across pre-specified subgroups with heart failure, chronic kidney disease, and diabetes mellitus, or in patients on RAAS inhibitors. At the end of the treatment period, when LOKELMA was no longer administered, potassium increased to near baseline levels. (See Table 2.)
Click on icon to see table/diagram/image
A multi-phase, placebo-controlled maintenance study with extension: In the correction phase of the study, 258 patients with hyperkalaemia (baseline average 5.6, range 4.1-7.2 mmol/L) received 10 g of LOKELMA administered three times daily for 48 hours. Reductions in potassium were observed 1 hour after the first 10 g dose of LOKELMA. Median time to normokalaemia was 2.2 hours with 84% of patients achieving normokalaemia within 24 hours and 98% within 48 hours. Responses were larger in patients with more severe hyperkalaemia; serum potassium fell 0.8, 1.2, and 1.5 mmol/L in patients with baseline serum potassium <5.5, 5.5-5.9, and ≥6.0 mmol/L, respectively.
Patients who achieved normokalaemia (potassium levels between 3.5 and 5.0 mmol/L) were randomised in a double-blind fashion to one of three doses of LOKELMA (5 g (n=45), 10 g (n=51), or 15 g (n=56)), or placebo (n=85) administered once daily for 28 days (the double-blind randomised withdrawal phase).
The proportion of subjects with average serum potassium <5.1 mmol/L from Study Day 8 to 29 was greater at the 5 g, 10 g, and 15 g once daily doses of LOKELMA (80%, 90%, and 94%, respectively), compared with placebo (46%). There was a mean decrease in serum potassium of 0.77 mmol/L, 1.10 mmol/L, 1.19 mmol/L, and 0.44 mmol/L in the 5 g, 10 g, 15 g once daily doses of LOKELMA and placebo groups, respectively, and the proportion of subjects who remained normokalaemic was 71%, 76%, 85% and 48% in the 5 g, 10 g, 15 g once daily doses of LOKELMA and placebo groups, respectively.
Extended maintenance phase (open-label) results: 123 patients entered the 11-month open-label phase. The proportion of subjects with average serum potassium < 5.1 mmol/L was 88%, the average serum potassium level was 4.66 mmol/L and the proportion of serum potassium measurements below 3.5 mmol/L was less than 1%; between 3.5 and 5.1 mmol/L was 77%; or between 3.5 and 5.5 mmol/L was 93%, irrespective of other factors that might influence the serum potassium. Average serum potassium levels were 4.66 mmol/L throughout the extension. Treatment was discontinued on study exit (Day 365). Figure 1 illustrates the mean serum potassium levels over the correction and maintenance phase of the study. (See Figure 1.)
Click on icon to see table/diagram/image
A two-phase, multi-center, multi-dose, open-label safety and efficacy study: The long term (up to 12 months) effects of LOKELMA were assessed in this study in 751 subjects with hyperkalaemia (baseline average 5.59 mmol/L; range 4.3, 7.6 mmol/L). Comorbid conditions included CKD (65%), diabetes mellitus (64%), heart failure (15%), and hypertension (83%). Use of diuretics and RAAS inhibitors was reported by 51 and 70% of subjects, respectively. During the correction phase, LOKELMA was administered 10 g TID for at least 24 hours and up to 72 hours. Subjects who achieved normokalaemia (3.5-5.0 mmol/L, inclusive) within 72 hours (n=746; 99%) entered the maintenance phase of the study. All subjects in the maintenance phase received LOKELMA at a starting dose of 5 g QD which could be increased in increments of 5 g QD (to a maximum of 15 g QD) or decreased (to a minimum of 5 g QOD) based upon the titration regimen.
Normokalaemia was achieved in 494/748 (66%), 563/748 (75%) and 583/748 (78%) of subjects after 24, 48 and 72 hours of correction phase dosing with an average reduction in serum potassium was -0.81 mmol/L, -1.02 mmol/L and -1.10 mmol/L at 24 (n=748), 48 (n=104) and 72 (n=28) hours, respectively. One hundred and twenty six patients had a baseline S-K ≥ 6.0 mmol/L (mean baseline potassium 6.28 mmol/L) and these patients had a mean reduction of -1.37 mmol/L at the end of the acute phase.
The proportion of subjects with a mean serum potassium ≤ 5.1 mmol/L across the Maintenance Phase Days 85-365 was 88% (95% CI 0.857, 0.908) and ≤ 5.5 mmol/L across the Maintenance Phase Days 85-365 was 99% (95% CI 0.976, 0.995). Normokalaemia was maintained while patients remained on drug and the mean serum potassium increased following discontinuation. Among those patients using RAAS inhibitors at baseline, 89% did not discontinue RAASi therapy, 74% were able to maintain the same dose during the maintenance phase and among those not on RAAS inhibitors at baseline, 14% were able to initiate this therapy. (See Figure 2.)
Click on icon to see table/diagram/image
A study in chronic kidney disease patients with hyperkalaemia: This study was a double-blind placebo-controlled dose-escalating study in 90 patients (60 LOKELMA patients; 30 controls) with baseline eGFR between 30-60 ml/min/1.73m
2 and hyperkalaemia (baseline serum potassium 5.2 mmol/L, range 4.6-6.0 mmol/L). Patients were randomised to receive escalating doses of LOKELMA (0.3 g, 3 g, and 10 g) or placebo, administered three times a day with meals for two to four days. The primary endpoint was the rate of change in serum potassium from baseline throughout the initial 2 days of treatment. The trial met the primary efficacy endpoint at the 3 g and 10 g doses of LOKELMA compared to placebo. LOKELMA at the 10 g dose and the 3 g dose resulted in mean maximal reductions of 0.92 mmol/L and 0.43 mmol/L, respectively. Twenty-four hour urine collections showed that LOKELMA decreased urinary potassium excretion from baseline; -15.8 mmol/24 hours compared to placebo +8.9 mmol/24 hours (p <0.001). Sodium excretion was unchanged relative to placebo (10 g TID, +25.4 mmol/24 hours compared to placebo +36.9 mmol/24 hours (NS)).
A randomised, double-blind, placebo-controlled study in patients on chronic haemodialysis: In this study, 196 patients (mean age 58 years, range 20 to 86 years) with end stage renal disease on stable dialysis for at least 3 months and persistent pre-dialysis hyperkalaemia were randomised to receive LOKELMA 5 g or placebo once daily on non-dialysis days. At randomization, mean serum potassium levels were 5.8 mmol/L (range 4.2-7.3 mmol/L) in the LOKELMA group and 5.9 mmol/L (range 4.2-7.3 mmol/L) in the placebo group. To achieve pre-dialysis serum potassium level between 4.0-5.0 mmol/L during the dose adjustment period (initial 4 weeks), the dose could be adjusted weekly in 5 g increments up to 15 g once daily based on pre-dialysis serum potassium measurement after the LIDI. The dose reached at the end of the dose-adjustment period was maintained throughout the subsequent 4-week evaluation period. At the end of the dose adjustment period, 37%, 43%, and 19% of patients were on LOKELMA 5 g, 10 g and 15 g. The proportion of responders, defined as those subjects who maintained a pre-dialysis serum potassium between 4.0 and 5.0 mmol/L on at least 3 out of 4 dialysis treatments after LIDI and who did not receive rescue therapy during the evaluation period, was 41% in the LOKELMA group, and 1% in the placebo group (p < 0.001) (see Figure 3).
In post-hoc analyses the number of times patients had serum potassium between 4.0 and 5.0 mmol/L after the LIDI during the evaluation period was higher in the LOKELMA group. 24% of patients were within this range at all 4 visits in the LOKELMA group and none in the placebo group. The post-hoc analysis showed the proportion of patients who maintained serum potassium level between 3.5 and 5.5 mmol/L on at least 3 out of 4 dialysis treatments after LIDI during the evaluation period was 70% in the LOKELMA group and 21% in the placebo group.
At the end of treatment, the mean post-dialysis serum potassium level was 3.6 mmol/L (range 2.6-5.7 mmol/L) in LOKELMA group and 3.9 mmol/L (range 2.2-7.3 mmol/L) in the placebo group. There were no differences between LOKELMA and placebo groups in interdialytic weight gain (IDWG). IDWG was defined as pre-dialysis weight minus post-dialysis weight on the previous dialysis session and was measured after the LIDI. (See Figure 3.)
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: LOKELMA is an inorganic, insoluble compound that is not subject to enzymatic metabolism. In addition, clinical studies have shown it not to be systemically absorbed. An
in vivo mass balance study in rats showed that sodium zirconium cyclosilicate was recovered in the faeces with no evidence of systemic absorption. Due to these factors and its insolubility, no
in vivo or
in vitro studies have been performed to examine its effect on cytochrome P450 (CYP450) enzymes or transporter activity.
Elimination: LOKELMA is eliminated via the faeces.
Toxicology: Preclinical safety data: Preclinical data reveal no hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, toxicity to reproduction, and development. Carcinogenicity studies have not been conducted.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image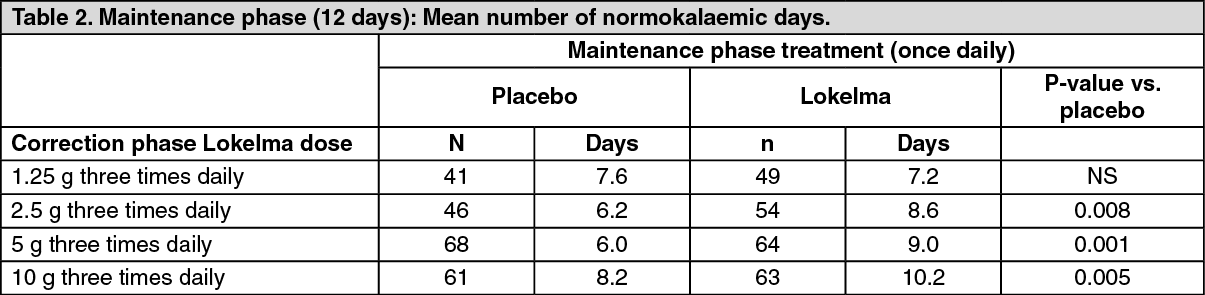 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image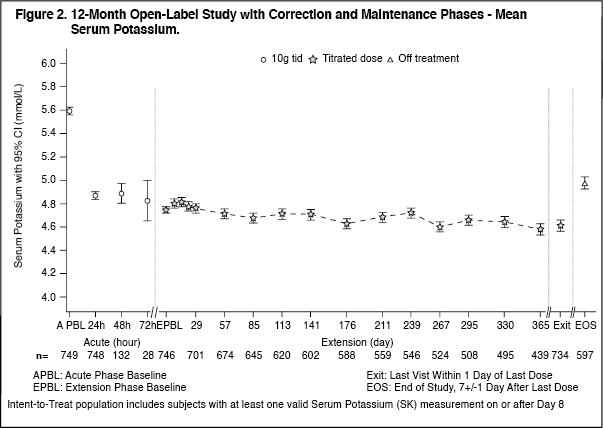 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image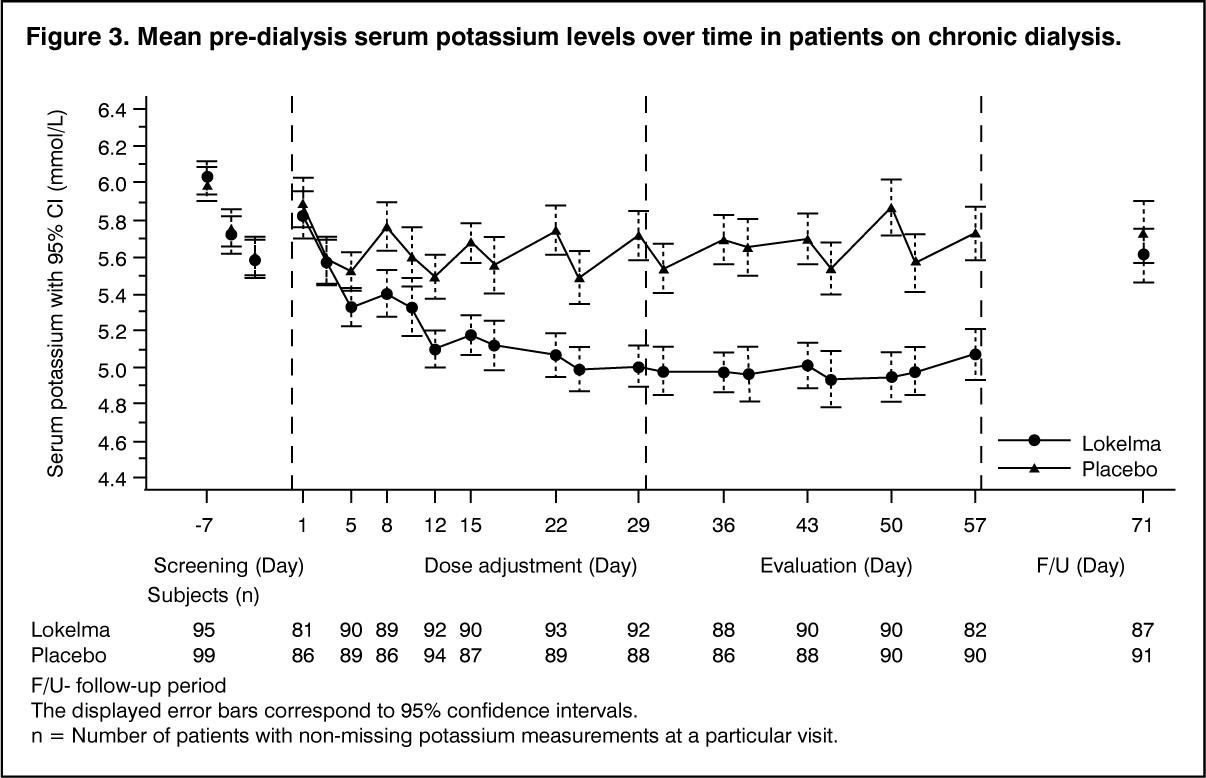 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
