Pharmacology: Mechanism of Action: Levofloxacin is the L-isomer of the racemate, ofloxacin, a quinolone antimicrobial agent. The antibacterial activity of ofloxacin resides primarily in the L-isomer. The mechanism of action of levofloxacin and other fluoroquinolone antimicrobials involves inhibition of bacterial topoisomerase IV and DNA gyrase (both of which are type II topoisomerases), enzymes required for DNA replication, transcription, repair and recombination.
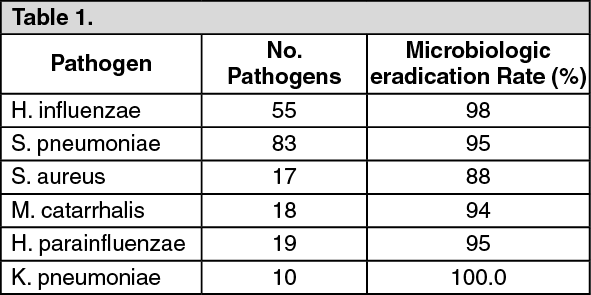
Clinical Studies: Community Acquired Bacterial Pneumonia: Adults inpatients and outpatients with a diagnosis of Community Acquired Bacterial Pneumonia were evaluated in two pivotal clinical studies. In the first study, 590 patients were enrolled in a prospective, multi center unblinded randomized trail comparing levofloxacin 500 mg once daily orally or intravenously for 7 to 14 days to ceftriaxone 1 to 2 grams intravenously once or in equally divided doses twice daily followed by cefuroxime axetil 500 mg orally twice daily for a total of 7 to 14 days. Patients assigned to treatment with the control regimen were allowed to receive erythromycin (or doxycycline if intolerant of erythromycin) if an infection due to atypical pathogens was suspected or proven. Clinical and microbiological evaluations were performed during treatment, 5 to 7 days posttherapy, and 3 to 4 weeks posttherapy. Clinical success (cure plus improvement) with levofloxacin at 5 to 7 days posttherapy, the primary efficacy variable in this study, was superior (95%) to the control group (83%). [95% CI of -19, -6]. In the second study 264 patients were enrolled in a prospective, multi center, non-comparative trial of 500 mg levofloxacin administered orally or intravenously once daily for 7 to 14 days. Clinical success for clinically evaluable patients was 93%. For both studies, the clinical success rate in patients with atypical pneumonia due to
Chlamydia pneumoniae.
Mycoplasma pneumoniae, and
Legionella pneumophila were 96%, 96%, and 70%, respectively. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additional studies were initiated to evaluated the utility of levofloxacin in community acquired pneumonia, with particular interest in penicillin-resistant strains (MIC value for penicillin ≥ 2μg/mL). In addition to the studies previously discussed. Inpatients and outpatients with mild to severe community acquired pneumonia were evaluated in six additional clinical studies: one double blind study, two open label randomized studies, and three open label non-comparative studies. The total number of clinically evaluable patients with
S. pneumoniae across all 6 studies was 250 for levofloxacin 41 for comparators. The Clinical success rate (cured or improved) among the 250 levofloxacin treated patients with
S. pneumoniae was 245/250 (98%). The Clinical success rate among the 41 comparator-treated patients with
S. pneumoniae was 39/41(95%). Across these 6 studies, 18 levofloxacin treated and 4 non quinolone comparator treated patients with community acquired pneumonia due to penicillin-resistant
S. pneumoniae (MIC value for penicillin ≥ 2 μg/mL) were identified, of the 18 levofloxacin treated patients, 15 were evaluable following the completion of therapy, fifteen out of the 15 evaluable levofloxacin treated patients with community acquired pneumonia due to penicillin-resistant
S. pneumoniae achieved clinical success (cure or improvement). Of these 15 patients, 6 were bacterial and 5 were classified as having severe disease. Of the 4 comparator treated patients with community acquired pneumonia due to penicillin-resistant
S. pneumoniae, 3 were evaluable for clinical efficacy. Three out of the 3 evaluable comparator treated patients achieved clinical success. All three of the comparator treated patients were bacteria and had disease classified as severe.
Nosocomial Pneumonia: Adult patients with clinically and radiologically documented nosocomial pneumonia were enrolled in a multicenter, randomized, open-label study comparing intravenous levofloxacin (750 mg once daily) followed by oral levofloxacin (750 mg once daily) for a total of 7-15 days to intravenous imipenem/cilastatin (500-1000 mg every 6-8 hours daily) followed by oral ciprofloxacin (750 mg every 12 hours daily) for a total of 7-15 days. Levofloxacin-treated patients received an average of 7 days of intravenous therapy (range: 1-16 days); comparator-treated patients received an average of 8 days of intravenous therapy (range: 1-19 days).
Overall, in the clinically and microbiologically evaluable population, adjunctive therapy was empirically initiated at study entry in 56 of 93 (60.2%) patients in the levofloxacin arm and 53 of 94 (56.4%) patients in the comparator arm. The average duration of adjunctive therapy was 7 days in the levofloxacin arm and 7 days in the comparator. In clinically and microbiologically evaluable patients with documented
Pseudomonas aeruginosa infection, 15 of 17 (88.2%) received ceftazidime (N=11) or piperacillin/tazobactam (N=4) in the levofloxacin arm and 16 of 17 (94.1%) received an aminoglycoside in the comparator arm. Overall, in clinically and microbiologically evaluable patients, vancomycin was added to the treatment regimen of 37 of 93 (39.8%) patients in the levofloxacin arm and 28 of 94 (29.8%) patients in the comparator arm for suspected methicillin-resistant
S. aureus infection.
Clinical success rates in clinically and microbiologically evaluable patients at the post-therapy visit (primary study endpoint assessed on day 3-15 after completing therapy) were 58.1% for levofloxacin and 60.6% for comparator. The 95% CI for the difference of response rates (levofloxacin minus comparator) was [-17.2, 12.0]. The microbiological eradication rates at the posttherapy visit were 66.7% for levofloxacin and 60.6% for comparator. The 95% CI for the difference of eradication rates (levofloxacin minus comparator) was [-8.3, 20.3]. Clinical success and microbiological eradication rates by pathogen are detailed as follows. (See Table 2.)
Click on icon to see table/diagram/image
Complicated Skin and Skin Structure Infections: Three hundred ninety-nine patients were enrolled in an open-label, randomized, comparative study for complicated skin and skin structure infections. The patients were randomized to receive either levofloxacin 750 mg once daily (IV followed by oral), or an approved comparator for a median of 10 ± 4.7 days. As is expected in complicated skin and skin structure infections, surgical procedures were performed in the levofloxacin and comparator groups. Surgery (incision and drainage or debridement) was performed on 45% of the levofloxacin-treated patients and 44% of the comparator-treated patients, either shortly before or during antibiotic treatment and formed an integral part of therapy for this indication. Among those who could be evaluated clinically 2-5 days after completion of study drug, overall success rates (improved or cured) were 116/138 (84.1%) for patients treated with levofloxacin and 106/132 (80.3%) for patients treated with the comparator.
Success rates varied with the type of diagnosis ranging from 68% in patients with infected ulcers to 90% in patients with infected wounds and abscesses. These rates were equivalent to those seen with comparator drugs.
Chronic Bacterial Prostatitis: Adult patients with a clinical diagnosis of prostatitis and microbiological culture results from urine sample collected after prostatic massage (VB3) or expressed prostatic secretion (EPS) specimens obtained via the Meares-Stamey procedure were enrolled in a multicenter, randomized, double-blind study comparing oral levofloxacin 500 mg, once daily for a total of 28 days to oral ciprofloxacin 500 mg, twice daily for a total of 28 days. The primary efficacy endpoint was microbiologic efficacy in microbiologically evaluable patients. A total of 136 and 125 microbiologically evaluable patients were enrolled in the levofloxacin and ciprofloxacin groups, respectively. The microbiologic eradication rate by patient infection at 5-18 days after completion of therapy was 75.0% in the levofloxacin group and 76.8% in the ciprofloxacin group (95% CI [-12.58, 8.98] for levofloxacin minus ciprofloxacin). The overall eradication rates for pathogens of interest are presented as follows. (See Table 3.)
Click on icon to see table/diagram/image
Eradication rates for
S. epidermidis when found with other co-pathogens are consistent with rates seen in pure isolates. Clinical success (cure + improvement with no need for further antibiotic therapy) rates in microbiologically evaluable population 5-18 days after completion of therapy were 75.0% for levofloxacin-treated patients and 72.8% for ciprofloxacin-treated patients (95% CI [-8.87, 13.27] for levofloxacin minus ciprofloxacin). Clinical long-term success (24-45 days after completion of therapy) rates were 66.7% for the levofloxacin-treated patients and 76.9% for the ciprofloxacin-treated patients (95% CI [-23.40, 2.89] for levofloxacin minus ciprofloxacin).
Pharmacokinetics: The mean ±SD pharmacokinetic parameters of levofloxacin determined under single and steady-state conditions following oral tablet doses of Levofloxacin.
Absorption: Levofloxacin is rapidly and essentially completely absorbed after oral administration. Peak plasma concentrations are usually attained one to two hours after oral dosing. The absolute bioavailability of levofloxacin from a 500 mg tablet and a 750 mg tablet of levofloxacin are both approximately 99%, demonstrating complete oral absorption of levofloxacin.
Levofloxacin pharmacokinetics are linear and predictable after single and multiple oral dosing regimens. Steady-state conditions are reached within 48 hours following a 500 mg or 750 mg once-daily dosage regimen. The mean ±SD peak and trough plasma concentrations attained following multiple once-daily oral dosage regimens were approximately 5.7 ±1.4 and 0.5 ±0.2 mcg/mL after the 500 mg doses, and 8.6 ±1.9 and 1.1 ±0.4 mcg/mL after the 750 mg doses, respectively. Oral administration of a 500 mg dose of levofloxacin with food prolongs the time to peak concentration by approximately 1 hour and decreases the peak concentration by approximately 14%. Therefore, levofloxacin Tablets can be administered without regard to food.
Distribution: The mean volume of distribution of levofloxacin generally ranges from 74 to 112 L after single and multiple 500 mg or 750 mg doses, indicating widespread distribution into body tissues. Levofloxacin reaches its peak levels in skin tissues and in blister fluid of healthy subjects at approximately 3 hours after dosing. The skin tissue biopsy to plasma AUC ratio is approximately 2 and the blister fluid to plasma AUC ratio is approximately 1 following multiple once-daily oral administration of 750 mg and 500 mg doses of Levofloxacin respectively, to healthy subjects. Levofloxacin also penetrates well into lung tissues. Lung tissue concentrations were generally 2- to 5-fold higher than plasma concentrations and ranged from approximately 2.4 to 11.3 mcg/g over a 24-hour period after a single 500 mg oral dose.
In vitro, over a clinically relevant range (1 to 10 mcg/mL) of serum/plasma levofloxacin concentrations, levofloxacin is approximately 24 to 38% bound to serum proteins across all species studied, as determined by the equilibrium dialysis method. Levofloxacin is mainly bound to serum albumin in humans. Levofloxacin binding to serum proteins is independent of the drug concentration.
Metabolism: Levofloxacin is stereochemically stable in plasma and urine and does not invert metabolically to its enantiomer, D-ofloxacin. Levofloxacin undergoes limited metabolism in humans and is primarily excreted as unchanged drug in the urine. Following oral administration, approximately 87% of an administered dose was recovered as unchanged drug in urine within 48 hours, whereas less than 4% of the dose was recovered in feces in 72 hours. Less than 5% of an administered dose was recovered in the urine as the desmethyl and N-oxide metabolites, the only metabolites identified in humans. These metabolites have little relevant pharmacological activity.
Excretion: Levofloxacin is excreted largely as unchanged drug in the urine. The mean terminal plasma elimination half-life of levofloxacin ranges from approximately 6 to 8 hours following single or multiple doses of levofloxacin given orally. The mean apparent total body clearance and renal clearance range from approximately 144 to 226 mL/min and 96 to 142 mL/min, respectively. Renal clearance in excess of the glomerular filtration rate suggests that tubular secretion of levofloxacin occurs in addition to its glomerular filtration. Concomitant administration of either cimetidine or probenecid results in approximately 24% and 35% reduction in the levofloxacin renal clearance, respectively, indicating that secretion of levofloxacin occurs in the renal proximal tubule. No levofloxacin crystals were found in any of the urine samples freshly collected from subjects receiving Levofloxacin.
Geriatric: There are no significant differences in levofloxacin pharmacokinetics between young and elderly subjects when the subjects' differences in creatinine clearance are taken into consideration. Following a 500 mg oral dose of Levofloxacin to healthy elderly subjects (66 - 80 years of age), the mean terminal plasma elimination half-life of levofloxacin was about 7.6 hours, as compared to approximately 6 hours in younger adults. The difference was attributable to the variation in renal function status of the subjects and was not believed to be clinically significant. Drug absorption appears to be unaffected by age. Levofloxacin dose adjustment based on age alone is not necessary.
Gender: There are no significant differences in levofloxacin pharmacokinetics between male and female subjects when subjects' differences in creatinine clearance are taken into consideration. Following a 500 mg oral dose of Levofloxacin to healthy male subjects, the mean terminal plasma elimination half-life of levofloxacin was about 7.5 hours, as compared to approximately 6.1 hours in female subjects. This difference was attributable to the variation in renal function status of the male and female subjects and was not believed to be clinically significant. Drug absorption appears to be unaffected by the gender of the subjects. Dose adjustment based on gender alone is not necessary.
Race: The effect of race on levofloxacin pharmacokinetics was examined through a covariate analysis performed on data from 72 subjects: 48 white and 24 non-white. The apparent total body clearance and apparent volume of distribution were not affected by the race of the subjects.
Renal Impairment: Clearance of levofloxacin is substantially reduced and plasma elimination half-life is substantially prolonged in adult patients with impaired renal function (creatinine clearance < 50 mL/min), requiring dosage adjustment in such patients to avoid accumulation. Neither hemodialysis nor continuous ambulatory peritoneal dialysis (CAPD) is effective in removal of levofloxacin from the body, indicating that supplemental doses of Levofloxacin are not required following hemodialysis or CAPD (see Dosage & Administration).
Hepatic Impairment: Pharmacokinetic studies in hepatically impaired patients have not been conducted. Due to the limited extent of levofloxacin metabolism, the pharmacokinetics of levofloxacin are not expected to be affected by hepatic impairment.
Bacterial Infection: The pharmacokinetics of levofloxacin in patients with serious community-acquired bacterial infections are comparable to those observed in healthy subjects.
Drug-Drug Interactions: The potential for pharmacokinetic drug interactions between Levofloxacin and antacids, warfarin, theophylline, cyclosporine, digoxin, probenecid, and cimetidine has been evaluated (see Interactions).



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image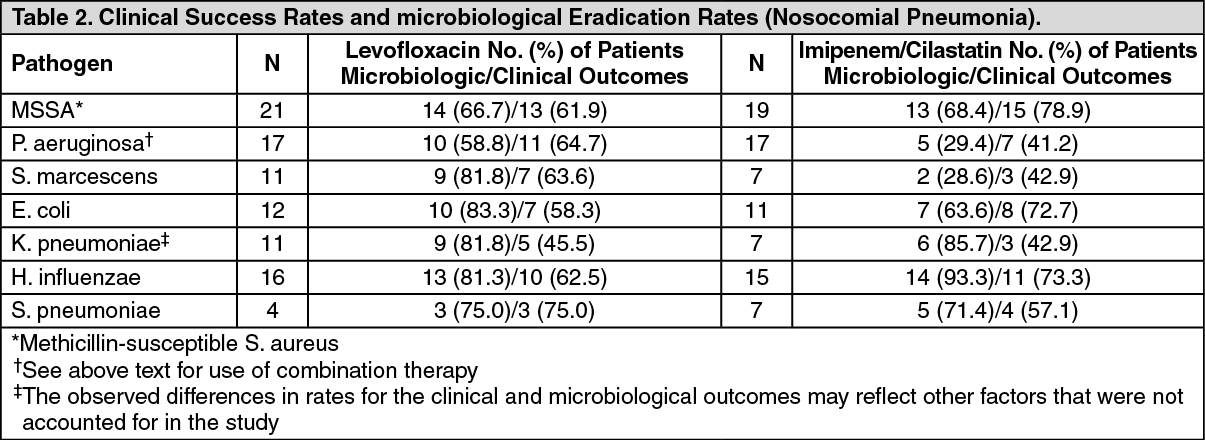 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image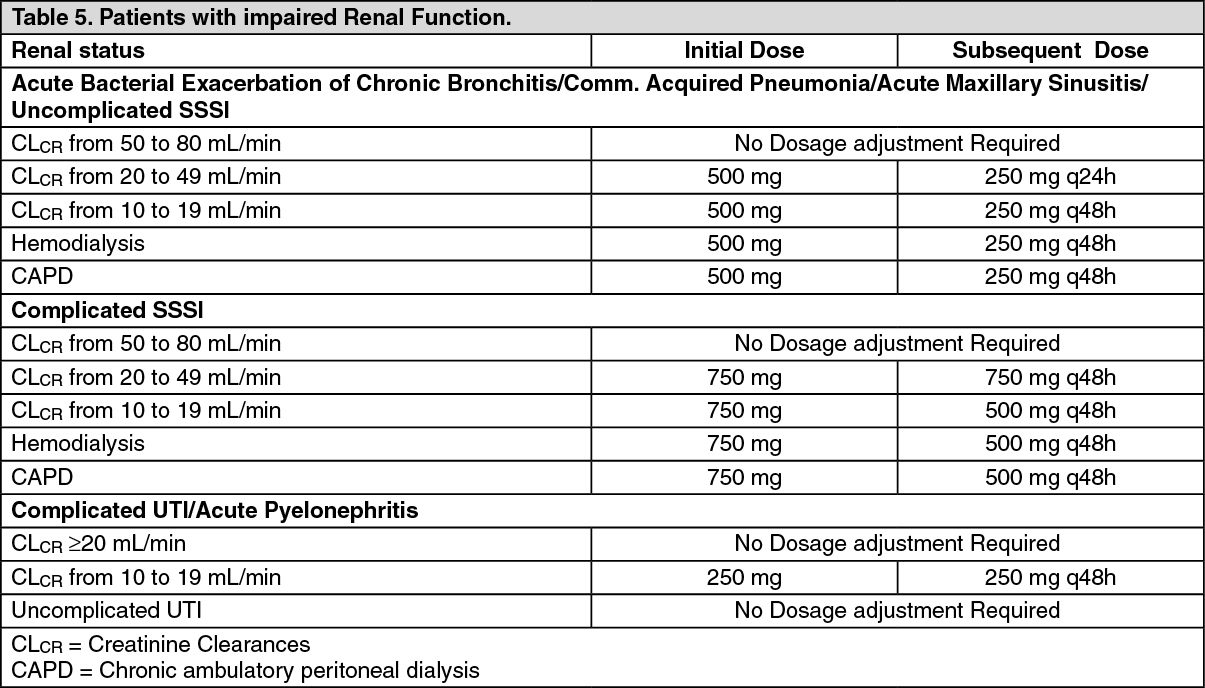 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
