


 Sign Out
Sign Out


Episodes of diarrhoea, mostly mild and transient, have been reported in patients treated with deferiprone. Gastrointestinal effects are more frequent at the beginning of therapy and in most patients resolve within a few weeks without the discontinuation of treatment. In some patients it may be beneficial to reduce the dose of deferiprone and then scale it back up to the former dose. Arthropathy events, which ranged from mild pain in one or more joints to severe arthritis with effusion and significant disability, have also been reported in patients treated with deferiprone. Mild arthropathies are generally transient.
Increased levels of serum liver enzymes have been reported in patients taking deferiprone. In the majority of these patients, the increase was asymptomatic and transient, and returned to baseline without discontinuation or decreasing the dose of deferiprone (see Precautions).
Some patients experienced progression of fibrosis associated with an increase in iron overload or hepatitis C.
Low plasma zinc levels have been associated with deferiprone, in a minority of patients. The levels normalised with oral zinc supplementation.
Neurological disorders (such as cerebellar symptoms, diplopia, lateral nystagmus, psychomotor slowdown, hand movements and axial hypotonia) have been observed in children who had been voluntarily prescribed approximately 2.5-times the maximum recommended dose of 100 mg/kg/day for several months. Episodes of hypotonia, instability, inability to walk, and hypertonia with inability of limb movement, have been reported in children in the post-marketing setting with standard doses of deferiprone. The neurological disorders progressively regressed after deferiprone discontinuation (see Precautions and Overdosage).
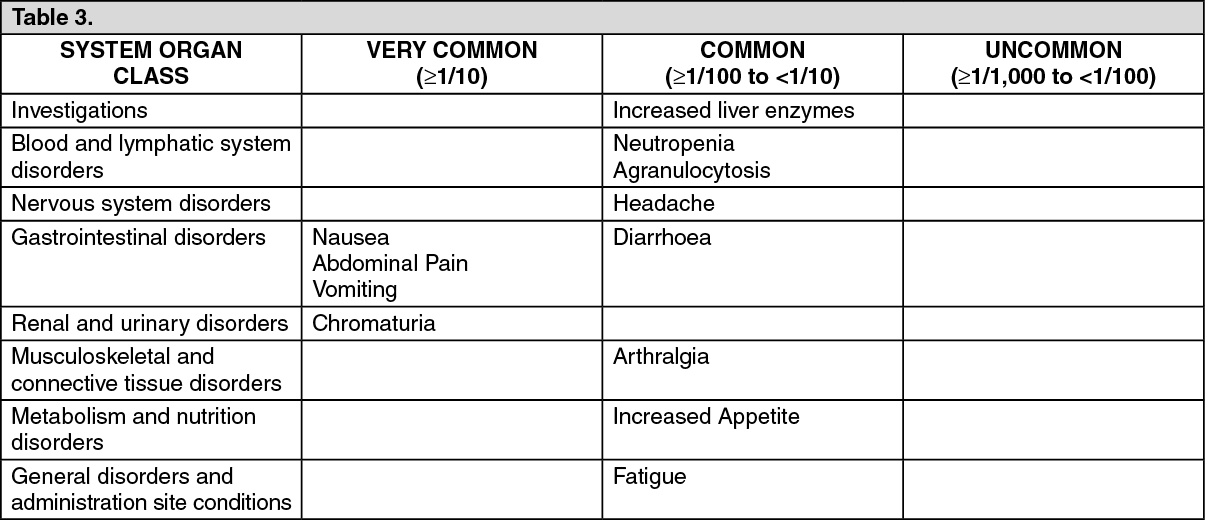
Adverse reaction frequencies: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form