Smoking and age: Cigarette smoking increases the risk of serious cardiovascular events from hormonal contraceptive use. This risk increases with age, particularly in women over 35 years of age, and with the number of cigarettes smoked. For this reason, hormonal contraceptives, including EVRA, should not be used by women who are over 35 years of age and smoke.
Body weight ≥ 90 kg: Analyses of phase III data suggest that EVRA may be less effective in users with body weight ≥ 90 kg than in users with lower body weights. Below 90 kg there was no association between body weight and pregnancy.
General: In case of undiagnosed, persistent or recurrent abnormal vaginal bleeding, appropriate measures should be taken to rule out malignancy.
When EVRA was used correctly in clinical trials, the chance of becoming pregnant was less than 1% in the first year of use. The chance of becoming pregnant increases with dosing errors.
Pre-existing conditions: When weighing the risks/benefits of hormonal contraceptive use, the physician should be familiar with the following conditions that may increase the risk of complications associated with hormonal contraceptive use: Conditions which increase the risk of developing venous thrombo-embolic complications, e.g. prolonged immobilization or major surgery, leg surgery or leg cast, obesity, family history of thrombo-embolic disease, inflammatory bowel diseases such as Crohn's disease or ulcerative colitis.
Risk factors for arterial disease, e.g. smoking, hyperlipidemia, hypertension (persistent blood pressure values ≥ 140 mm Hg systolic or ≥ 90 mm Hg diastolic), obesity, or conditions which increase the risk of arterial thromboembolic complications such as systemic lupus erythematosus.
Severe migraine without aura; Diabetes mellitus; Severe depression or a history of this condition; Presence or history of cholelithiasis; Chronic Idiopathic Jaundice; Family history of cholestatic jaundice (e.g. Rotor, Dubin-Johnson Syndrome).
Thromboembolic and other vascular disorders: An increased risk of thromboembolic and thrombotic disease that could lead to permanent disability or death has been associated with the use of hormonal contraceptives and is well established. Case control studies have found the relative risk of users compared to non-users to be 3 for the first episode of superficial venous thrombosis, 4 to 11 for deep vein thrombosis or pulmonary embolism, and 1.5 to 6 for users with predisposing conditions for venous thromboembolic disease. Studies have shown the relative risk to be somewhat lower, about 3 for new cases and about 4.5 for new cases requiring hospitalization. The risk of thromboembolic disease associated with hormonal contraceptives returns to baseline after the combined hormonal contraceptive (CHC) use is stopped. Venous thromboembolism (VTE) risk is highest in the first ever year of use. There is also some evidence that the risk of VTE when a CHC is re-started after ≥4 weeks of discontinuation is at least as high as the risk of VTE when a CHC is initially started.
Epidemiologic, case-control studies were conducted in the U.S. using healthcare claims data to evaluate the risk of VTE among women aged 15-44 who used EVRA (a transdermal patch bioequivalent to EVRA) compared to women who used oral contraceptives containing 30-35 mcg of ethinyl estradiol (EE) and either norgestimate (NGM) or levonorgestrel (LNG). NGM is the prodrug for norelgestromin, the progestin in EVRA. These studies (see Table 2) used slightly different designs and reported odds ratios ranging from 0.9 (indicating no increase in risk) to 2.5 (indicating an approximate doubling of risk). One study (i3 Ingenix) included patient chart review to confirm the VTE occurrence. Two studies using different databases were conducted by the Boston Collaborative Drug Surveillance Program (BCDSP) with LNG-containing oral contraceptives as the comparator. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
As with any combination hormonal contraceptive, the clinician should be alert to the earliest manifestations of thromboembolic disorders (thrombophlebitis, VTE including pulmonary embolism, cerebrovascular disorders, and retinal thrombosis). Should any of these occur or be suspected, EVRA should be discontinued immediately.
A two- to four-fold increase in the relative risk of post-operative thromboembolic complications has been reported with the use of hormonal contraceptives. The relative risk of venous thrombosis in users who have predisposing conditions is twice that of users without such medical conditions. If feasible, hormonal contraceptives should be discontinued at least four weeks prior to and for two weeks after elective surgery of a type associated with an increase in risk of thromboembolism and during and following prolonged immobilization. Since the immediate postpartum or post-abortion period is also associated with an increased risk of thromboembolism, hormonal contraceptives should be started as described in the Use after Childbirth and Use after Abortion or Miscarriage under Dosage & Administration.
The relative risk of arterial thromboses (e.g. stroke, myocardial infarction) is increased by the presence of other predisposing factors such as cigarette smoking, hypertension, hypercholesterolemia, obesity, diabetes, history of pre-eclamptic toxemia and increasing age. Hormonal contraceptives have been associated with these serious vascular complications. The risk of vascular disease may be less severe with hormonal contraceptive formulations containing lower dosages of estrogen and progestogen, although this has not been conclusively established.
The risk of serious cardiovascular side effects increases with age and with heavy smoking and is quite marked in smokers over 35 years of age. Users of hormonal contraceptives should be strongly advised not to smoke.
Due to the vague symptomatology of many thromboembolic events, hormonal contraceptives should be discontinued in cases of suspected thromboses while diagnostic interventions are being pursued.
There have been clinical reports of retinal thrombosis associated with the use of hormonal contraceptives. Hormonal contraceptives should be discontinued if there is unexplained partial or complete loss of vision; onset of proptosis or diplopia; papilledema or retinal vascular lesions. Appropriate diagnostic and therapeutic measures should be undertaken immediately.
The use of any combined hormonal contraceptives (CHCs) increases the risk of venous thromboembolism (VTE) compared with no use. Products that contain levonorgestrel, norgestimate or norethisterone are associated with the lowest risk of VTE. Other products such as EVRA may have up to twice this level of risk. The decision to use any product other than one with the lowest VTE risk should be taken only after a discussion with the woman to ensure she understands the risk of VTE with EVRA, how her current risk factors influence this risk, and that her VTE risk is highest in the first ever year of use. There is also some evidence that the risk is increased when a CHC is re-started after a break in use of 4 weeks or more.
In women who do not use a CHC and are not pregnant, about 2 out of 10,000 will develop a VTE over the period of one year. However, in any individual woman, the risk may be far higher, depending on her underlying risk factors.
It is estimated that out of 10,000 women who use a CHC containing norelgestromin, between 6 to 12 women will develop a VTE in one year; this compares with about 6 in women who use a levonorgestrel-containing CHC.
Studies have suggested that the incidence of VTE in women who used EVRA is up to 2-fold higher than in users of CHCs that contain levonorgestrel.
Extremely rarely, thrombosis has been reported to occur in other blood vessels, e.g. hepatic, mesenteric, renal or retinal veins and arteries, in CHC users.
Hypertension: An increase in blood pressure (BP) has been reported in some users taking hormonal contraceptives. Studies indicate that this increase is more likely to occur in older hormonal contraceptive users and with extended duration of use. For many users, elevated blood pressure will return to normal after they stop taking hormonal contraceptives. There is no difference in the occurrence of hypertension between former and never users. In three contraception trials of EVRA (n = 1530, n = 819, and n = 748, respectively) mean changes from baseline in systolic and diastolic blood pressure were less than 1 mm mercury.
Users with hypertension should have their condition under control before hormonal contraceptive therapy can be started. Hormonal contraceptive therapy should be discontinued if significant persistent elevation of blood pressure (160 mm Hg systolic or ≥ 100 mm Hg diastolic) occurs and cannot be adequately controlled. In general, women who develop hypertension during hormonal contraceptive therapy should be switched to a non-hormonal contraceptive. If other contraceptive methods are not suitable, hormonal contraceptive therapy may continue combined with antihypertensive therapy. Regular monitoring of BP throughout hormonal contraceptive therapy is recommended.
Hepatobiliary disease: Benign hepatic adenomas are associated with combination hormonal contraceptive use. Indirect calculations have estimated the attributable risk to be in the range of 3.3 cases/100000 for users, a risk that increases after 4 or more years of use, especially with hormonal contraceptives containing 50 micrograms or more of estrogen. Rupture of benign hepatic adenomas may cause death through intra-abdominal hemorrhage.
Studies have shown that combination hormonal contraceptive users have an increased risk of developing hepatocellular carcinoma.
Gallbladder disease including cholecystitis and cholelithiasis has been reported with hormonal contraceptive use.
Carcinoma of the reproductive organs and breasts: Most studies suggest that use of hormonal contraceptives is not associated with an overall increase in the risk of developing breast cancer. Some studies have reported an increased relative risk of developing breast cancer, particularly at a younger age. This increased relative risk has been reported to be related to duration of use, before the first term pregnancy.
A meta-analysis of 54 epidemiological studies reports that users who are currently using combined hormonal contraceptives or have used them in the past 10 years are at a slightly increased risk of having breast cancer diagnosed, although the additional cancers tend to be localized to the breast. It is not possible to infer from these data whether the patterns of risk observed are due to an earlier diagnosis of breast cancer in ever-users, the biological effects of hormonal contraceptives, or a combination of both factors. This meta-analysis also suggests that the age at which users discontinue the use of combined hormonal contraceptives is an important risk factor for breast cancer; the older the age at stopping, the more breast cancers are diagnosed. Duration of use was considered less important.
The possible increase in risk of breast cancer should be discussed with users and weighed against the benefits of combined hormonal contraceptives, taking into account the evidence that they offer substantial protection against the risk of developing ovarian and endometrial cancer.
Some studies suggest that hormonal contraceptive use has been associated with an increased risk of cervical intraepithelial neoplasia in some populations of users. However, there continues to be controversy about the extent to which such findings may be due to differences in sexual behavior and other factors.
Metabolic effects: Hormonal contraceptives may cause a decrease in glucose tolerance. This effect has been shown to be directly related to estrogen dose. Progestogens increase insulin secretion and create insulin resistance. This effect varies with different progestational agents. However, in the non-diabetic woman, hormonal contraceptives appear to have no effect on fasting blood glucose. Because of these demonstrated effects, prediabetic and diabetic users in particular should be monitored carefully while using hormonal contraceptives.
A small proportion of women will have persistent hypertriglyceridemia while taking hormonal contraceptives. Changes in serum triglycerides and lipoprotein levels have been reported in hormonal contraceptive users.
Headache: As with all hormonal contraceptives, the following events require discontinuation of EVRA and evaluation of the cause: onset or exacerbation of migraines with or without focal aura; or development of headaches with a new pattern that is recurrent, persistent or severe.
Bleeding irregularities: Breakthrough bleeding, spotting and/or amenorrhea may be encountered in users on hormonal contraceptives, especially during the first 3 months of use. Non-hormonal causes should be considered and, if necessary, adequate diagnostic measures taken to rule out organic disease or pregnancy.
Some users may experience amenorrhea or oligomenorrhea after discontinuing hormonal contraception, especially when such a condition was pre-existent.
Chloasma: Chloasma may occasionally occur with use of hormonal contraception, especially in users with a history of chloasma gravidarum. Users with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation while using EVRA. Chloasma is often not fully reversible.
Transdermal versus oral contraceptives: Prescribers should be aware of the differences in pharmacokinetic (PK) profiles of transdermal and oral combined hormonal contraceptives and should exercise caution when making a direct comparison between these parameters. In general, transdermal patches are designed to maintain steady delivery of EE and NGMN over a seven-day period while oral contraceptives are administered on a daily basis and produce daily peaks and troughs. Inter-subject variability (%CV) for PK parameters following delivery from the patch is higher relative to the variability determined from the oral contraceptive. It is not known whether there are changes in the risk of serious adverse events based on the difference in pharmacokinetic profiles of EE in women using EVRA compared with women using oral contraceptives containing 35 micrograms of EE. Increased estrogen exposure may increase the risk of adverse events, including venous thromboembolism (see Pharmacology: Pharmacokinetics: Transdermal versus oral contraceptives under Actions).
Effects on Ability to Drive and Use Machines: None known.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image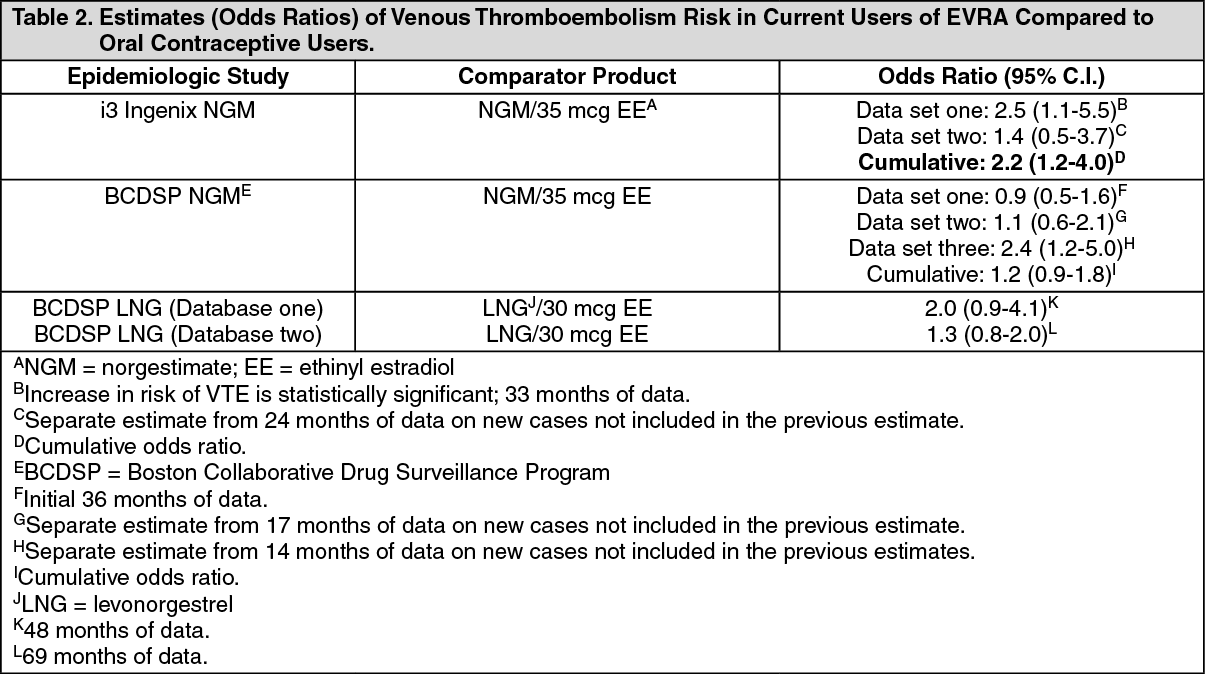 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
