Pharmacology: Pharmacodynamics: Mechanism of action: Safinamide has a selective and reversible MAO-B inhibitory effect and increases brain concentrations of intrinsic dopamine and dopamine of levodopa origin. This MAO-B inhibition is considered as the main mechanism of action of safinamide. Safinamide also has a nondopaminergic effect (glutamate release suppressive effect via a voltage-gated sodium channel inhibitory effect).
Pharmacological effect: MAO-B inhibition: For inhibitory effect of safinamide on MAO-B, IC
50 was 79 nM in the human brain and 98 nM in the rat brain, showing that MAO-B inhibition was approximately 1000-fold more potent in the human brain and approximately 6000-fold more potent in the rat brain than MAO-A inhibition (
in vitro). MAO-B inhibition of safinamide was reversible (
in vitro, in vivo).
Voltage-gated sodium channel inhibition: Safinamide inhibited a voltage-gated sodium channel in an activity-dependent manner. In human Nav subtypes (Nav 1.1 - 1.8), IC
50 was 13 - 82 μM under rest conditions and 1.6 - 4.9 μM in the inactivated state (
in vitro). In a microdialysis study in the rat hippocampus, safinamide significantly suppressed glutamate release induced by sodium channel agonists (
in vitro).
Effect in Parkinson's disease model: Although coadministration of levodopa and benserazide to rats with 6-hydroxydopamine (6-OHDA) is associated with rotary motion, multiple dosing of levodopa and benserazide reduces rotary motion (wearing-off phenomenon). Safinamide significantly reversed this reduction in rotary motion.
In a cynomolgus monkey model of Parkinson's disease induced by 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP), treatment with safinamide prolonged the duration of the therapeutic effect of levodopa on Parkinson's disease.
CLINICAL STUDIES: Clinical studies for efficacy and safety: Japanese phase 2/3 study: In a randomized, double-blind study in Japanese patients with Parkinson's disease with wearing-off phenomenon under treatment with levodopa-containing products, there was a statistically significant increase in the change in mean daily "on" time from the baseline to the last evaluation point in the safinamide 50 mg and 100 mg groups compared with the placebo group (P=0.0002 and P<0.0001, respectively). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The incidence of adverse reactions was 31.6% (42/133 subjects) in the 50 mg group and 30.3% (40/132 subjects) in the 100 mg group. Major adverse reactions were dyskinesia 8.3% (11/133 subjects), visual hallucinations 3.0% (4/133 subjects), headache 2.3% (3/133 subjects), somnolence 2.3% (3/133 subjects), and nausea 2.3% (3/133 subjects) in the 50 mg group, and dyskinesia 10.6% (14/132 subjects), visual hallucinations 4.5% (6/132 subjects), somnolence 2.3% (3/132 subjects), nausea 2.3% (3/132 subjects), decreased weight 2.3% (3/132 subjects), and decreased appetite 2.3% (3/132 subjects) in the 100 mg group.
Japanese phase 3 study: In an open-label, long-term study in Japanese patients with Parkinson's disease with wearing-off phenomenon under treatment with levodopa-containing products, the change in mean daily "on" time from the baseline with safinamide 50 to 100 mg/day (mean ± SD) was 1.05±1.74 hours (n=193) at Week 4 and 1.42±2.72 hours (n=142) at Week 52, showing a persistent effect after long-term treatment.
The incidence of adverse reactions was 38.9% (79/203 subjects). Major adverse reactions were dyskinesia 16.3% (33/203 subjects), fall 3.4% (7/203 subjects), constipation 3.0% (6/203 subjects), visual hallucinations 2.5% (5/203 subjects), insomnia 2.5% (5/203 subjects), and nausea 2.5% (5/203 subjects).
Others: Effect on QT interval: When safinamide 100 and 350 mg was administered to healthy adult subjects once daily for 6 days, the QTc interval reached a minimum 1 hour after administration, with a difference from the placebo group of -5.4 and -15.5 msec, respectively. This effect was correlated with plasma concentrations of safinamide (non-Japanese data).
Note: The approved daily dose of this drug is generally 50 mg and the maximum is 100 mg.
Pharmacokinetics: Blood Level: Single dose: When Japanese healthy adult subjects received single oral doses of safinamide 50, 100, and 200 mg under fasted condition, plasma concentrations of safinamide over time and plasma pharmacokinetic parameters of safinamide were as follows. (See figure and Table 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Multiple dose: When Japanese healthy adult subjects received multiple oral doses of safinamide 50, 100, and 200 mg once daily for 7 days under fed condition (under fasted condition on Day 7 only), plasma pharmacokinetic parameters of safinamide after the last dose were as follows. C
max and AUC after multiple doses of safinamide increased dose-proportionally. The accumulation ratio for C
max and AUC
0-24 (Day 7/Day 1) ranged 1.9 to 2.0, and no accumulation occurred at any doses, and the steady state was reached by Day 6 of treatment. (See Table 5.)
Click on icon to see table/diagram/image
Absorption: After single and multiple oral administrations to Japanese healthy adult subjects under fasted condition, safinamide was rapidly absorbed with a t
max of 1.0 to 3.5 hours. In addition, when healthy adult subjects received a single oral dose of safinamide 50 mg, the bioavailability was 95% (non-Japanese data).
A comparison of plasma pharmacokinetic parameters (C
max, t
max, t
1/2, and AUC
0-t) in Japanese healthy adult subjects (n=8) who received a single oral dose of safinamide 50 mg under fasted and fed conditions showed no food effect.
Distribution: When healthy adult subjects received a single intravenous dose of safinamide 50 mg, the distribution volume was 165 L (non-Japanese data). The plasma protein binding in humans was 89% (
in vitro).
Metabolism: The main elimination pathway of safinamide is metabolism. It was suggested that safinamide is metabolized to NW-1153 by nonspecific cytoplasm amidase and CYP3A4, MAO-A and aldehyde dehydrogenase are involved in the metabolism of safinamide to NW-1689 via intermediate products. It was estimated that the contribution of nonmicrosomal enzymes (cytoplasm amidase/MAO-A) might be greater than that of CYP3A4 to safinamide metabolic capacity (
in vitro, non-Japanese data).
Excretion: When healthy adult subjects received a single oral dose of C-safinamide 400 mg, 78% of total radioactivity was excreted (76% in urine and 1.5% in feces). A trace of unchanged safinamide was excreted in urine within 48 hours after administration, indicating that most of the administered safinamide is metabolized (non-Japanese data).
When Japanese healthy adult subjects received single oral doses of safinamide 50, 100, and 200 mg, 4.5% to 4.9% was excreted unchanged in urine by 96 hours after administration, and the cumulative urinary excretion rate of metabolites up to 96 hours after administration was 31.5% to 34.3% for propionate metabolite (NW-1153), 0.22% to 0.25% for benzoate metabolite (NW-1689), and 28.4% to 32.8% for glucuronate conjugate (NW-1689 acyl glucuronide).
Note: The approved daily dose of this drug is generally 50 mg and the maximum is 100 mg.
Patients with specific backgrounds: Patients with renal impairment: When subjects with moderate renal impairment (eGFR 30 to 59 mL/min) and subjects with severe renal impairment (eGFR of less than 30 mL/min and not requiring hemodialysis) received a single oral dose of safinamide 50 mg, plasma pharmacokinetic parameters were similar to those of subjects with normal renal function (eGFR of more than 90 mL/min) (non-Japanese data).
Patients with hepatic impairment: When subjects with mild and moderate hepatic impairment (Child-Pugh A and B) received a single oral dose of safinamide 50 mg, AUC
0-∞ was increased by 32% and 82%, respectively, compared with subjects with normal hepatic function (non-Japanese data) [see PRECAUTIONS CONCERNING DOSAGE AND ADMINISTRATION under Dosage & Administration and PRECAUTIONS CONCERNING PATIENTS WITH SPECIFIC BACKGROUNDS under Precautions].
Drug-drug interaction: Ketoconazole: When healthy adult subjects (n=14) received a multiple dose of ketoconazole (CYP3A4 inhibitor) 200 mg twice daily for 6 days and a single dose of safinamide 100 mg, C
max and AUC
0-∞ were increased by 6.6% and 12.9%, respectively, compared with safinamide alone (non-Japanese data).
Midazolam: When healthy adult subjects (n=16) received a multiple dose of safinamide 100 mg once daily for 14 days and a single dose of midazolam (CYP3A4 substrate) 7.5 mg, C
max and AUC
0-t were decreased by 2% and 20%, respectively, compared with midazolam alone (non-Japanese data).
Caffeine: When healthy adult subjects (n=16) received a multiple dose of safinamide 100 mg once daily for 14 days and a single dose of caffeine (CYP1A2 substrate) 200 mg, C
max and AUC
0-t were increased by 7% and 13%, respectively, compared with caffeine alone (non-Japanese data).
Rosuvastatin: When healthy adult subjects (n=24) received a multiple dose of safinamide 100 mg once daily for 11 days and a single dose of rosuvastatin calcium (BCRP substrate) 20 mg, C
max and AUC
0-t were increased by 29% and 21%, respectively, compared with rosuvastatin calcium alone (non-Japanese data).
Levodopa/Carbidopa: When patients with Parkinson's disease (n=24) received multiple dose of safinamide 100 mg once daily for 6 days in combination with levodopa/carbidopa, C
max and AUC
0-6 of levodopa were decreased by 0.6% and 7.2%, respectively, compared with levodopa/carbidopa alone (non-Japanese data).
Induction of CYP: In an enzyme induction study using human hepatocytes, safinamide at concentrations of ≥1 μM led to a ≥2-fold increase in CYP2B6 mRNA expression compared with a control, suggesting possible induction of CYP2B6 by safinamide (
in vitro).



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image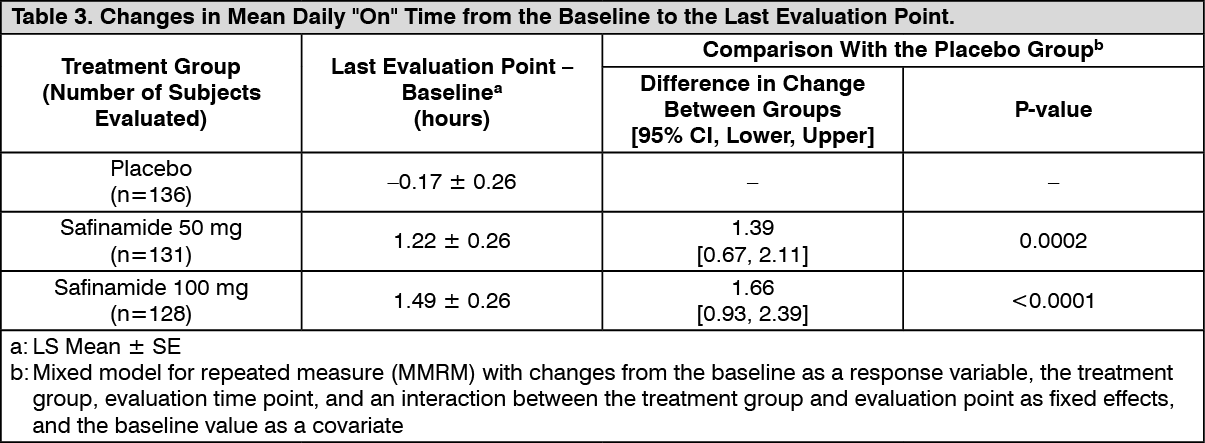 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image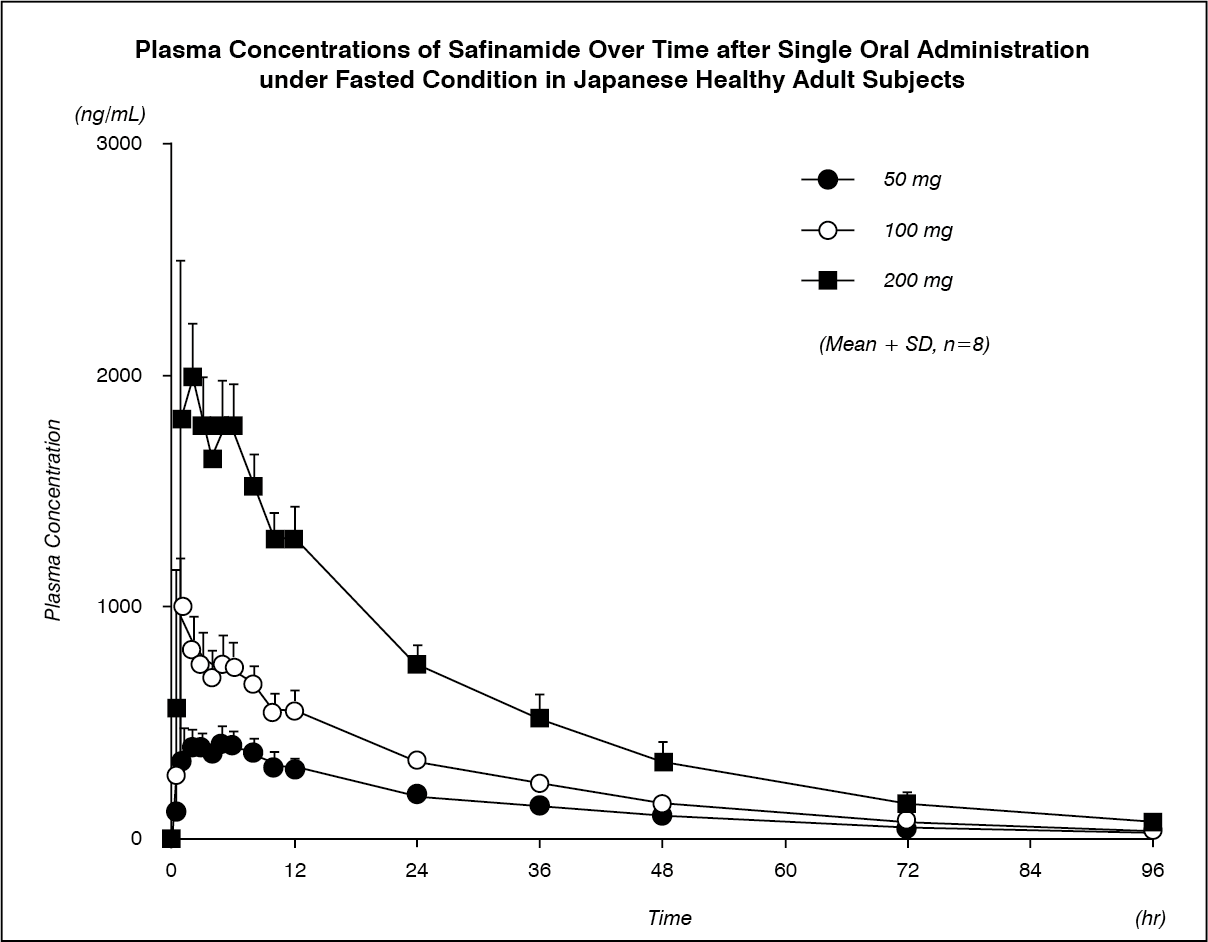 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image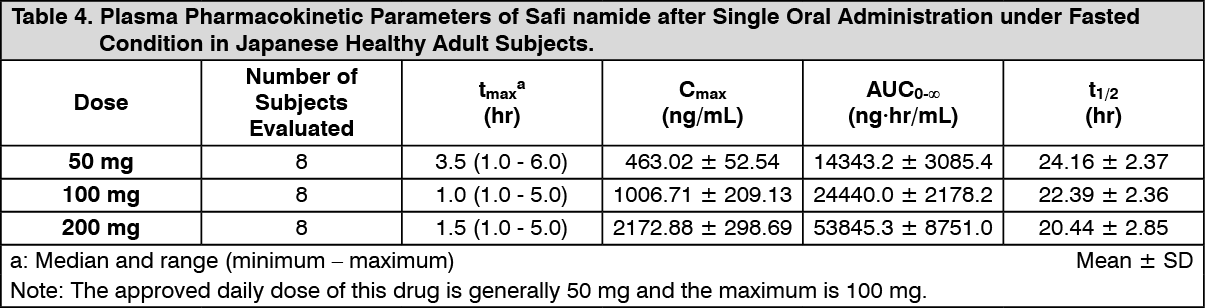 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image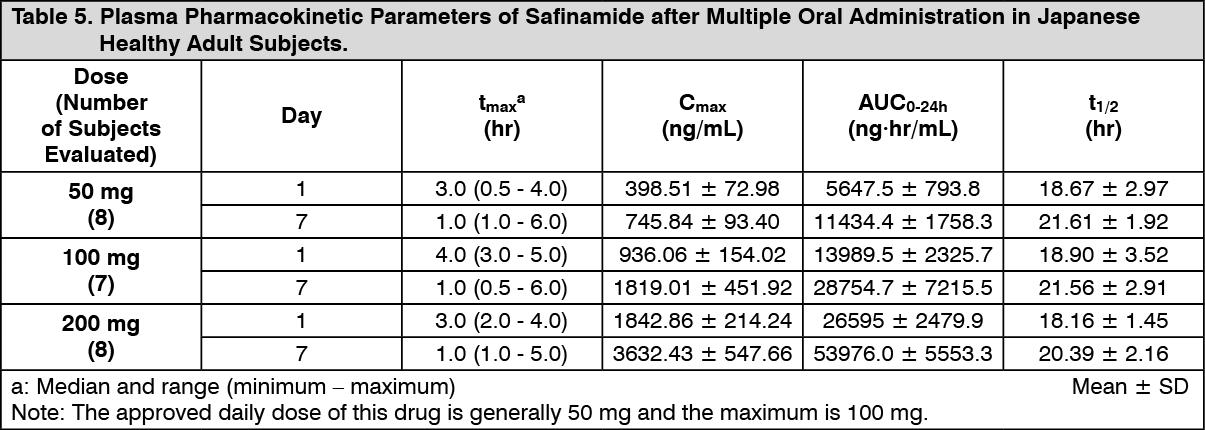 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image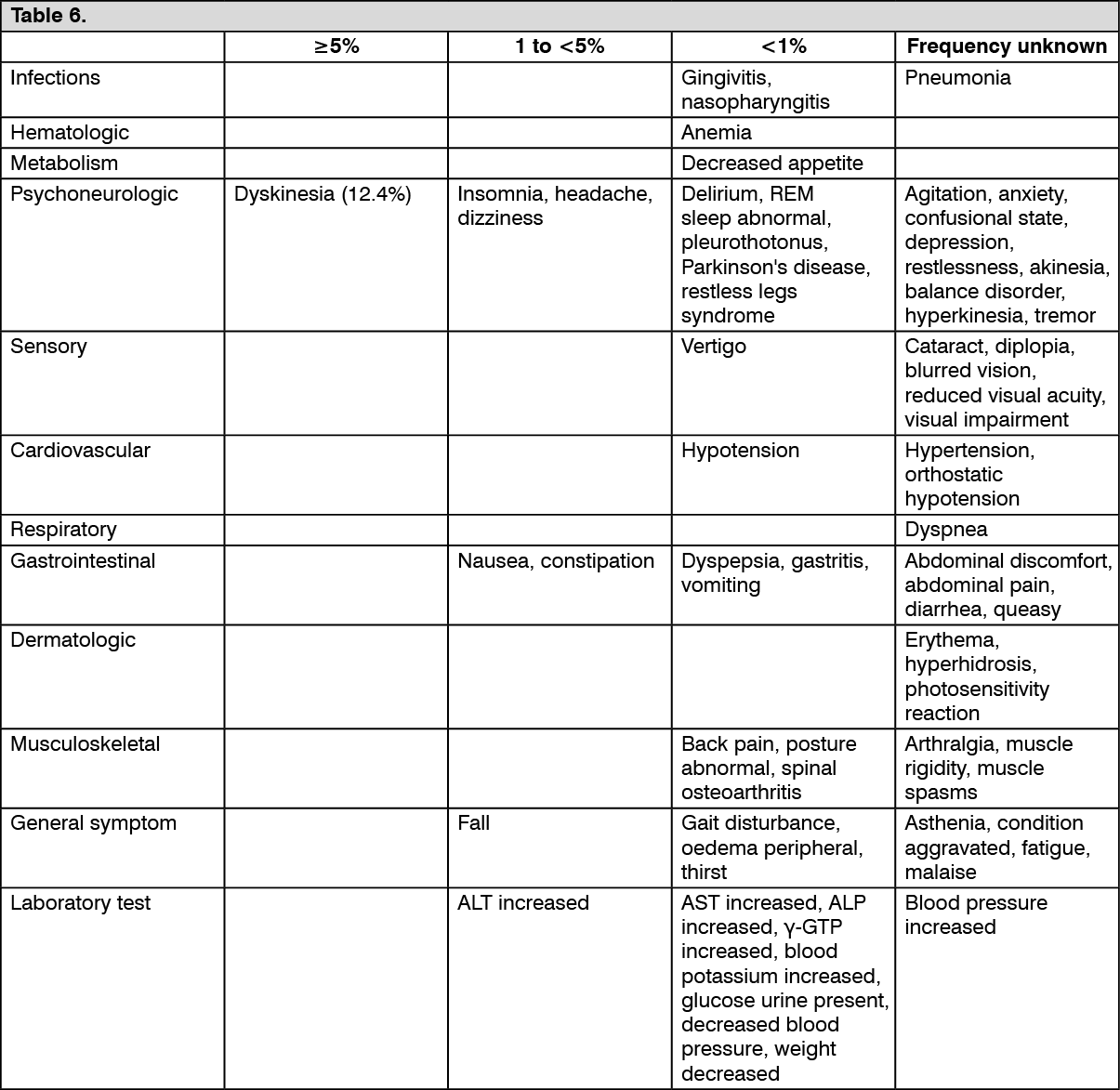 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
