The recommended dose of BiCNU in previously untreated patients is 150 to 200 mg/m
2 intravenously every 6 weeks. Administer as a single dose or divided into daily injections such as 75 to 100 mg/m
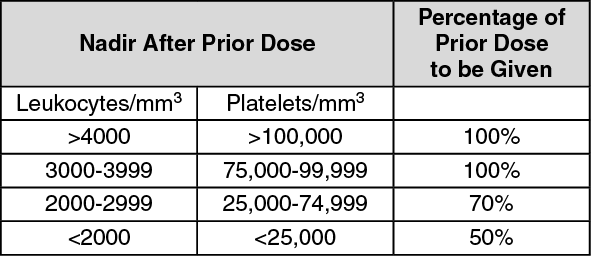
2 on two successive days. Lower the dose when BiCNU is used with other myelosuppressive drugs or in patients in whom bone marrow reserve is depleted. Administer BiCNU for the duration according to the established regimen. Premedicate each dose with anti-emetics. Adjust doses subsequent to the initial dose according to the hematologic response of the patient to the preceding dose. The following schedule is suggested as a guide to dosage adjustment: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The hematologic toxicity can be delayed and cumulative. Monitor blood counts weekly. Do not administer a repeat course of BiCNU until circulating blood elements have returned to acceptable levels (platelets above 100 Gi/L, leukocytes above 4 Gi/L and absolute neutrophil count above 1 Gi/L). The usual interval between courses is 6 weeks.
Evaluate renal function prior to administration and periodically during treatment. For patients with compromised renal function, monitor for toxicity more frequently. Discontinue BiCNU if the creatinine clearance is less than 10 mL/min. Monitor transaminases and bilirubin periodically during treatment. [See Adverse Reactions.]
Preparation and Administration of Intravenous Solution: Dissolve BiCNU with 3 mL of the supplied sterile diluent (Dehydrated Alcohol Injection, USP).
Aseptically add 27 mL Sterile Water for Injection, USP: Each mL of resulting solution contains 3.3 mg of BiCNU in 10% ethanol. Such solutions should be protected from light.
The reconstituted solution is a clear, colorless to yellowish solution.
Once reconstituted, the solution must be further diluted with Sodium Chloride Injection, US Por 5% Dextrose Injection, USP: Examine reconstituted vials for crystal formation prior to use. If crystals are observed, they may be re-dissolved by warming the vial to room temperature with agitation.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
After reconstitution as recommended, BiCNU is stable for 24 hours under refrigeration (2°-8°C, 36°-46°F) in glass container. Examine reconstituted vials for crystal formation prior to use. If crystals are observed, they may be redissolved by warming the vial to room temperature with agitation.
Vials reconstituted as directed and further diluted with 500 mL Sodium Chloride Injection, USP or 5% Dextrose Injection, USP, in glass or polypropylene containers to a concentration of 0.2 mg/mL, should be stored at room temperature, protected from light and utilized within 8 hours. These solutions are also stable 24 hours under refrigeration (2°-8°C, 36°-46°F) protected from light.
Administer reconstituted solution by slow intravenous infusion over at least two hours. Administration of BiCNU over a period of less than two hours can lead to pain and burning at the site of injection. Monitor the injected area during the administration. The rate of administration of the intravenous infusion should not be more than 1.66 mg/m
2/min.
See Storage for important instructions on the storage and handling of the injection. BiCNU is a cytotoxic drug. Follow applicable special handling and disposal procedures.
The lyophilized dosage formulation contains no preservatives and is not intended for use as a multiple dose vial.
Accidental contact of reconstituted BiCNU with the skin has caused transient hyperpigmentation of the affected areas. Wear impervious gloves to minimize the risk of dermal exposure impervious gloves when handling vials containing BiCNU. Immediately wash the skin or mucosa thoroughly with soap and water if BiCNU lyophilized material or solution contacts the skin or mucosa.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
