


 Sign Out
Sign Out

Summary of the safety profile: The safety of avelumab as monotherapy has been evaluated in 1,738 patients with solid tumours including metastatic MCC receiving 10 mg/kg every 2 weeks of avelumab in clinical studies. In this patient population, the most common adverse reactions with avelumab were fatigue (32.4%), nausea (25.1%), diarrhoea (18.9%), decreased appetite (18.4%), constipation (18.4%), infusion-related reactions (17.1%), weight decreased (16.6%), and vomiting (16.2%).
The most common Grade ≥3 adverse reactions were anaemia (6.0%), dyspnoea (3.9%), and abdominal pain (3.0%). Serious adverse reactions were immune-related adverse reactions and infusion-related reaction (see Precautions).
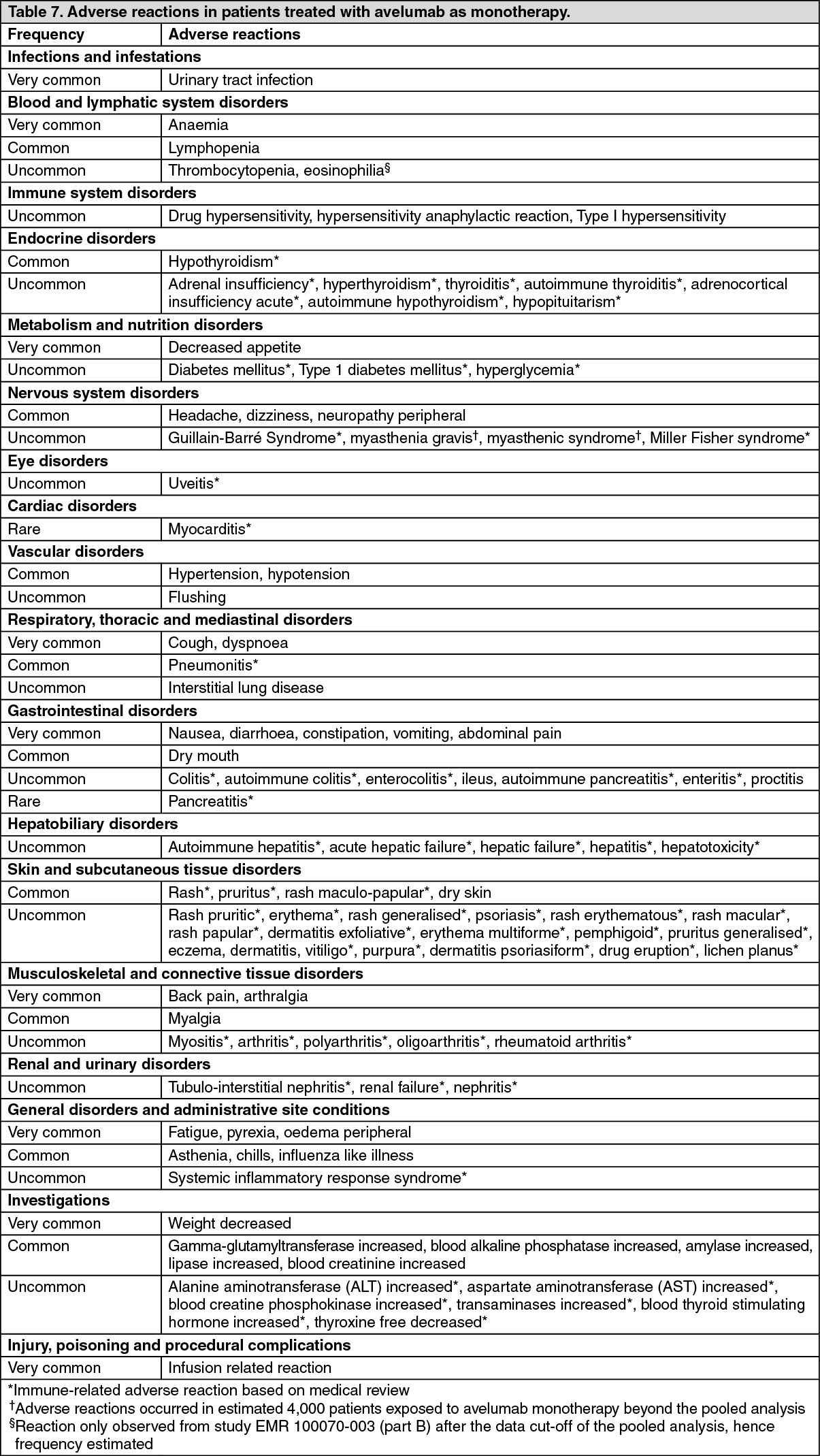
Tabulated list of adverse reactions: Adverse reactions reported for avelumab as monotherapy in patients with metastatic MCC, or locally advanced or metastatic UC are presented in Table 7. In all studies, avelumab was administered at 10 mg/kg every 2 weeks.
These reactions are presented by system organ class and frequency. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Within each frequency grouping, adverse reactions are presented in the order of decreasing seriousness. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRenal cell carcinoma: Summary of the safety profile: The safety of avelumab in combination with axitinib has been evaluated in 489 patients with advanced RCC receiving 10 mg/kg avelumab every 2 weeks and axitinib 5 mg orally twice daily in two clinical studies.
In this patient population, the most common adverse reactions were diarrhoea (62.8%), hypertension (49.3%), fatigue (42.9%), nausea (33.5%), dysphonia (32.7%), decreased appetite (26.0%), hypothyroidism (25.2%), cough (23.7%), headache (21.3%), dyspnoea (20.9%), and arthralgia (20.9%).
Tabulated list of adverse reactions: Adverse reactions reported for 489 patients with advanced RCC treated in two clinical studies with avelumab in combination with axitinib are presented in Table 8.
These reactions are presented by system organ class and frequency. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Within each frequency grouping, adverse reactions are presented in the order of decreasing seriousness. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Data for immune-related adverse reactions for avelumab as a monotherapy are based on 1,650 patients in the phase I study EMR100070-001 in solid tumours and 88 patients in study EMR100070-003, and for avelumab in combination with axitinib are based on 489 patients in study B9991002 and B9991003 who received avelumab (see Pharmacology: Pharmacodynamics under Actions).
The management guidelines for these adverse reactions are described in Precautions.
Immune-related pneumonitis: In patients treated with avelumab as monotherapy, 1.2% (21/1,738) of patients developed immune-related pneumonitis. Of these patients there was 1 (0.1%) patient with a fatal outcome, 1 (0.1%) patient with Grade 4, and 5 (0.3%) patients with Grade 3 immune-related pneumonitis.
The median time to onset of immune-related pneumonitis was 2.5 months (range: 3 days to 11 months). The median duration was 7 weeks (range: 4 days to more than 4 months).
Avelumab was discontinued in 0.3% (6/1,738) of patients due to immune-related pneumonitis. All 21 patients with immune-related pneumonitis were treated with corticosteroids and 17 (81%) of the 21 patients were treated with high-dose corticosteroids for a median of 8 days (range: 1 day to 2.3 months). Immune-related pneumonitis resolved in 12 (57%) of the 21 patients at the time of data cut-off.
In patients treated with avelumab in combination with axitinib, 0.6% (3/489) of patients developed immune-related pneumonitis. Of these patients, none experienced immune-related pneumonitis Grade ≥3.
The median time to onset of immune-related pneumonitis was 3.7 months (range: 2.7 months to 8.6 months). The median duration was 2.6 months (range: 3.3 weeks to more than 7.9 months).
Immune-related pneumonitis did not lead to discontinuation of avelumab in any patient. All 3 patients with immune-related pneumonitis were treated with high-dose corticosteroids for a median of 3.3 months (range: 3 weeks to 22.3 months). Immune-related pneumonitis resolved in 2 (66.7%) of the 3 patients at the time of data cut-off.
Immune-related hepatitis: In patients treated with avelumab as monotherapy, 0.9% (16/1,738) of patients developed immune-related hepatitis. Of these patients, there were 2 (0.1%) patients with a fatal outcome, and 11 (0.6%) patients with Grade 3 immune-related hepatitis.
The median time to onset of immune-related hepatitis was 3.2 months (range: 1 week to 15 months). The median duration was 2.5 months (range: 1 day to more than 7.4 months).
Avelumab was discontinued in 0.5% (9/1,738) of patients due to immune-related hepatitis. All 16 patients with immune-related hepatitis treated with corticosteroids and 15 (94%) of the 16 patients received high-dose corticosteroids for a median of 14 days (range: 1 day to 2.5 months). Immune-related hepatitis resolved in 9 (56%) of the 16 patients at the time of data cut-off.
In patients treated with avelumab in combination with axitinib, 6.3% (31/489) of patients developed immune related hepatitis. Of these patients, there were 18 (3.7%) patients with Grade 3 and 3 (0.6%) patients with Grade 4 immune related hepatitis.
The median time to onset of immune related hepatitis was 2.3 months (range: 2.1 weeks to 14.5 months). The median duration was 2.1 weeks (range: 2 days to 8.9 months).
Avelumab was discontinued in 4.7% (23/489) of patients due to immune-related hepatitis. All 31 patients with immune related hepatitis were treated for hepatitis including 30 (96.8%) patients treated with corticosteroids and 1 patient with a non-steroidal immunosuppressant. Twenty eight (90.3%) of the 31 patients received high dose corticosteroids for a median of 2.4 weeks (range: 1 day to 10.2 months). Immune related hepatitis resolved in 27 (87.1%) of the 31 patients at the time of data cut off.
Immune-related colitis: In patients treated with avelumab as monotherapy, 1.5% (26/1,738) of patients developed immune-related colitis. Of these patients, there were 7 (0.4%) patients with Grade 3 immune-related colitis.
The median time to onset of immune-related colitis was 2.1 months (range: 2 days to 11 months). The median duration was 6 weeks (range: 1 day to more than 14 months).
Avelumab was discontinued in 0.5% (9/1,738) of patients due to immune-related colitis. All 26 patients with immune-related colitis were treated with corticosteroids and 15 (58%) of the 26 patients received high-dose corticosteroids for a median of 19 days (range: 1 day to 2.3 months). Immune-related colitis resolved in 18 (70%) of 26 patients at the time of data cut-off.
In patients treated with avelumab in combination with axitinib, 2.7% (13/489) of patients developed immune related colitis. Of these patients, there were 9 (1.8%) patients with Grade 3 immune-related colitis.
The median time to onset of immune related colitis was 5.1 months (range: 2.3 weeks to 14 months). The median duration was 1.6 weeks (range: 1 day to more than 9 months).
Avelumab was discontinued in 0.4% (2/489) of patients due to immune-related colitis. All 13 patients with immune-related colitis were treated with corticosteroids and 12 (92.3%) of the 13 patients received high dose corticosteroids for a median of 2.3 weeks (range: 5 days to 4.6 months). Immune related colitis resolved in 10 (76.9%) of 13 patients at the time of data cut off.
Immune-related pancreatitis: In patients treated with avelumab as monotherapy, immune-related pancreatitis occurred in less than 1% (1/4,000) of patients across clinical trials in multiple tumour types and in 0.6% (3/489) of patients receiving avelumab in combination with axitinib including 2 (0.4%) patients with fatal outcome.
Immune-related myocarditis: In patients treated with avelumab as monotherapy, immune-related myocarditis occurred in less than 1% (5/4,000) of patients across clinical trials in multiple tumour types and in 0.6% (3/489) of patients receiving avelumab in combination with axitinib including 2 (0.4%) patients with fatal outcome.
Immune-related endocrinopathies: Thyroid disorders: In patients treated with avelumab as monotherapy, 6% (98/1,738) of patients developed immune-related thyroid disorders, including 90 (5%) patients with hypothyroidism, 7 (0.4%) with hyperthyroidism, and 4 (0.2%) with thyroiditis. Of these patients, there were 3 (0.2%) patients with Grade 3 immune-related thyroid disorders.
The median time to onset of thyroid disorders was 2.8 months (range: 2 weeks to 13 months). The median duration was not estimable (range: 1 day to more than 26 months).
Avelumab was discontinued in 0.1% (2/1,738) of patients due to immune-related thyroid disorders. Thyroid disorders resolved in 7 (7%) of the 98 patients at the time of data cut-off.
In patients treated with avelumab in combination with axitinib, 24.7% (121/489) of patients developed immune related thyroid disorders, including 111 (22.7%) patients with hypothyroidism, 17 (3.5%) with hyperthyroidism, and 7 (1.4%) with thyroiditis. Of these patients, there were 2 (0.4%) patients with Grade 3 immune related thyroid disorders.
The median time to onset of thyroid disorders was 2.8 months (range: 3.6 weeks to 19.3 months). The median duration was not estimable (range: 8 days to more than 23.9 months).
Avelumab was discontinued in 0.2% (1/489) of patients due to immune-related thyroid disorders. Thyroid disorders resolved in 15 (12.4%) of the 121 patients at the time of data cut off.
Adrenal insufficiency: In patients treated with avelumab as monotherapy, 0.5% (8/1,738) of patients developed immune-related adrenal insufficiency. Of these patients, there was 1 (0.1%) patient with Grade 3 immune-related adrenal insufficiency.
The median time to onset of immune-related adrenal insufficiency was 2.5 months (range: 1 day to 8 months). The median duration was not estimable (range: 2 days to more than 6 months).
Avelumab was discontinued in 0.1% (2/1,738) of patients due to immune-related adrenal insufficiency. All 8 patients with immune-related adrenal insufficiency were treated with corticosteroids, 4 (50%) of the 8 patients received high-dose systemic corticosteroids (≥40 mg prednisone or equivalent) followed by a taper for a median of 1 day (range: 1 day to 24 days). Adrenal insufficiency resolved in 1 patient with corticoid treatment at the time of data cut-off.
In patients treated with avelumab in combination with axitinib, 1.8% (9/489) of patients developed immune-related adrenal insufficiency. Of these patients, there were 2 (0.4%) patients with Grade 3 immune related adrenal insufficiency.
The median time to onset of immune related adrenal insufficiency was 5.5 months (range: 3.6 weeks to 8.7 months). The median duration was 2.8 months (range: 3 days to more than 15.5 months).
Immune-related adrenal insufficiency did not lead to discontinuation of avelumab in any patient. Eight (88.9%) patients with immune-related adrenal insufficiency were treated with corticosteroids and 2 (25%) of the 8 patients received high dose corticosteroids (≥40 mg prednisone or equivalent) for a median of 8 days (range: 5 days to 11 days). Adrenal insufficiency resolved in 4 (44.4%) of the 9 patients at the time of data cut off.
Type 1 diabetes mellitus: In patients treated with avelumab as monotherapy, Type 1 diabetes mellitus without an alternative aetiology occurred in 0.1% (2/1,738) of patients including two Grade 3 reactions that led to permanent discontinuation of avelumab.
In patients treated with avelumab in combination with axitinib, Type 1 diabetes mellitus without an alternative aetiology occurred in 1.0% (5/489) of patients. Of these patients, there was 1 (0.2%) patient with Grade 3 Type 1 diabetes mellitus.
The median time to onset of Type 1 diabetes mellitus was 1.9 months (range: 1.1 months to 7.3 months).
Avelumab was discontinued in 0.2% (1/489) of patients due to Type 1 diabetes mellitus. All 5 patients with Type 1 diabetes mellitus were treated with insulin. Type 1 diabetes mellitus did not resolve in any of the patients at the time of data cut off.
Immune-related nephritis and renal dysfunction: In patients treated with avelumab as monotherapy, immune-related nephritis occurred in 0.1% (1/1,738) of patients receiving avelumab leading to permanent discontinuation of avelumab.
In patients treated with avelumab in combination with axitinib, immune-related nephritis occurred in 0.4% (2/489) of patients. Of these patients, there were 2 (0.4%) patients with Grade 3 immune-related nephritis.
The median time to onset of immune-related nephritis was 1.2 months (range: 2.9 weeks to 1.8 months). The median duration was 1.3 weeks (range: more than 4 days to 1.3 weeks).
Immune-related nephritis did not lead to discontinuation of avelumab in any patient. All 2 patients with immune-related nephritis were treated with high dose corticosteroids for a median of 1.1 weeks (range: 3 days to 1.9 weeks). Immune-related nephritis resolved in 1 (50%) of the 2 patients at the time of data cut off.
Hepatotoxicity (in combination with axitinib): In patients treated with avelumab in combination with axitinib, Grades 3 and Grade 4 increased ALT and increased AST were reported in 9% and 7% of patients, respectively.
In patients with ALT ≥3 times ULN (Grades 2-4, n=82), ALT resolved to Grades 0-1 in 92%.
Among the 73 patients who were rechallenged with either avelumab (59%) or axitinib (85%) monotherapy or with both (55%), 66% had no recurrence of ALT ≥3 times ULN.
Immunogenicity: Of 1,738 patients treated with avelumab 10 mg/kg as an intravenous infusion every 2 weeks, 1,627 were evaluable for treatment-emergent anti-drug antibodies (ADA) and 96 (5.9%) tested positive. In ADA positive patients, there may be an increased risk for infusion-related reactions (about 40% and 25% in ADA ever-positive and ADA never-positive patients, respectively). A new ADA method with improved sensitivity and drug tolerance for evaluating treatment-emergent ADA in patients treated with avelumab as monotherapy was used for study B9991001. Of the 344 patients treated with avelumab 10 mg/kg as an intravenous infusion every 2 weeks plus BSC, 325 were evaluable for treatment-emergent ADA and 62 (19.1%) tested positive. Based on data available, including the low incidence of immunogenicity, the impact of ADA on pharmacokinetics, efficacy and safety is uncertain, the impact of neutralizing antibodies (nAb) is unknown.
Of the 480 patients with at least one valid ADA result at any time point treated with avelumab 10 mg/kg as an intravenous infusion every 2 weeks in combination with axitinib 5 mg twice daily, 453 were evaluable for treatment-emergent ADA and 66 (14.6%) tested positive. The new ADA method with improved sensitivity was used in the RCC population. Overall, there was no evidence of altered pharmacokinetic profile, increased incidence of infusion reactions or effects on efficacy with anti-avelumab antibody development.
View ADR Monitoring Form