Therapeutic Classification: Corticosteroid for nasal use.
Pharmacology: Mode of action: Mometasone furoate is a topical glucocorticosteroid with local anti-inflammatory properties at doses that are not systemically active.
Clinical Pharmacology: Mometasone furoate, administered as a nasal spray, has a systemic bioavailability of <1% in plasma, using a sensitive assay with a lower quantitation limit (LLOQ) of 0.25 pg/ml. Mometasone furoate suspension is very poorly absorbed from the gastrointestinal tract, and the small amount that may be swallowed and absorbed undergoes extensive first-pass metabolism prior to excretion in urine and bile.
In studies utilizing nasal antigen challenge, Mometasone Aqueous Nasal Spray has shown anti-inflammatory activity in both the early- and late-phase allergic responses. This has been demonstrated by decreases (vs. placebo) in histamine and eosinophils, neutrophils, and epithelial cell adhesion proteins.
Three studies were conducted to assess the safety and efficacy of Mometasone Aqueous Nasal Spray in the treatment of nasal polyps for four month. These included two pivotal trials evaluating doses of 200 mcg once or twice daily and a supportive trial evaluating a dose of 200 mcg once daily. A total of 594 adult patients (ages 18 to 86 years) received Mometasone Aqueous Nasal Spray. The co-primary efficacy endpoints in the pivotal trials were: change from baseline in nasal congestion/obstruction averaged over the first month of treatment; and change from baseline to last assessment in bilateral polyp grade during the entire 4 months of treatment as assessed by nasal endoscopy. Efficacy was demonstrated in both studies at a dose of 200 mcg twice daily and in one study at a dose of 200 mcg once a day. Improvement in other symptoms of nasal polyps (loss of smell, rhinorrhea and postnasal drip) was also observed after a 1-month treatment with 200 mcg, twice daily dose compared to placebo in both studies and in one study after once daily treatment. In the supportive study, patients demonstrated a statistically significant improvement with Mometasone Aqueous nasal spray at a dose of 200 mcg once a day in relief of nasal congestion and reduction of polyp size with 4 months of treatment compared to placebo.
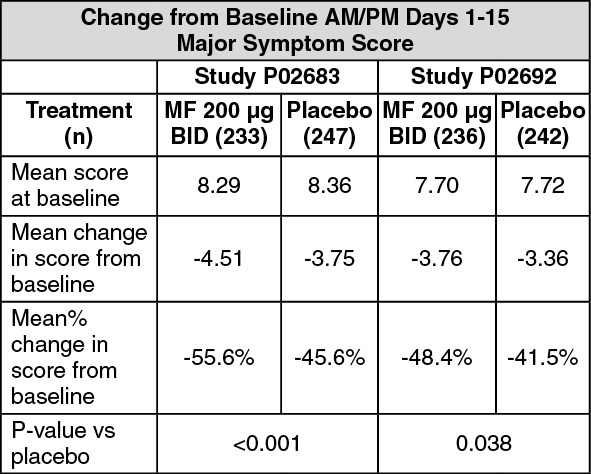
In two trials with 1954 patients 12 years of age and older with signs and symptoms of acute rhinosinusitis for 7 to 28 days prior to baseline, Mometasone Aqueous Nasal Spray 200 μg twice daily was effective in significantly improving symptoms of rhinosinusitis compared to placebo as evaluated by the Major Symptom Score (MSS) composite of symptoms (facial pain/pressure/tenderness, sinus headache, rhinorrhea, post nasal drip, and nasal congestion/stuffiness) during the 15 day treatment period (P02683 p < 0.001; P02692 p = 0.038). In P02683, Mometasone Aqueous Nasal Spray 200 μg twice daily reduced the MSS score (averaged across the 15 day treatment period) by 55.6% from baseline, whereas placebo treatment reduced the MSS by 45.6%. In P02692, Mometasone Aqueous Nasal Spray 200 μg twice daily reduced the MSS score by 48.4% from baseline, whereas placebo treatment reduced the MSS by 41.5% (see Table).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients were eligible for study entry only if all signs and symptoms suggestive of bacterial rhinosinusitis were absent. These signs and symptoms were: fever >38.3°C; persistent severe unilateral facial pain or tooth pain; orbital or periorbital facial swelling; dental involvement; and worsening of symptoms after initial improvement. In addition, patients with severe symptoms (on a scale of mild, moderate or severe) in more than three of the five MSS symptom groups were not eligible for study participation. Thus, study subjects generally had mild or moderate rhinosinusitis, likely of non-bacterial origin. Consistent with this, a 500 mg three times a day amoxicillin arm was not significantly different from placebo in reducing the symptoms of rhinosinusitis as evaluated by the MSS. Overall, fewer subjects treated with Mometasone Aqueous Nasal Spray 200 μg twice daily were considered by the treating physician to be treatment failures than those with placebo (p=0.0074). In addition, during the post-treatment follow-up period, the number of recurrences seen with Mometasone was low and comparable to the amoxicillin and placebo treatment groups. Treatment duration beyond 15 days was not evaluated in acute rhinosinusitis.
Toxicology: Preclinical Pharmacology and Toxicology: Preclinical studies demonstrate that mometasone furoate is devoid of androgenic, antiandrogenic, estrogenic or antiestrogenic activity but, like other glucocorticoids, it possesses some antiuterotrophic activity and delays vaginal opening in animal models at high oral doses of 56 mg/kg/day and 280 mg/kg/day.
In cell culture, mometasone furoate was shown to be at least ten times more potent than other steroids, including beclomethasone dipropionate (BDP), betamethasone, hydrocortisone and dexamethasone, at inhibiting the synthesis/release of IL-1, IL-6 and TNFα. Mometasone furoate (IC
50 = 0.12 Nm) was also at least six times more potent than BDP and betamethasone at inhibiting IL-5 production. Also, in mixed leukocytes from atopic patients, mometasone was a more potent leukotriene production inhibitor than BDP.
In a preclinical model, the compound has been shown to reduce the accumulation of eosinophils markedly at the site of an allergic reaction. For example, in allergic mice with IgE-mediated allergy, inhaled mometasone furoate at doses as low as 10 micrograms/kg inhibited eosinophil infiltration into bronchoalveolar lavage fluid and the lung bronchi and bronchioles. Additionally, mometasone furoate reduced the number of lymphocytes, and the levels of messenger RNA for the proallergic cytokines IL-4 and IL-5.
It is likely that much of the mechanism for the antiallergic and anti-inflammatory effects of mometasone furoate lies in its ability to inhibit the release of mediators of allergic reactions. Mometasone furoate significantly inhibits the release of leukotrienes from leukocytes of allergic patients. In addition, it is an extremely potent inhibitor of the production of the Th
2 cytokines, IL-4 and IL-5 from human CD4
+ T-cells.
Mometasone furoate was nonmutagenic in the mouse-lymphoma assay and the salmonella/mammalian-microsome bioassay. Mometasone furoate was negative in the mouse bone-marrow erythrocyte-micronucleus assay, the rat bone-marrow clastogenicity assay, the mouse mitotic male germ-cell clastogenicity assay, and the Chinese hamster lung-cell chromosomal-aberrations assay. At cytotoxic doses in Chinese hamster ovary cell cultures, mometasone furoate induced a dose-related increase in simple chromosome aberrations when continuously exposed (7.5 hours) in the nonactivation phase, but not in the presence of rat liver S9 fraction. This finding is not considered to be of significance in the risk assessment of mometasone furoate, since the S9 phase of the chromosomal-aberration assay and all
in vivo assays were negative. Clastogenic responses without human health risk implications have been observed at cytotoxic doses with other corticosteroids, such as dexamethasone.
In subcutaneous Segment I and III studies, mometasone furoate was well tolerated at doses up to 7.5 micrograms/kg (2.6 times the human dose by inhalation). At 15 micrograms/kg prolonged gestation and prolonged and difficult labor occurred with a reduction in offspring survival and body weight or body weight gain. There was no effect on fertility.
Like other glucocorticoids, mometasone furoate is a teratogen in rodents and rabbits. Teratology studies were conducted in rats, mice and rabbits by the topical (dermal) and/or subcutaneous routes. Umbilical hernia occurred in rats administered ≥600 micrograms/kg dermally, cleft palate in mice administered 180 micrograms/kg subcutaneously, and gall-bladder agenesis, umbilical hernia, and flexed front paws in rabbits administered ≥150 micrograms/kg dermally. In these teratogenicity studies, there were also reductions in maternal body weight gains, effects on fetal growth (lower fetal body weight and/or delayed ossification) in rats, rabbits and mice, and reduced offspring survival in mice.
No toxicologic effects unique to mometasone furoate exposure were demonstrated. All observed effects are typical of this class of compounds and are related to exaggerated pharmacologic effects of glucocorticoids.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
