


 Sign Out
Sign Out


The empirical formula of Atorvastatin calcium is (C33H34FN2O5)2Ca∙3H2O) and its molecular weight is 1209.42.
Atorvastatin calcium is a white to off-white crystalline powder, practically insoluble in aqueous solutions of pH 4 and below. It is very slightly soluble in distilled water, pH 7.4 phosphate buffer, and acetonitrile, slightly soluble in ethanol and freely soluble in methanol.
Mechanism of Action: Atorvastatin is a selective, competitive inhibitor of HMG-CoA reductase, the rate-limiting enzyme that converts 3-hydroxy-3-methylglutaryl-coenzyme A to mevalonate, a precursor of sterols, including cholesterol. In patients with homozygous and heterozygous familial hypercholesterolemia (FH), non-familial forms of hypercholesterolemia, and mixed dyslipidemia, Atorvastatin reduces total-C (total cholesterol), LDL-C (low-density lipoprotein cholesterol), and apo B (apolipoprotein B). Atorvastatin also reduces VLDL-C (very-low-density lipoprotein cholesterol) and TG (triglycerides) and produces variable increases in HDL-C (high-density lipoprotein cholesterol).
Triglycerides and cholesterol in the liver are incorporated into VLDL and released into the plasma for delivery to peripheral tissues. LDL is formed from VLDL and is catabolized primarily through the high-affinity LDL receptor. Like LDL, cholesterol-enriched triglyceride-rich lipoproteins, including VLDL, IDL, and remnants can also promote atherosclerosis. Elevated plasma triglycerides are frequently found in a triad with low HDL-C levels and small LDL particles, as well as in association with non-lipid metabolic risk factors for coronary heart disease. As such, total plasma TG has not consistently been shown to be an independent risk factor for CHD. Furthermore, the independent effect of raising HDL or lowering TG on the risk of coronary and cardiovascular morbidity and mortality has not been determined.
Atorvastatin lowers plasma cholesterol and lipoprotein levels by inhibiting HMG-CoA reductase and cholesterol synthesis in the liver and by increasing the number of hepatic LDL receptors on the cell surface for enhanced uptake and catabolism of LDL.
Atorvastatin reduces LDL production and the number of LDL particles. Atorvastatin produces a profound and sustained increase in LDL receptor activity coupled with a beneficial change in the quality of circulating LDL particles. Atorvastatin is effective in reducing LDL in patients with homozygous familial hypercholesterolemia, a population that has not normally responded to lipid-lowering medication.
In a dose-response study, Atorvastatin (10-80 mg) reduced total-C (30%-46%), LDL-C (41%-61%), apo B (34%-50%), and TG (14%-33%). These results are consistent in patients with heterozygous familial hypercholesterolemia, non-familial forms of hypercholesterolemia, and mixed hyperlipidemia, including patients with non-insulin-dependent diabetes mellitus.
In patients with isolated hypertriglyceridemia, Atorvastatin reduces total-C, LDL-C, VLDL-C, apo B, TG, and non-HDL-C, and increases HDL-C. In patients with dysbetalipoproteinemia, Atorvastatin reduces IDL-C (intermediate density lipoprotein cholesterol).
In patients with Fredrickson Types IIa and IIb hyperlipoproteinemia pooled from 24 controlled trials, the median percent increases from baseline in HDL-C for Atorvastatin (10-80 mg) were 5.1-8.7% in a non-dose-related manner. Additionally, analysis of this pooled data demonstrated significant dose related decreases in total-C/HDL-C and LDL-C/HDL-C ratios, ranging from -29 to -44% and -37 to -55%, respectively.
Atorvastatin and some of its metabolites are pharmacologically active in humans. The primary site of action of Atorvastatin is the liver, which is the principal site of cholesterol synthesis and LDL clearance. LDL-C reduction correlates better with drug dose than it does with systemic drug concentration. Individualization of drug dosage should be based on therapeutic response (see Dosage & Administration).
Prevention of Cardiovascular Complications: In the Anglo-Scandinavian Cardiac Outcomes Trial Lipid Lowering Arm (ASCOT-LLA), the effect of Atorvastatin on fatal and non-fatal coronary heart disease was assessed in 10,305 hypertensive patients 40-80 years of age (mean of 63 years), without a previous myocardial infarction (MI) and with total cholesterol (TC) levels ≤6.5 mmol/l (251 mg/dl). Additionally all patients had at least 3 of the following cardiovascular risk factors: male gender (81.1%), age ≥55 years (84.5%), smoking (33.2%), diabetes (24.3%), history of CHD in a first-degree relative (26%), TC:HDL ≥6 (14.3%), peripheral vascular disease (5.1%), left ventricular hypertrophy (14.4%), prior cerebrovascular event (9.8%), specific ECG abnormalities (14.3%), proteinuria/albuminuria (62.4%). In this double-blind, placebo-controlled study patients were treated with anti-hypertensive therapy (Goal BP <140/90 mm Hg for non-diabetic patients, <130/80 mm Hg for diabetic patients) and allocated to either Atorvastatin 10 mg daily (n=5168) or placebo (n=5137). Patients were followed for a median duration of 3.3 years. Blood pressure control throughout the trial was similar in patients assigned to Atorvastatin and placebo. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe primary endpoint examined in ASCOT was the rate of fatal coronary heart disease or non-fatal (symptomatic and silent) myocardial infarction. These coronary events occurred in 1.9% of Atorvastatin treated patients compared to 3% of placebo treated subjects, a relative risk reduction of 36% (p=0.0005). There was no significant difference between groups for cardiovascular mortality (p=0.51) and all-cause mortality (p=0.17).
In the Collaborative Atorvastatin Diabetes Study (CARDS), the effect of Atorvastatin on fatal and non-fatal cardiovascular disease was assessed in 2838 patients with type 2 diabetes 40-75 years of age, without prior history of cardiovascular disease and with LDL ≤4.14 mmol/l (160 mg/dl) and TG ≤6.78 mmol/l (600 mg/dl). Additionally, all patients had at least 1 of the following risk factors: hypertension, current smoking, retinopathy, microalbuminuria or macroalbuminuria.
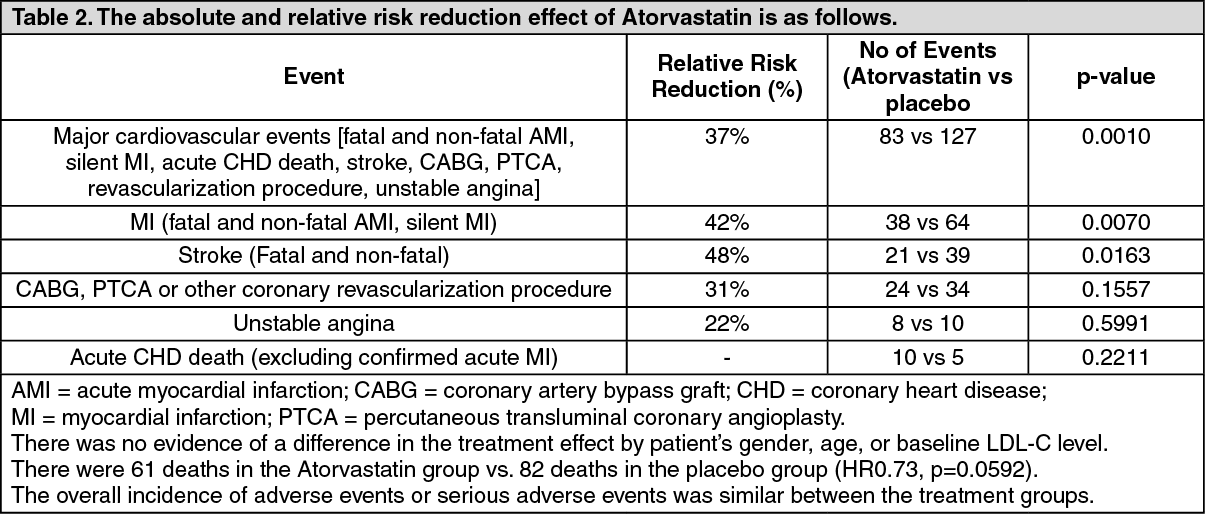
In this randomized, double-blind, multicenter, placebo-controlled trial, patients were treated with either Atorvastatin 10 mg daily (n=1428) or placebo (n=1410) for a median follow-up of 3.9 years. As the effect of Atorvastatin treatment on the primary endpoint reached the predefined stopping rules for efficacy, CARDS was terminated 2 years earlier than anticipated.
The absolute and relative risk reduction effect of Atorvastatin is as follows: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSecondary Prevention of Cardiovascular Events: In the Treating to New Targets Study (TNT), the effect of Atorvastatin 80 mg/day vs. Atorvastatin 10 mg/day on the reduction in cardiovascular events was assessed in 10,001 subjects (94% white, 81% male, 38% ≥65 years) with clinically evident coronary heart disease who had achieved a target LDL-C level <130 mg/dL after completing an 8-week, open-label, run-in period with Atorvastatin 10 mg/day. Subjects were randomly assigned to either 10 mg/day or 80 mg/day of Atorvastatin and followed for a median duration of 4.9 years. The primary endpoint was the time-to-first occurrence of any of the following major cardiovascular events (MCVE): death due to CHD, non-fatal myocardial infarction, resuscitated cardiac arrest, and fatal and non-fatal stroke. The mean LDL-C, TC, TG, non-HDL and HDL cholesterol levels at 12 weeks were 73, 145, 128, 98 and 47 mg/dL during treatment with 80 mg of Atorvastatin and 99, 177, 152, 129 and 48 mg/dL during treatment with 10 mg of Atorvastatin.
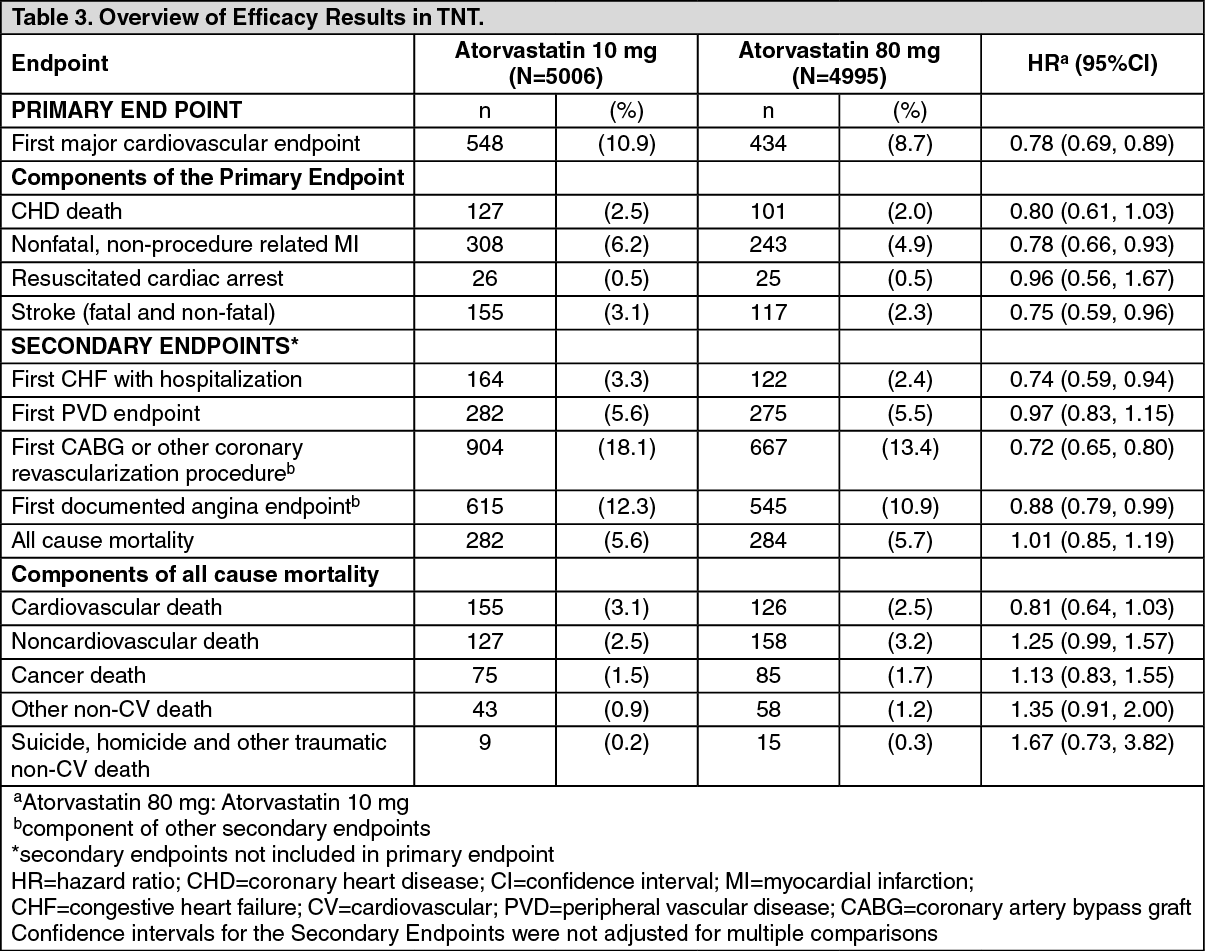
Treatment with Atorvastatin 80 mg/day significantly reduced the rate of major cardiovascular events (MCVE) (434 events in the 80 mg/day group vs 548 events in the 10 mg/day group) with a relative risk reduction of 22%. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThere was no significant difference between the treatment groups for all-cause mortality: 282 (5.6%) in the Atorvastatin 10 mg/day group vs. 284 (5.7%) in the Atorvastatin 80 mg/day group. The proportions of subjects who experienced cardiovascular death, including the components of CHD death and fatal stroke were numerically smaller in the Atorvastatin 80 mg group than in the Atorvastatin 10 mg treatment group. The proportions of subjects who experienced non-cardiovascular death were numerically larger in the Atorvastatin 80 mg group than in the Atorvastatin 10 mg treatment group.
In the Incremental Decrease in Endpoints Through Aggressive Lipid Lowering Study (IDEAL), treatment with Atorvastatin 80 mg/day was compared to treatment with simvastatin 20-40 mg/day in 8,888 subjects up to 80 years of age with a history of CHD to assess whether reduction in CV risk could be achieved. Patients were mainly male (81%), white (99%) with an average age of 61.7 years, and an average LDL-C of 121.5 mg/dL at randomization; 76% were on statin therapy. In this prospective, randomized, open-label, blinded endpoint (PROBE) trial with no run-in period, subjects were followed for a median duration of 4.8 years. The mean LDL-C, TC, TG, HDL and non-HDL cholesterol levels at Week 12 were 78, 145, 115, 45 and 100 mg/dL during treatment with 80 mg of Atorvastatin and 105, 179, 142, 47 and 132 mg/dL during treatment with 20-40 mg of simvastatin.
There was no significant difference between the treatment groups for the primary endpoint, the rate of first major coronary event (fatal CHD, non-fatal MI and resuscitated cardiac arrest): 411 (9.3%) in the Atorvastatin 80 mg/day group vs. 463 (10.4%) in the simvastatin 20-40 mg/day group, HR 0.89, 95% CI (0.78, 1.01), p=0.07.
There were no significant differences between the treatment groups for all-cause mortality: 366 (8.2%) in the Atorvastatin 80 mg/day group vs. 374 (8.4%) in the simvastatin 20-40 mg/day group. The proportions of subjects who experienced CV or non-CV death were similar for the Atorvastatin 80 mg group and the simvastatin 20-40 mg group.
There were more serious adverse events and discontinuations due to adverse events in the high-dose Atorvastatin group (92, 1.8%; 497, 9.9%, respectively) as compared to the low-dose group (69, 1.4%; 404, 8.1%, respectively). Persistent transaminase elevations (≥3x ULN twice within 4-10 days) occurred in 62 (1.3%) individuals with Atorvastatin 80 mg and in nine (0.2%) individuals with Atorvastatin 10 mg. Elevations of CK (≥10 x ULN) were low overall, but were higher in the high-dose Atorvastatin treatment group (13, 0.3%) compared to the low-dose Atorvastatin group (6, 0.1%).
Paediatric Population: Heterozygous Familial Hypercholesterolaemia in Paediatric Patients aged 6-17 years old: An 8-week, open-label study to evaluate pharmacokinetics, pharmacodynamics, and safety and tolerability of Atorvastatin was conducted in children and adolescents with genetically confirmed heterozygous familial hypercholesterolemia and baseline LDL-C ≥4 mmol/L. A total of 39 children and adolescents, 6 to 17 years of age, were enrolled. Cohort A included 15 children, 6 to 12 years of age and at Tanner Stage 1. Cohort B included 24 children, 10 to 17 years of age and at Tanner Stage ≥2.
The initial dose of Atorvastatin was 5 mg daily of a chewable tablet in Cohort A and 10 mg daily of a tablet formulation in Cohort B. The atorvastatin dose was permitted to be doubled if a subject had not attained target LDL-C of <3.35 mmol/L at Week 4 and if Atorvastatin was well tolerated.
Mean values for LDL-C, TC, VLDL-C, and Apo B decreased by Week 2 among all subjects. For subjects whose dose was doubled, additional decreases were observed as early as 2 weeks, at the first assessment, after dose escalation. The mean percent decreases in lipid parameters were similar for both cohorts, regardless of whether subjects remained at their initial dose or doubled their initial dose. At Week 8, on average, the percent change from baseline in LDL-C and TC was approximately 40% and 30%, respectively, over the range of exposures.
Heterozygous Familial Hypercholesterolaemia in Paediatric Patients aged 10-17 years old: In a double-blind, placebo controlled study followed by an open-label phase, 187 boys and post-menarchal girls 10-17 years of age (mean age 14.1 years) with heterozygous familial hypercholesterolaemia (FH) or severe hypercholesterolaemia were randomised to Atorvastatin (n=140) or placebo (n=47) for 26 weeks and then all received Atorvastatin for 26 weeks. The dosage of Atorvastatin (once daily) was 10 mg for the first 4 weeks and up-titrated to 20 mg if the LDL-C level was >3.36 mmol/l. Atorvastatin significantly decreased plasma levels of total-C, LDL-C, triglycerides, and apolipoprotein B during the 26-week double-blind phase. The mean achieved LDLC value was 3.38 mmol/l (range: 1.81-6.26 mmol/l) in the Atorvastatin group compared to 5.91 mmol/l (range: 3.93-9.96 mmol/l) in the placebo group during the 26-week double-blind phase.
An additional paediatric study of Atorvastatin versus colestipol in patients with hypercholesterolaemia aged 10-18 years demonstrated that Atorvastatin (N=25) caused a significant reduction in LDL-C at week 26 (p<0.05) compared with colestipol (N=31).
A compassionate use study in patients with severe hypercholesterolaemia (including homozygous hypercholesterolaemia) included 46 paediatric patients treated with atorvastatin titrated according to response (some subjects received 80 mg atorvastatin per day). The study lasted 3 years: LDLcholesterol was lowered by 36%.
The long-term efficacy of Atorvastatin therapy in childhood to reduce morbidity and mortality in adulthood has not been established.
Pharmacokinetics: Absorption: Atorvastatin is rapidly absorbed after oral administration; maximum plasma concentrations occur within one to two hours. Extent of absorption and plasma Atorvastatin concentrations increase in proportion to Atorvastatin dose. Atorvastatin tablets are 95% to 99% bioavailable compared with solutions. The absolute bioavailability of Atorvastatin is approximately 14% and the systemic availability of HMG-CoA reductase inhibitory activity is approximately 30%. The low systemic availability is attributed to presystemic clearance in gastrointestinal mucosa and/or hepatic first-pass metabolism. Although food decreases the rate and extent of drug absorption by approximately 25% and 9% respectively, as assessed by Cmax and AUC, LDL-C reduction is similar whether Atorvastatin is given with or without food. Plasma Atorvastatin concentrations are lower (approximately 30% for Cmax and AUC) following evening drug administration compared with morning. However, LDL-C reduction is the same regardless of the time of day of drug administration (see Dosage & Administration).
Distribution: Mean volume of distribution of Atorvastatin is approximately 381 liters. Atorvastatin is ≥98% bound to plasma proteins. A red blood cell/plasma ratio of approximately 0.25 indicates poor drug penetration into red blood cells.
Metabolism: Atorvastatin is extensively metabolized to ortho- and parahydroxylated derivatives and various beta-oxidation products. In vitro inhibition of HMG-CoA reductase by ortho- and parahydroxylated metabolites is equivalent to that of Atorvastatin. Approximately 70% of circulating inhibitory activity for HMG-CoA reductase is attributed to active metabolites. In vitro studies suggest the importance of Atorvastatin metabolism by hepatic cytochrome P450 3A4, consistent with increased plasma concentrations of Atorvastatin in humans following coadministration with erythromycin, a known inhibitor of this isozyme. In vitro studies also indicate that Atorvastatin is a weak inhibitor of cytochrome P450 3A4. Atorvastatin coadministration did not produce a clinically significant effect in plasma concentrations of terfenadine, a compound predominantly metabolized by cytochrome P450 3A4; therefore, it is unlikely that Atorvastatin will significantly alter the pharmacokinetics of other cytochrome P450 3A4 substrates (see Interactions). In animals, the ortho-hydroxy metabolite undergoes further glucuronidation.
Excretion: Atorvastatin and its metabolites are eliminated primarily in bile following hepatic and/or extrahepatic metabolism; however, the drug does not appear to undergo enterohepatic recirculation. Mean plasma elimination half-life of Atorvastatin in humans is approximately 14 hours, but the half-life of inhibitory activity for HMG-CoA reductase is 20 to 30 hours due to the contribution of active metabolites. Less than 2% of a dose of Atorvastatin is recovered in urine following oral administration.
Special Populations: Elderly: Plasma concentrations of Atorvastatin are higher (approximately 40% for Cmax and 30% for AUC) in healthy, elderly subjects (aged ≥65 years) than in young adults. The ACCESS study specifically evaluated elderly patients with respect to reaching their NCEP treatment goals. The study included 1087 patients under 65 years of age, 815 patients over 65 years of age, and 185 patients over 75 years of age. No differences in safety, efficacy or lipid treatment goal attainment were observed between elderly patients and the overall population.
Paediatric: In an open-label, 8-week study, Tanner Stage 1 (N=15) and Tanner Stage ≥2 (N=24) paediatric patients (ages 6-17 years) with heterozygous familial hypercholesterolemia and baseline LDL-C ≥4 mmol/L were treated with 5 or 10 mg of chewable or 10 or 20 mg of film-coated atorvastatin tablets once daily, respectively. Body weight was the only significant covariate in atorvastatin population PK model. Apparent oral clearance of atorvastatin in paediatric subjects appeared similar to adults when scaled allometrically by body weight. Consistent decreases in LDL-C and TC were observed over the range of atorvastatin and o-hydroxyatorvastatin exposures.
Gender: Plasma concentrations of Atorvastatin in women differ (approximately 20% higher for Cmax and 10% lower for AUC) from those in men. However, there were no clinically significant differences in lipid effects between men and women.
Renal Insufficiency: Renal disease has no influence on the plasma concentrations or lipid effects of Atorvastatin. Thus, dose adjustment in patients with renal dysfunction is not necessary (see Dosage & Administration).
Hemodialysis: While studies have not been conducted in patients with end-stage renal disease, hemodialysis is not expected to significantly enhance clearance of Atorvastatin since the drug is extensively bound to plasma proteins.
Hepatic Insufficiency: Plasma concentrations of Atorvastatin are markedly increased (approximately 16-fold in Cmax and 11-fold in AUC) in patients with chronic alcoholic liver disease (Childs-Pugh B) (see Contraindications).
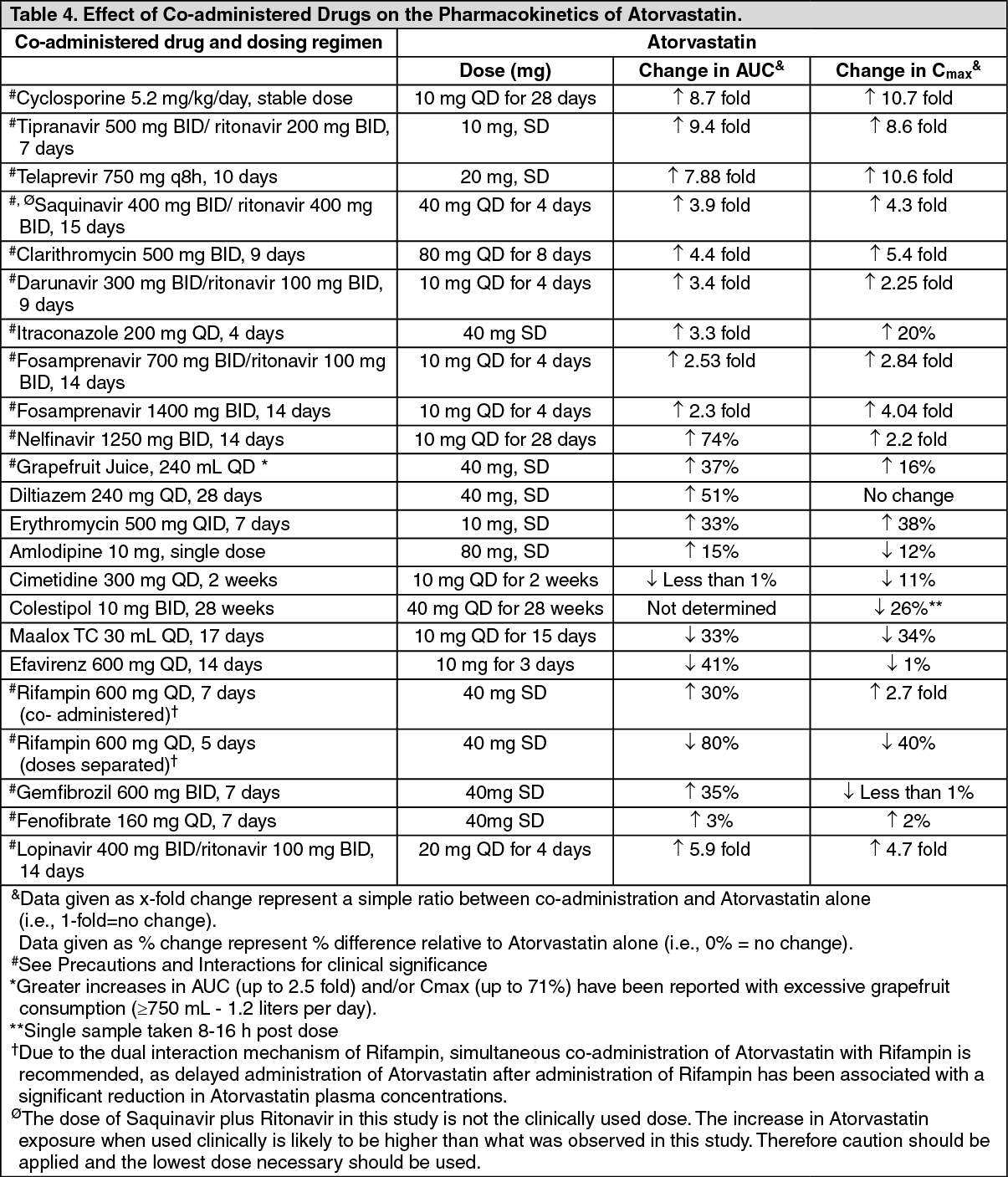
Drug Interactions: The effect of co-administered drugs on the pharmacokinetics of Atorvastatin as well as the effect of Atorvastatin on the pharmacokinetics of co-administered drugs are summarized as follows (see Precautions and Interactions). See Table 4 and Table 5.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image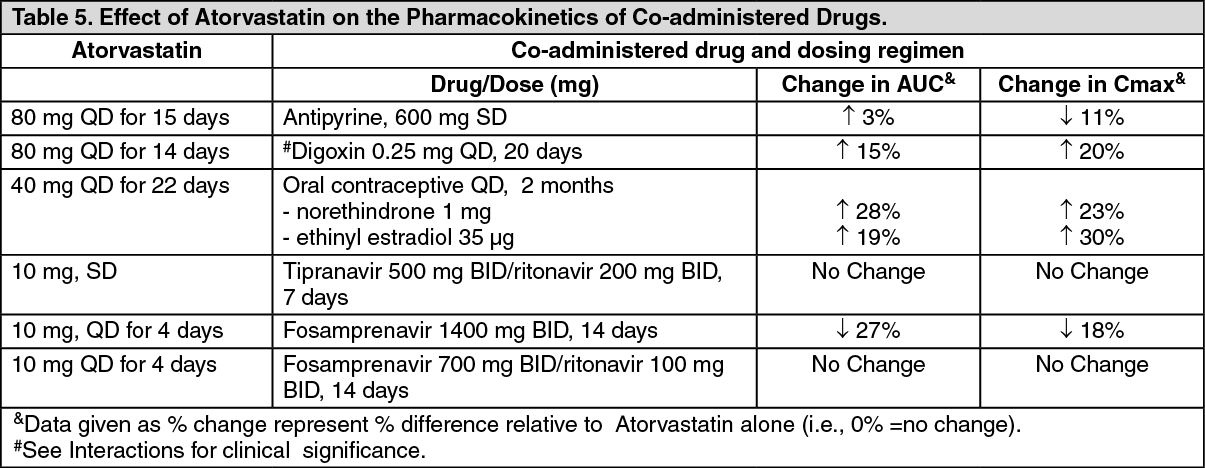 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageToxicology: Preclinical safety data: Carcinogenesis, Mutagenesis, Impairment of Fertility: Atorvastatin was not carcinogenic in rats. The maximum dose used was 63-fold higher than the highest human dose (80 mg/day) on a mg/kg body-weight basis and 8- to 16- fold higher based on AUC(0-24) values. In a 2-year study in mice, incidences of hepatocellular adenomas in males and hepatocellular carcinomas in females were increased at the maximum dose used, which was 250-fold higher than the highest human dose on a mg/kg body-weight basis. Systemic exposure was 6- to 11-fold higher based on AUC(0-24).
All other chemically similar drugs in this class have induced tumors in both mice and rats at multiples of 12 to 125 times their highest recommended clinical doses, on a mg/kg body-weight basis.
Atorvastatin did not demonstrate mutagenic or clastogenic potential in four in vitro tests with and without metabolic activation or in one in vivo assay. It was negative in the Ames test with Salmonella typhimurium and Escherichia coli, and in the in vitro HGPRT forward mutation assay in Chinese hamster lung cells. Atorvastatin did not produce significant increases in chromosomal aberrations in the in vitro Chinese hamster lung cell assay and was negative in the in vivo mouse micronucleus test.No adverse effects on fertility or reproduction were observed in male rats given doses of Atorvastatin up to 175 mg/kg/day or in female rats given doses up to 225 mg/kg/day. These doses are 100 to 140 times the maximum recommended human dose on a mg/kg basis. Atorvastatin caused no adverse effects on sperm or semen parameters, or on reproductive organ histopathology in dogs given doses of 10, 40, or 120 mg/kg for two years.