


 Sign Out
Sign Out

Pharmacological Activity: Activity in the muscarinic acetylcholine receptor subtypes (in vitro): Antagonistic activity of imidafenacin was investigated on muscarinic acetylcholine receptors in vas deferens (M1), atrium (M2), and ileum (M3) using tissue specimens prepared from rabbits and guinea pigs. Imidafenacin showed higher antagonistic activity in the ileum (M3) and vas deferens (M1), compared with the atrium (M2). Major metabolites in humans showed no antagonistic activity in the muscarinic acetylcholine receptor subtypes.
Antagonistic activity of imidafenacin was investigated in recombinant human muscarinic acetylcholine receptor subtypes M1, M2, and M3 in the receptor binding assay. Imidafenacin showed high affinities for subtypes M3 and M1.
Imidafenacin inhibited acetylcholine release and urinary bladder contraction by antagonizing subtypes M3 and M1 in the tissue specimens prepared from rats.
Activity in the urinary bladder (in vivo): Imidafenacin decreased rhythmic contraction of the rat urinary bladder dose-dependently.
Imidafenacin inhibited a carbachol-induced decrease in the capacity of the rat urinary bladder dose dependently.
Selectivity for the urinary bladder: In rats, the activity ratio of inhibition of rhythmic contraction in the urinary bladder to carbachol-induced salivary secretion was about 10 times higher in imidafenacin than in propiverine hydrochloride, demonstrating high selectivity of imidafenacin for the urinary bladder.
Evaluation of rat performance in the Morris water maze task indicated that antagonistic activity of imidafenacin on subtype M1 was unlikely to impair spatial learning and memory.
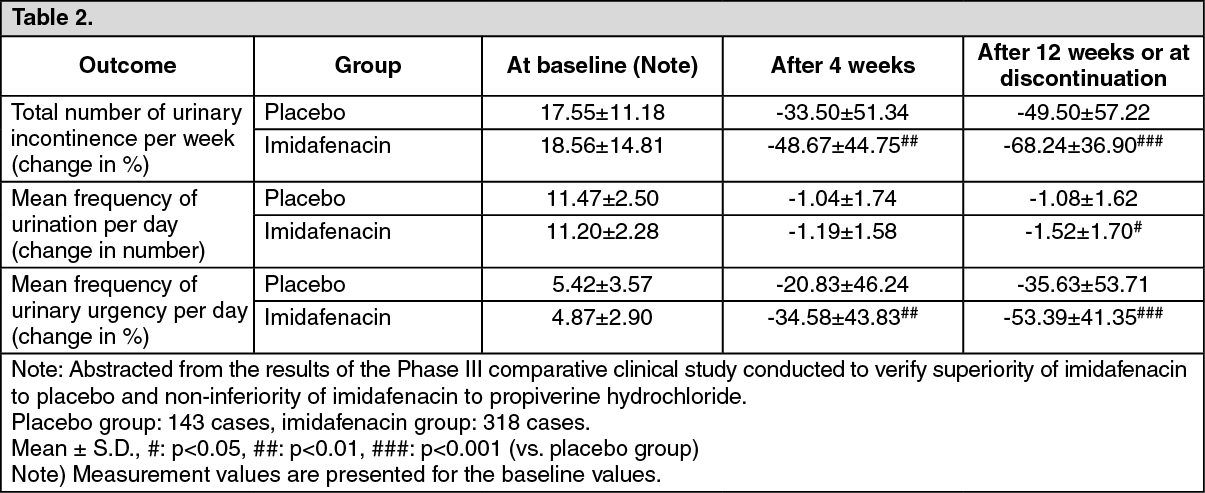
Clinical Studies: Double-blind Placebo-controlled Study: Imidafenacin was orally administered at the dose of 0.1 mg twice daily for 12 weeks to patients with overactive bladder. For the primary efficacy outcome, change in total number of urinary incontinence per week from the baseline value, significant improvement was observed in the imidafenacin group compared with the placebo group. In addition, significant improvement was also observed in changes in mean frequency of urination per day and mean frequency of urinary urgency per day from the baseline values in the imidafenacin group compared with the placebo group.
Adverse reactions in the imidafenacin group including abnormalities in laboratory test values were reported in 130 (40.5%) of 321 cases evaluated. Major adverse reactions included thirst in 87 cases (27.1%) and constipation in 30 cases (9.3%). (See Table 2.)
 Click on icon to see table/diagram/image
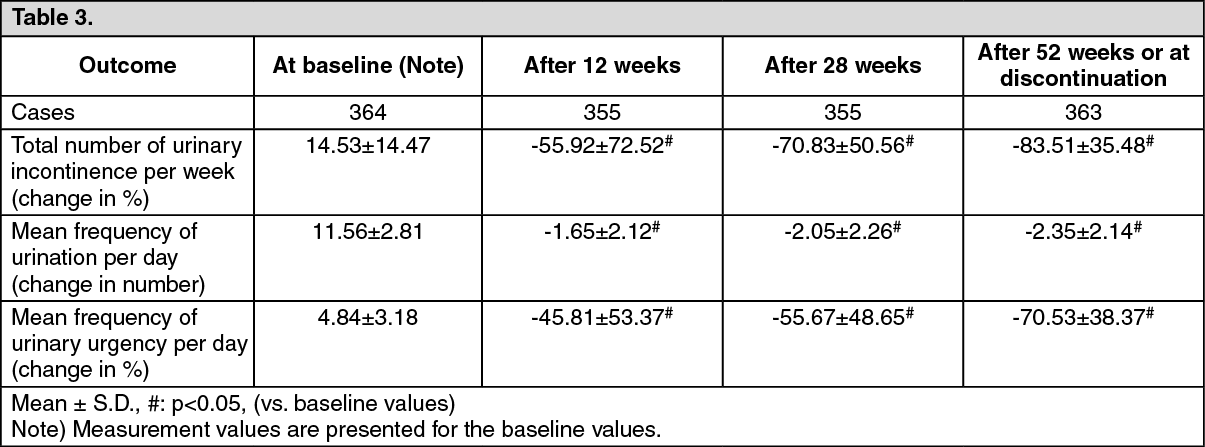
Click on icon to see table/diagram/imageLong-term Study: Imidafenacin was orally administered at the dose of 0.1 mg twice daily for 52 weeks to patients with overactive bladder. Improvement was observed in changes in total number of urinary incontinence per week, mean frequency of urination per day, and mean frequency of urinary urgency per day from the baseline values, with duration for 52 weeks without attenuation.
Adverse reactions in the imidafenacin group including abnormalities in laboratory test values were reported in 223 (46.7%) of 478 cases evaluated. Major adverse reactions included thirst in 164 cases (34.3 %) and constipation in 43 cases (9.0%). (See Table 3.)
 Click on icon to see table/diagram/image
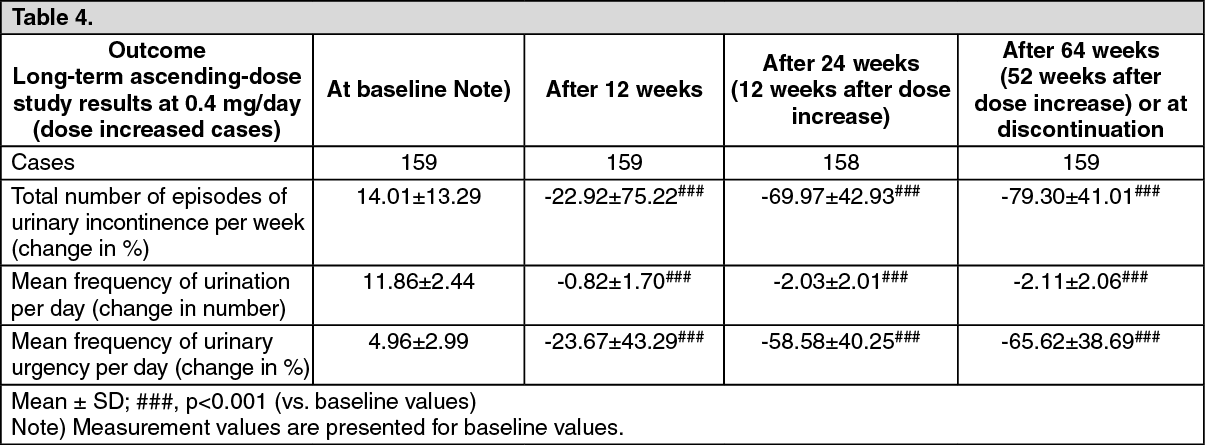
Click on icon to see table/diagram/imageLong-term Ascending-dose Study: Imidafenacin was orally administered at the dose of 0.1 mg twice daily for 12 weeks to patients with overactive bladder. Then, imidafenacin was orally administered at the dose of 0.2 mg twice daily for 52 weeks in the dose increased group, and at the dose of 0.1 mg twice daily for 40 weeks in the dose maintained group according to the criteria for dose increase. In the group of 0.4 mg/day, improvement was observed in changes in total number of urinary incontinence per week, mean frequency of urination per day, and mean frequency of urinary urgency per day from the baseline values, with duration for 64 weeks after the start of the study (52 weeks after dose increase) without attenuation.
There were 49.4% (215 of 435) patients who experienced adverse drug reactions including abnormalities in laboratory test values, reported in the safety analysis set. Among them, 62.6% (114 of 182) of patients were in the dose increased group and 39.9% (101 of 253) of patients were in the dose maintained group. The most common adverse drug reactions were dry mouth and constipation, and the incident ratios were 53.3% (97 of 182) and 18.7% (34 of 182) in the dose increased group, 26.5% (67 of 253) and 9.9% (25 of 253) in the dose maintained group, respectively. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNote: Criteria for dose increase: If all symptoms of overactive bladder failed to meet the normalization criteria (mean frequency of urinary urgency per day of 0 [disappearance], mean frequency of urination per day of less than eight, and total number of episodes of urinary incontinence per week of 0 [disappearance]) at the visit after administration of the initial dose for 12 weeks, the dose of imidafenacin may be increased when the investigator judged that the dose increase should be valid, and the patient requested the dose increase. If, however, moderate to severe adverse reaction(s) had developed before the visit after 12 weeks of administration, dose increase should not be conducted.
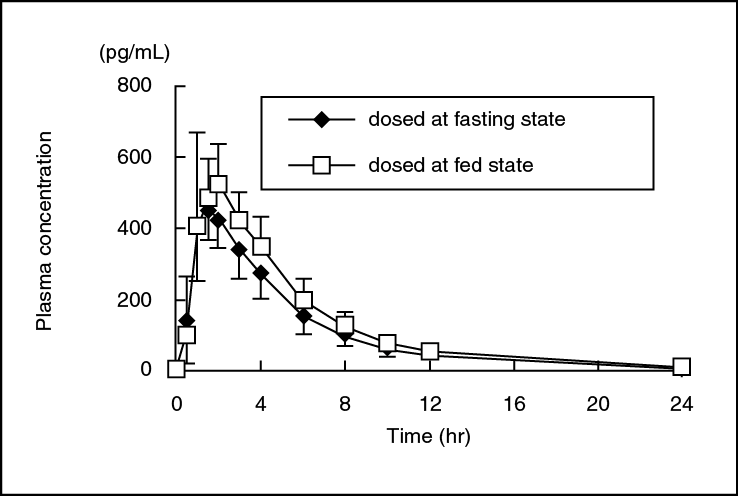
Pharmacokinetics: Plasma Concentrations: Single administration: Effect of meal: After single oral administration of 0.1 mg of imidafenacin to healthy adult males (n=12) at the fasting state, plasma concentration reached the peak (Cmax: 471 pg/mL) at 1.5 hours, and decreased with a half-life of 2.9 hours. Cmax and AUC0-12 at the fed state were about 1.3 and 1.2 times higher than those at the fasting state, respectively. (See figure and Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRepeated administration: After repeated oral administration of 0.25 mg of imidafenacin twice daily for 5 days to the healthy adult males (n=5), the time-course of plasma concentration and pharmacokinetic parameters after the final dosing were comparable to those after the initial dosing, indicating no accumulation of imidafenacin after repeated administration.
Note: The approved dosage is 0.2 mg/day, and if the efficacy is insufficient, the dosage may be increased up to 0.4 mg/day.
The elderly: After single oral administration of 0.1 mg of imidafenacin to the healthy non-elderly adult males (n=6) and the elderly males aged 65 years or more (n=9) at the fasting state, Cmax in the elderly was about 1.2 times higher than that in the non-elderly, while AUC0-∞ was comparable between the two groups. (See Table 6.)
 Click on icon to see table/diagram/image
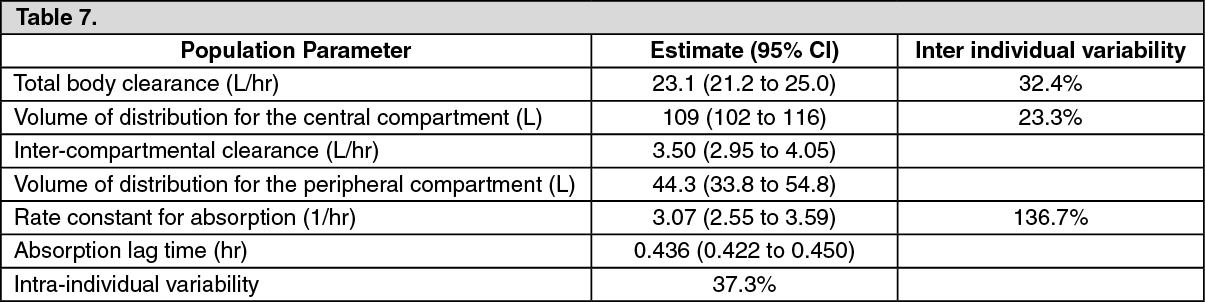
Click on icon to see table/diagram/imagePopulation pharmacokinetic (PPK) analysis: A two-compartment model involving primary absorption with a lag time in absorption was used for the analysis of population pharmacokinetics by NONMEM. Plasma concentration of imidafenacin was determined at a total of 3,168 points in 852 patients with overactive bladder aged 20 to 85 years (including 101 patients with mild hepatic dysfunction, 116 patients with mild renal dysfunction, and 14 patients with moderate renal dysfunction) and 90 healthy adults aged 20 to 75 years in the long-term study and long-term ascending-dose study. The relationship of clearance (CL/F) of imidafenacin to the following covariates was assessed: body weight, age, gender, drinking habit, smoking habit, indices for hepatic function (AST [GOT], ALT [GPT], γ-GTP, ALP, lactate dehydrogenase, and total bilirubin), indices for renal function (serum creatinine, and blood urea nitrogen), and albumin. CL/F in the patients with mild abnormality in ALP was lower than that in the normal patients by 4%. CL/F in the elderly was lower than that in the non-elderly by 14%. The other covariates including indices for renal function (serum creatinine, blood urea nitrogen) did not affect CL/F. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAbsorption (for reference: overseas data): In the healthy adult foreign males, imidafenacin was absorbed almost 100% from the gastrointestinal tract, with an absolute bioavailability of 57.8%.
Metabolism: After oral administration, about 40% of imidafenacin was subjected to first-pass effect in the liver. Major plasma metabolites included M-2 (oxidized metabolite on the imidazole ring of imidafenacin), M-4 (ring-cleaved metabolite of M-2), and M-9 (N-glucuronide of imidafenacin). Metabolism to M-2 and M-4 was primarily catalyzed by CYP3A4, and that to M-9 was by UGT1A4. In addition, imidafenacin and its major metabolites, M-2, M-4, and M-9, did not inhibit human CYP species in vitro (CYP1A2, CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4).
Excretion (for reference: overseas data): After single oral administration of 14C-imidafenacin to healthy adult foreign males (n=6) at a dose of 0.25 mg at the fasting state, 95% of the dose was recovered in the urine and feces until 192 hours after administration (65.6% in the urine, and 29.4% in the feces). Less than 10% of the dose was excreted unchanged in the urine, and none of the dose was excreted unchanged in the feces.
Note) The approved dosage is 0.2 mg/day, and if the efficacy is insufficient, the dosage may be increased up to 0.4 mg/day.
Protein Binding: The protein binding ratio of imidafenacin ranged from 87.1 to 88.8%. Major binding proteins were albumin and α1-acid glycoprotein.
Drug Interactions: Itraconazole: After 0.1 mg of imidafenacin was orally co-administered to healthy adult males (n=10) treated with 200 mg of itraconazole once daily for 9 days, Cmax and AUC0-∞ of imidafenacin increased to 1.3 and 1.8 times those after imidafenacin was administered alone, respectively.
(For reference) Distribution in animals (in rats): After single oral administration of imidafenacin to rats, concentration in the bladder reached maximum at 1 hour after administration, and decreased with a half-life of 1.8 hours, more slowly than in the serum. Cmax and AUC0-12 in the bladder were 10.7 and 25.4 times higher than those in the serum, respectively.