


 Sign Out
Sign Out


In addition to its activity as a single agent, an additive effect was demonstrated in an in vitro study when lapatinib and 5-FU (the active metabolite of capecitabine) were used in combination in the 4 tumor cell lines tested. The clinical significance of these in vitro data is unknown.
The combination of lapatinib and trastuzumab may offer complementary MOAs and possible non-overlapping mechanisms of resistance. The growth inhibitory effects of lapatinib were evaluated in trastuzumab-conditioned cell lines. Lapatinib retained significant activity against HER2-amplified breast cancer cell lines selected for long-term growth in a trastuzumab-containing medium in vitro and was synergistic in combination with trastuzumab in these cell lines. These findings suggest non-cross-resistance between these two HER2/neu (ErbB2) directed agents.
Hormone-sensitive breast cancer cells (estrogen receptor [ER] positive and/or progesterone receptor [PgR]-positive) that co-express HER2 tend to be resistant to established endocrine therapies. Hormone-sensitive breast cancer cells that initially lack EGFR or HER2 will up regulate these receptors as the tumor becomes resistant to endocrine therapy. Randomized trials in hormone sensitive metastatic breast cancer indicate that a HER2 or EGR tyrosine kinase inhibitor may improve PFS when added to endocrine therapy.
Pharmacodynamics: Cardiac electrophysiology: QT prolongation: Study EGF114271: The effect of lapatinib on the QTc-interval was evaluated in a single-blind, placebo-controlled, single sequence (placebo and active treatment) crossover study in patients with advanced solid tumors (N=58). During the 4-day treatment period, 3 doses of matching placebo were administered 12 hours apart in the morning and evening on day 1 and in the morning on day 2. This was followed by 3 doses of 2000 mg lapatinib administered in the same way. Measurements, including ECGs and pharmacokinetic samples were done at baseline and at the same time points on day 2 and day 4.
In the evaluable population (N=37), the maximum mean ΔΔQTcF (90% CI) of 8.75 ms (4.08, 13.42) was observed 10 hours after ingestion of the third dose of 2000 mg lapatinib. The ΔΔQTcF exceeded the 5 ms threshold and the upper bound 90% CIs exceeded the 10 ms threshold at multiple time points. The results for the PD population (N=52) were consistent with those from the evaluable population (maximum ΔΔQTcF (90% CI) of 7.91 ms (4.13, 11.68) observed 10 hours after ingestion of the third dose of lapatinib. The PK/PD analyses confirmed a positive relationship between lapatinib plasma concentrations and ΔΔQTcF.
Clinical Studies: The combination of lapatinib (Tykerb) with capecitabine or paclitaxel demonstrated superior efficacy versus capecitabine or paclitaxel monotherapy in study EGF100151.
Data in two randomized studies in the metastatic setting (EGF111438 (CEREBREL) and EGF108919 (COMPLETE) show that lapatinib (Tykerb) combined with chemotherapy is less effective than trastuzumab combined with chemotherapy.
The combination of lapatinib (Tykerb) with trastuzumab was evaluated in the randomized clinical study EGF104900 and demonstrated superior efficacy versus lapatinib (Tykerb) alone in MBC patients who progressed on a prior trastuzumab-containing regimen.
Lapatinib (Tykerb) was also studied in combination with letrozole and had superior efficacy versus letrozole alone in HER2+, HR+ advanced or metastatic breast cancer patients.
See as follows for details.
Lapatinib (Tykerb) is not indicated in the adjuvant setting.
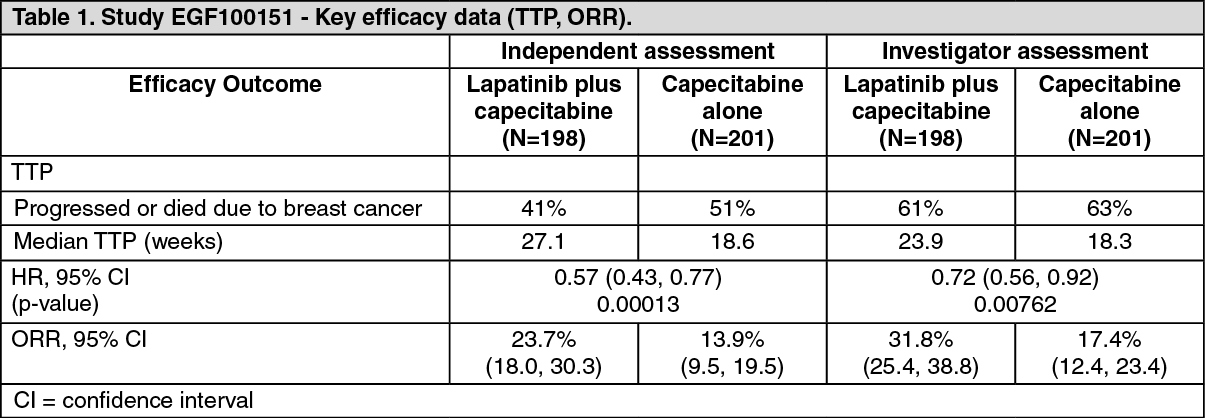
Combination treatment with lapatinib (Tykerb) and capecitabine: Study EGF100151: The efficacy and safety of lapatinib (Tykerb) in combination with capecitabine in breast cancer was evaluated in the randomized phase III study EGF100151. Patients eligible for enrolment had HER2/neu (over-expressing (IHC 3+ or IHC 2+ and FISH positive), locally advanced or metastatic breast cancer, progressing after prior treatment including taxanes, anthracyclines and trastuzumab. LVEF was evaluated in all patients (using echocardiogram [Echo] or multi gated acquisition scan [MUGA]) prior to initiation of treatment with lapatinib (Tykerb) to ensure baseline LVEF was within the institutionals normal limits. In clinical studies LVEF was monitored at approximately 8 week intervals during treatment with lapatinib to ensure it did not fall below the institutions lower limit of normal. The majority of LVEF decreases (greater than 60% of events) were observed during the first 9 weeks of treatment; however, limited data was available for long term exposure.
Patients were randomized to receive either lapatinib (Tykerb) 1250 mg once daily (continuously) plus capecitabine (2000 mg/m2/day on days 1 to 14 every 21 days), or to receive capecitabine alone (2500 mg/m2/day on days 1 to 14 every 21 days). Study treatment was given until disease progression, or withdrawal for another reason. The primary endpoint was time to progression (TTP) as assessed by an independent review panel. The results as follows are based on both the investigator's assessment and review by an independent review panel.
The results at the data cut-off date of 03 April 2006 (the date at which further enrolment to the study was halted), showed a significant increase in TTP for patients receiving lapatinib plus capecitabine (representing a 43% reduction in the risk of disease progression or death due to breast cancer versus capecitabine monotherapy, as assessed by the independent review panel). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe overall response rate as assessed by an independent review panel was 23.7% for patients receiving lapatinib plus capecitabine and 13.9% for patients receiving capecitabine. Median duration of response was 32.1 weeks and 30.6 weeks respectively.
On the combination arm, there were 4 (2%) progressions in the central nervous system (CNS) versus the 13 (6%) progressions on the capecitabine monotherapy arm, as assessed by an independent review panel (see Lapatinib effect on CNS metastasis as follows).
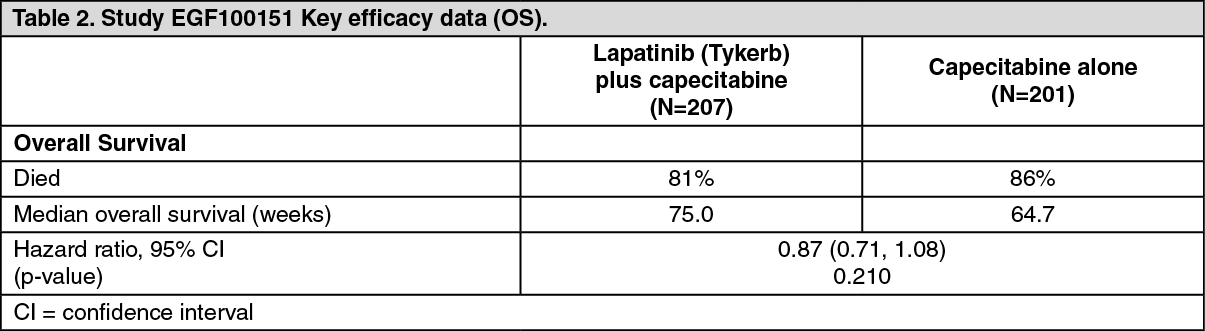
At the time enrollment was halted (3 April 2006), 399 patients were randomized to study therapy and 9 other patients were being screened. All 9 patients in screening, and all those already receiving capecitabine monotherapy, were offered combination treatment. In total, 207 patients were assigned to the combination therapy and 201 patients to capecitabine monotherapy.
An analysis of survival data to 01 October 2008 is summarized in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAfter the study was halted, 36 patients crossed over from capecitabine to lapatinib (Tykerb) plus capecitabine, of whom 26 crossed over prior to disease progression while on capecitabine alone. To isolate the treatment effect in the presence of cross-over, Cox regression analysis considering crossover as a time-dependent covariate and treatment effect was performed. The results from this analysis suggest a clinically relevant 20% reduction in risk of death, with a treatment effect hazard ratio of 0.80 (95% [CI]: 0.64, 0.99; p=0.043).
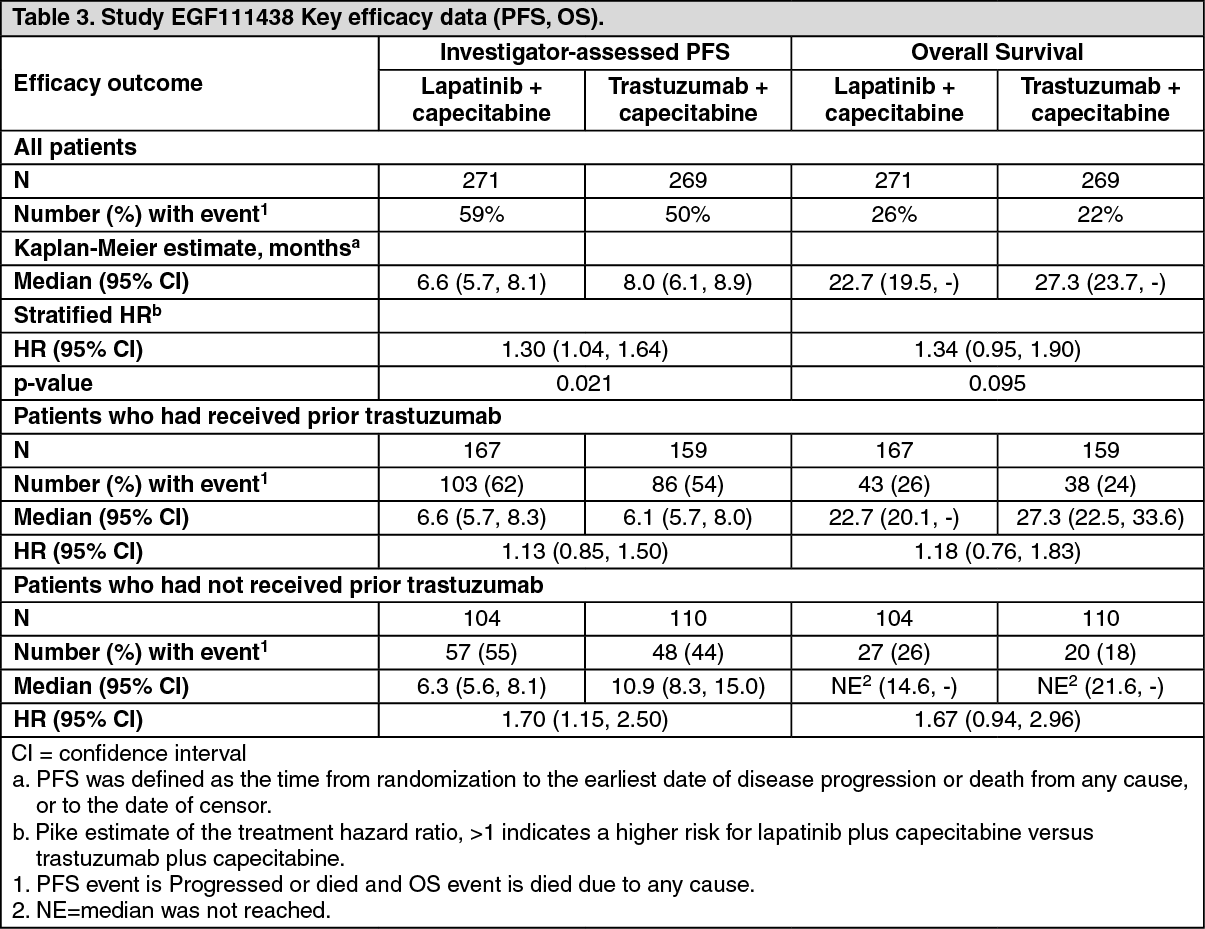
Study EGF111438 (CEREBEL): A randomized Phase III study (EGF111438) (N=540) compared the effect of lapatinib in combination with capecitabine to trastuzumab in combination with capecitabine on the incidence of the CNS as the site of first relapse in women with HER2 overexpressing metastatic breast cancer. Patients were randomized to either 1250 mg lapatinib once daily (continuously) plus capecitabine (2000 mg/m2/day on days 1-14 every 21 days), or trastuzumab (loading dose of 8 mg/kg followed by 6 mg/kg infusions every 3 weeks) plus capecitabine (2500 mg/m2/day, on days 1-14, every 21 days). Randomization was stratified by prior trastuzumab treatment and number of prior treatments for metastatic disease (none versus ≥1st line). The study was stopped when a pre-planned interim analysis (N=475) showed superior efficacy of the trastuzumab plus capecitabine arm and a low incidence of CNS events.
The final analysis confirmed that the primary endpoint results were inconclusive due to a low number of CNS events (8 patients (3.2%) in the lapatinib plus capecitabine arm experienced CNS metastasis as site of first progression, versus 12 patients (4.8%) in the trastuzumab plus capecitabine arm) (see Lapatinib effect on CNS metastasis as follows). The final results of PFS and OS are shown in Table 3. The final analysis confirmed the superior efficacy of the trastuzumab plus capecitabine arm. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLapatinib effect on CNS metastasis: In terms of objective responses, lapatinib (Tykerb) monotherapy has demonstrated minimal activity in the treatment of established CNS metastases.
Lapatinib is not recommended for the prevention of CNS metastases.
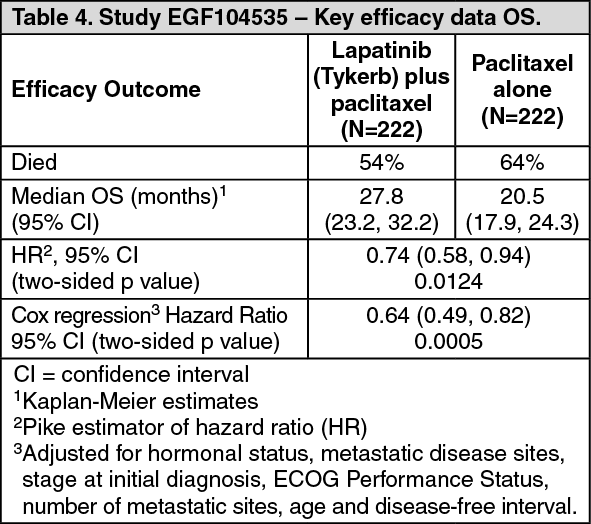
Combination treatment with lapatinib (Tykerb) and paclitaxel: Study EGF104535: The efficacy and safety of lapatinib (Tykerb) in combination with paclitaxel in breast cancer were evaluated in a randomized phase III study EGF104535. Patients had histologically confirmed invasive breast cancer (stage IV) with HER2 overexpression (documented by IHC or FISH) and had not received prior therapy for metastatic disease.
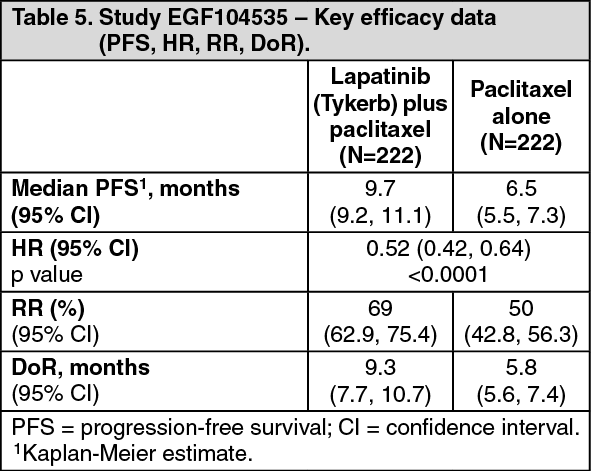
Patients were randomized to paclitaxel (80 mg/m2 IV on days 1, 8, and 15 of a 28 day schedule) and either 1500 mg/day lapatinib (Tykerb) or placebo once daily. Patients received a minimum of 6 cycles of lapatinib (Tykerb) plus paclitaxel. After the 6 cycles were completed, patients continued on lapatinib (Tykerb) or placebo until disease progression or unacceptable toxicity. The primary endpoint was OS. 444 patients were enrolled in this study. Of the 222 who were on paclitaxel plus placebo, 149 (67%) with disease progression entered the open-label extension phase and received lapatinib (Tykerb) monotherapy. The median age was 50 years and 7% were older than 65 years. 86% were Asian, 8% Hispanic, and 5% Caucasian. The overall survival data are summarized in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA summary of other efficacy endpoints are provided in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStudy EGF30001: Another randomized, double-blind, controlled phase III study evaluated lapatinib (Tykerb) and paclitaxel as first-line therapy for metastatic breast cancer in patients with negative or untested ErbB2 status previously untreated in the metastatic setting. Patients (N= 579) were randomized 1:1 to paclitaxel (175 mg/m2 IV over 3 hours on day 1, every 3 weeks) and either 1500 mg/day lapatinib (Tykerb) or placebo once daily. 64% were Caucasian, 18% Hispanic, and 11% Asian. 91 patients (16%) had HER2-positive disease. The primary endpoint was time-to-progression (TTP); secondary endpoints included progression-free survival (PFS), tumor response rate (RR), clinical benefit rate (CBR), overall survival (OS) and safety. No significant differences in TTP or PFS were observed between treatment arms in the unselected ITT population. The median PFS in the HER2-positive subgroup was 34.4 weeks (95% CI: 32.1, 41.6) for lapatinib (Tykerb) plus paclitaxel combination versus 22.6 weeks (95% CI: 20.1, 32.9) for paclitaxel plus placebo (HR 0.56; 95% CI: 0.34, 0.90; p = 0.007). The OS analyses of the ITT population and HER2 positive subgroup are presented in Table 6. (See Table 6.)
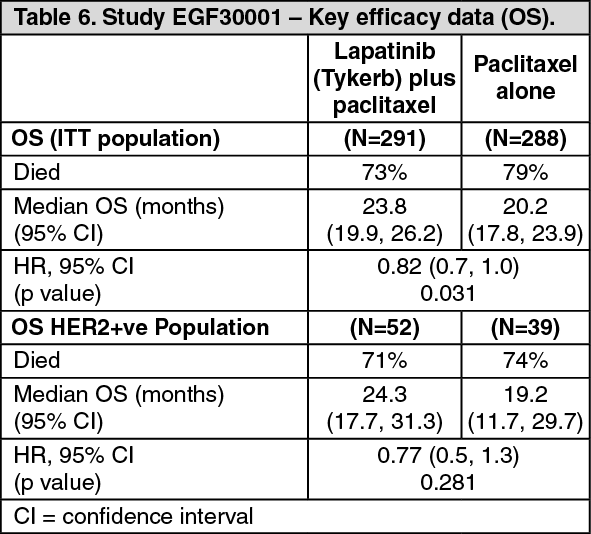 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEGF108919 (COMPLETE): The randomized Phase III study (EGF108919) (N=652) compared the efficacy and safety of lapatinib plus a taxane followed by lapatinib alone versus trastuzumab plus a taxane followed by trastuzumab alone as first line therapy for women with HER2 positive metastatic breast cancer. Patients were randomized to either 1250 mg lapatinib once daily plus 80 mg/m2 paclitaxel: once weekly (days 1, 8 and 15 of a 4-week cycle) or 75 mg/m2 docetaxel once every 3 weeks (days 1 of a 3 week cycle) for 24 weeks followed by 1500 mg lapatinib once daily, or trastuzumab once weekly (loading dose 4mg/kg followed by 2mg/kg weekly infusions) plus 80 mg/m2 paclitaxel: once weekly (days 1, 8 and 15 of a 4-week cycle) or trastuzumab every 3 weeks (loading dose 8 mg/kg followed by 6 mg/kg once every 3 weeks) plus 75 mg/m2 docetaxel once every 3 weeks (days 1 of a 3 week cycle) for 24 weeks followed by 6 mg/kg trastuzumab: once every 3 weeks.
The study was stopped when a pre-planned interim analysis showed that the trastuzumab arm was superior to the lapatinib arm. This was confirmed by the final analysis (see Table 7).
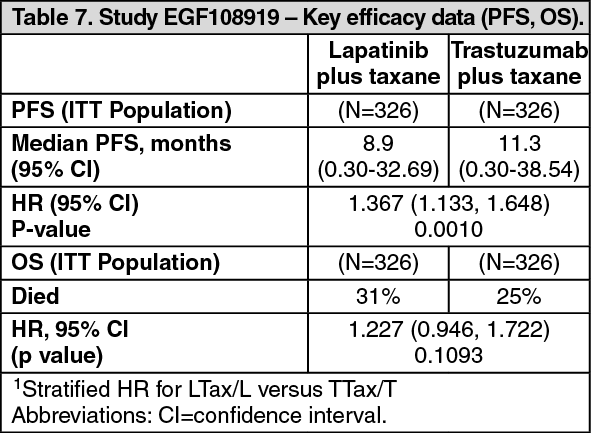 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCombination treatment with lapatinib (Tykerb) and trastuzumab: Study EGF104900: The efficacy and safety of lapatinib (Tykerb) in combination with trastuzumab in metastatic breast cancer were evaluated in the randomized trial EGF104900.
Eligible patients were women with stage IV ErbB2 gene amplified (or protein overexpressing) metastatic breast cancer exposed to treatment with anthracyclines and taxanes. In addition, per the protocol, patients were to be reported by the investigators as having progressed on their most recent trastuzumab containing regimen in the metastatic setting. The median number of prior trastuzumab-containing regimens in the metastatic setting was three. Patients were randomized to receive either oral lapatinib (Tykerb) 1,000 mg once daily plus trastuzumab 4 mg/kg administered as an intravenous (IV) loading dose, followed by 2 mg/kg IV weekly (N = 148), or oral lapatinib (Tykerb) 1,500 mg once daily (N = 148). Patients with objective disease progression after at least 4 weeks of lapatinib (Tykerb) monotherapy were eligible to crossover to combination therapy. Of the 148 patients who received monotherapy, 77 (52%) elected to receive combination treatment at the time of disease progression.
The primary objective of this study was to evaluate and compare PFS in patients with metastatic breast cancer treated with lapatinib (Tykerb) and trastuzumab compared with lapatinib (Tykerb) monotherapy. Secondary objectives were to evaluate and compare the two treatment arms with respect to OS, overall tumor response rate, clinical benefit response rate and time to response.
The median age was 51 years and 13% were 65 years or older. 94% were Caucasian. Most patients in both treatment arms had visceral disease (215 [73%] overall). Half of the patients in the study population were estrogen receptor negative and progesterone receptor negative (150 [51%] overall). A summary of efficacy endpoints is provided in Table 8 and OS data in Table 9. Subgroup analysis results based on a predefined stratification factor (hormone receptor status) are shown in Table 10. (See Tables 8,9 and 10.)
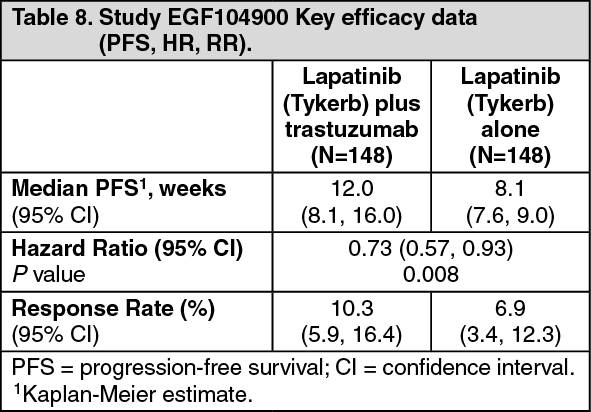 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image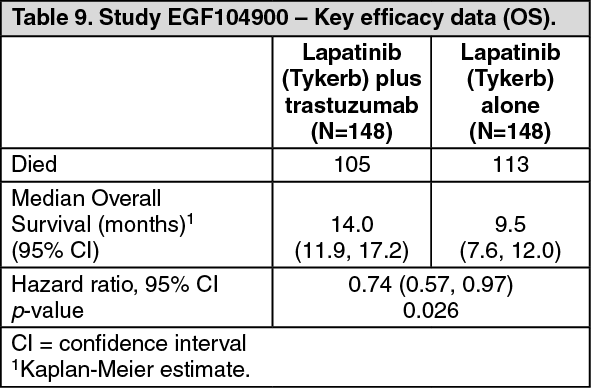 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCombination treatment with lapatinib (Tykerb) and letrozole: Study EGF30008: Lapatinib (Tykerb) was studied in combination with letrozole for the treatment of advanced or metastatic breast cancer in hormone receptor positive (estrogen receptor [ER] positive and/or progesterone receptor [PgR] positive) postmenopausal women.
EGF30008 was a randomized, double-blind, placebo-controlled study in patients with hormone-sensitive locally advanced or metastatic breast cancer (MBC), who had not received prior therapy for metastatic disease. 1286 patients were randomized to 2.5 mg letrozole once daily plus 1500 mg lapatinib (Tykerb) once daily (N=642) or letrozole plus placebo (N=644). Randomization was stratified by sites of disease and prior adjuvant anti-estrogen therapy. HER2 receptor status was retrospectively determined by central laboratory testing. Of all patients randomized to treatment, 219 had tumors over-expressing the HER2 receptor which was the pre-specified primary population for the analysis of efficacy.
In the HER2-positive population, investigator-determined progression-free survival (PFS) was significantly greater with letrozole plus lapatinib (Tykerb) than with letrozole plus placebo (see Table 11).
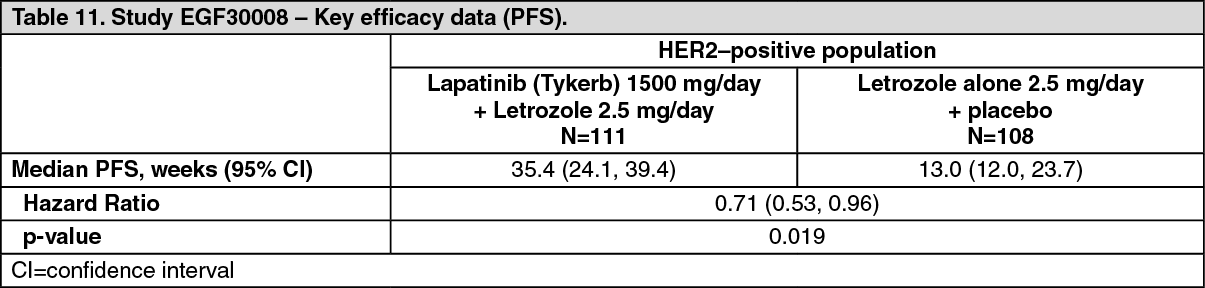 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe benefit of lapatinib (Tykerb) plus letrozole on PFS in the HER2-positive population was confirmed in a pre-planned Cox regression analysis (HR=0.65 (95% CI 0.47-0.89) p=0.008). In addition to a PFS benefit seen in this population, combination therapy of lapatinib (Tykerb) and letrozole improved objective response rate (27.9% and 14.8% respectively) and in Clinical Benefit Rate (47.7% and 28.7% respectively) compared with letrozole treatment alone.
At the time of the final PFS analysis (with median follow-up of 2.64 years), the OS data were not mature and there was no significant difference between treatment groups in the HER2-positive population; this had not changed with additional follow-up (>7.5 years median follow-up time; Table 12). (See Table 12.)
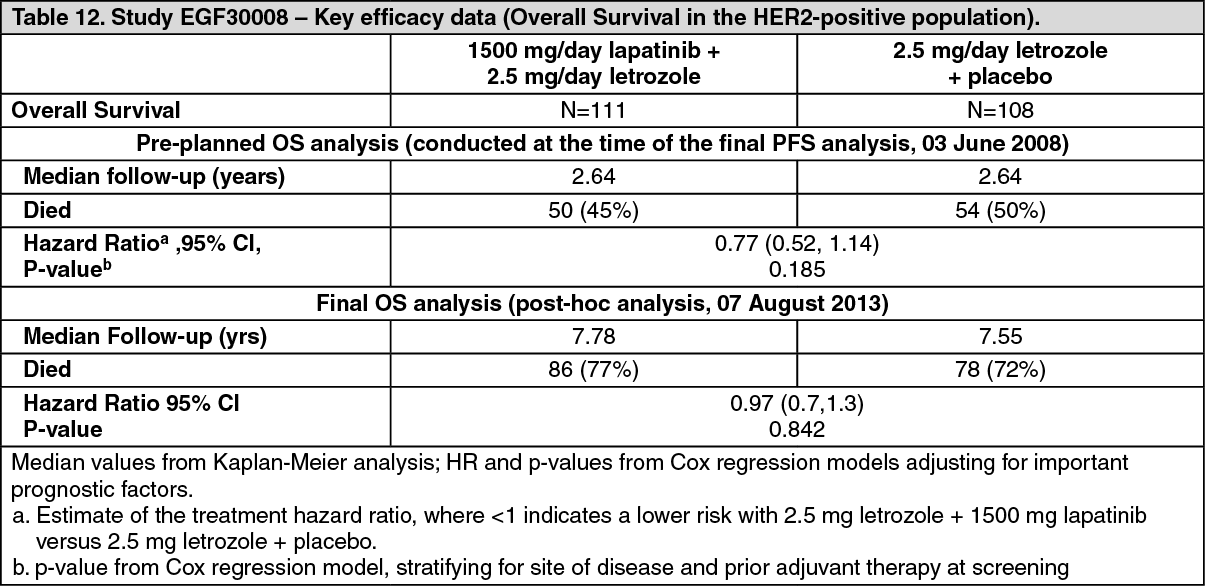 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Absorption of lapatinib following oral administration of lapatinib is incomplete and variable (approximately 50 to 100% coefficient of variation in AUC). Serum concentrations appear after a median lag time of 0.25 hours (range 0 to 1.5 hours). Peak plasma concentrations (Cmax) of lapatinib are achieved approximately 4 hours after administration. Daily dosing of 1250 mg produces steady state geometric mean (95% CI) Cmax values of 2.43 (1.57 to 3.77) microg/mL and AUC values of 36.2 (23.4 to 56) microg.hr/mL.
Systemic exposure to lapatinib is increased when administered with food (see Dosage & Administration and Interactions). Lapatinib AUC values were approximately 3- and 4-fold higher (Cmax approximately 2.5 and 3-fold higher) when administered with a low-fat (5% fat [500 calories]) or high-fat (50% fat [1,000 calories]) meal, respectively.
Distribution: Lapatinib is highly bound (>99%) to albumin and alpha-1 acid glycoprotein. In vitro studies indicate that lapatinib is a substrate for the transporters BCRP (ABCG2) and Pgp (ABCB1). Lapatinib has also been shown to inhibit Pgp (IC50 2.3 microgram/mL), BCRP (IC50 0.014 microgram/mL) and the hepatic uptake transporter OATP 1B1 (IC50 2.3 microgram/mL), in vitro at clinically relevant concentrations. The clinical significance of these effects on the pharmacokinetics of other drugs or the pharmacological activity of other anti-cancer agents is not known. Lapatinib does not significantly inhibit the OAT or OCT renal transporters (in vitro IC50 values were ≥6.9 microgram/mL).
Biotransformation/metabolism: Lapatinib undergoes extensive metabolism, primarily by CYP3A4 and CYP3A5, with minor contributions from CYP2C19 and CYP2C8 to a variety of oxidated metabolites, none of which account for more than 14% of the dose recovered in the feces or 10% of the lapatinib concentration in plasma.
Elimination: The half-life of lapatinib measured after single doses increases with increasing dose. However, daily dosing of lapatinib results in achievement of steady state within 6 to 7 days, indicating an effective half-life of about 1 day. Lapatinib is predominantly eliminated through metabolism by CYP3A4/5. The primary route of elimination for lapatinib and its metabolites is in feces, with less than 2% of the dose (as lapatinib and metabolites) excreted in urine. Recovery of lapatinib in feces accounts for a median 27% (range 3 to 67%) of an oral dose.
In vitro evaluation of drug interaction potential: Lapatinib inhibits CYP3A (Ki 0.6 to 2.3 microgram/mL) and CYP2C8 (0.3 microgram/mL) in vitro at clinically relevant concentrations. Lapatinib did not significantly inhibit the following enzymes in human liver microsomes: CYP1A2, CYP2C9, CYP2C19, and CYP2D6 or UGT (in vitro IC50 values were ≥6.9 microgram/mL)
Special populations: Pediatric patients (below 18 years): The pharmacokinetics of Lapatinib (Tykerb) in pediatric patients have not been established.
Geriatric patients (65 years or above): Age does not appear to affect lapatinib pharmacokinetics, based on the analysis of individual study results. An examination of combined data, spanning a range of 18 to 82 years suggests no obvious effect.
Gender: Gender does not appear to affect lapatinib pharmacokinetics. An examination of combined data, including >300 females and >450 males, suggests no obvious difference.
Race/ethnicity: The available study data indicates no obvious distinction related to race/ethnicity.
Renal impairment: Lapatinib pharmacokinetics have not been specifically studied in patients with renal impairment or in patients undergoing hemodialysis. However, renal impairment is unlikely to affect the pharmacokinetics of lapatinib given that less than 2% of an administered dose (as unchanged lapatinib and metabolites) is eliminated by the kidneys.
Hepatic impairment: Lapatinib pharmacokinetics were examined in subjects with moderate (N = 8) or severe (N = 4) hepatic impairment and in 8 healthy control subjects. Systemic exposure (AUC) to lapatinib after a single oral 100 mg dose increased approximately 56% and 85% in patients with moderate and severe hepatic impairment, respectively. Administration of lapatinib (Tykerb) in patients with hepatic impairment requires caution due to increased drug exposure. Dose reduction is recommended for patients with severe pre-existing hepatic impairment. In patients who develop severe hepatotoxicity while on therapy, lapatinib (Tykerb) should be discontinued permanently (see Dosage & Administration and Precautions).
Pharmacogenomics: Polymorphic variations in drug-metabolizing enzymes, transporters, receptors, and other proteins that might affect lapatinib pharmacokinetics have not been explored.
The HLA alleles DQA1*02:01 and DRB1*07:01 were associated with hepatotoxicity in a genetic substudy of a monotherapy trial with lapatinib (Tykerb) (see Precautions).
Toxicology: Non-Clinical Safety Data: Safety pharmacology: No neurological, respiratory or cardiovascular effects were identified in a panel of in vitro safety pharmacology studies or in in vivo animal studies with lapatinib.
Repeat dose toxicity: Lapatinib was evaluated in repeat dose toxicity studies for up to 6 months in rats and up to 9 months in dogs. The principal treatment-related effects were inflammation and atrophy of the skin and adnexal structures, and degeneration and inflammation of the GI tract and accessory digestive organs (including liver), mammary gland and prostate. These effects were seen at ≥60 mg/kg/day in rats and ≥40 mg/kg/day in dogs. The NOAEL in male and female rats was 60 mg/kg/day and 10 mg/kg/day, respectively, with AUC estimates of 24.7 microg.h/mL and 25.1 microg.h/mL, respectively. The NOAEL in male and female dogs was 10 mg/kg/day with AUC estimates of 5.4 microg.h/mL and 8.2 microg.h/mL, respectively. Corresponding systemic exposures at these dose levels were 0.5 and 0.6-fold the human clinical exposure for male and female rats, respectively, and 0.1 and 0.2-fold the human clinical exposure for male and female dogs, respectively.
Carcinogenicity and mutagenicity: In oral carcinogenicity studies with lapatinib, severe skin lesions were seen at the highest doses tested (150 and 300 mg/kg/day in male mice and 300 mg/kg/day in female mice, and 500 mg/kg/day in male rats and 300 mg/kg/day in female rats). Compared to humans given 1250 mg lapatinib (Tykerb) and 2000 mg/m2, these doses produced exposures based on AUC up to 1.7-fold higher in mice and male rats, and up to 12-fold higher in female rats. There was no evidence of carcinogenicity in mice. In rats, an increase in the incidence of benign hemangioma of the mesenteric lymph node occurred in males given 120 mg/kg/day and females given 180 mg/kg/day, but was within the historical control background range. There was also an increase in renal infarcts and papillary necrosis in female rats at ≥60 mg/kg/day and 180 mg/kg/day, respectively (approximate 5.8 and 8.2-fold the clinical exposure in humans given 1250 mg lapatinib and 2000 mg/m2 capecitabine, respectively). The relevance of these renal findings for humans is uncertain.
Lapatinib was not clastogenic or mutagenic in a battery of assays including the Chinese hamster chromosome aberration assay, the Ames assay, human peripheral lymphocyte chromosome aberration assay and an in vivo rat bone marrow chromosome aberration assay.
Reproductive toxicity: For data regarding the impact of lapatinib (Tykerb) on reproductive function, (see Use in Pregnancy & Lactation).