Each tablet contains: Telmisartan, USP 40 mg or 80 mg.
Excipient with known effect: These products contain lactose.
If the patient has been told by the doctor that the patient has an intolerance to some sugars, contact the doctor before taking this medicinal product. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Angiotensin II Receptor Blocker.
Pharmacology: Telmisartan is an orally active and specific angiotensin II receptor (type AT1) antagonist. Telmisartan displaces angiotensin II with very high affinity from its binding site at the AT1 receptor subtype, which is responsible for the known actions of angiotensin II. Telmisartan does not exhibit any partial agonist activity at the AT1 receptor. Telmisartan selectively binds the AT1 receptor. The binding is long-lasting. Telmisartan does not show affinity for other receptors, including AT2 and other less characterized AT receptors. The functional role of these receptors is not known, nor is the effect of their possible overstimulation by angiotensin II, whose levels are increased by telmisartan. Plasma aldosterone levels are decreased by telmisartan. Telmisartan does not inhibit human plasma renin or block ion channels. Telmisartan does not inhibit angiotensin converting enzyme (kininase II), the enzyme which also degrades bradykinin. Therefore, it is not expected to potentiate bradykinin-mediated adverse effects.
Pharmacokinetics: Absorption of telmisartan is rapid although the amount absorbed varies. The mean absolute bioavailability for telmisartan is about 50%. Telmisartan is largely bound to plasma protein (>99.5%), mainly albumin and alpha-1 acid glycoprotein. Telmisartan is metabolized by conjugation to the glucuronide of the parent compound. No pharmacological activity has been shown for the conjugate. Telmisartan is characterized by biexponential decay pharmacokinetics with a terminal elimination half-life of >20 hours. There is no evidence of clinically relevant accumulation of telmisartan taken at the recommended dose. Plasma concentrations were higher in females than in males, without relevant influence on efficacy. After oral administration, telmisartan is nearly exclusively excreted with the feces, mainly as unchanged.
Hypertension: Treatment of essential hypertension in adults.
Cardiovascular prevention: Reduction of cardiovascular morbidity in adults with manifest atherothrombotic cardiovascular disease (history of coronary heart disease, stroke, or peripheral arterial disease) or type 2 diabetes mellitus with documented target organ damage.
Hypertension: Usual starting dose: 40 mg once a day.
Most of the antihypertensive effect is apparent within 2 weeks and maximal reduction is generally attained after 4 weeks.
When additional blood pressure reduction beyond that achieved with 80 mg telmisartan is required, a diuretic may be added.
No initial dosage adjustment is necessary for elderly patients or patients with renal impairment, including those on hemodialysis. Patients on dialysis may develop orthostatic hypotension; their blood pressure should be closely monitored.
Cardiovascular risk reduction: Recommended dose: 80 mg once a day.
It is not known whether doses lower than 80 mg of telmisartan are effective in reducing the risk of cardiovascular morbidity and mortality.
When initiating telmisartan therapy for cardiovascular risk reduction, monitoring of blood pressure is recommended, and if appropriate, adjustment of medications that lower blood pressure may be necessary.
Telmisartan tablets may be administered with other antihypertensive agents. Telmisartan tablets may be administered with or without food.
The most prominent manifestations of telmisartan overdose were hypotension and tachycardia; bradycardia dizziness, increase in serum creatinine, and acute renal failure have also been reported. Telmisartan is not removed by hemodialysis. The patient should be closely monitored, and the treatment should be symptomatic and supportive. Management depends on the time since ingestion and the severity of the symptoms. Suggested measures include induction of emesis and/or gastric lavage. Activated charcoal may be useful in the treatment of overdosage. Serum electrolytes and creatinine should be monitored frequently. If hypotension occurs, the patient should be placed in a supine position, with salt and volume replacement given quickly.
Second and third trimesters of pregnancy.
Biliary obstructive disorders.
Severe hepatic impairment.
Concomitant use with aliskiren-containing products in patients with diabetes mellitus or renal impairment (GFR <60 mL/min/1.73m2).
Avoid Use in Pregnancy.
When pregnancy is detected, discontinue Telmisartan as soon as possible. Drugs that act directly on the renin-angiotensin system can cause injury and even death to the developing fetus.
Intravascular volume depletion: Symptomatic hypotension, especially after the first dose, may occur in patients who are volume and/or sodium depleted by vigorous diuretic therapy, dietary salt restriction, diarrhea or vomiting. Such conditions should be corrected before the administration of telmisartan.
Renovascular hypertension: There is an increased risk of severe hypotension and renal insufficiency when patients with bilateral renal artery stenosis or stenosis of the artery to a single functioning kidney are treated with medicinal products that affect the renin-angiotensin-aldosterone system.
Dual blockade of the renin-angiotensin-aldosterone system (RAAS): There is evidence that the concomitant use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren increases the risk of hypotension, hyperkalemia and decreased renal function (including acute renal failure). Dual blockade of RAAS through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is therefore not recommended. If dual blockade therapy is considered absolutely necessary, this should only occur under specialist supervision and subject to frequent close monitoring of renal function, electrolytes and blood pressure. ACE-inhibitors and angiotensin II receptor blockers should not be used concomitantly in patients with diabetic nephropathy.
Hyperkalemia: As with other medicinal products that affect the renin-angiotensin-aldosterone system, hyperkalemia may occur during the treatment with telmisartan, especially in the presence of renal impairment, overt proteinuria due to diabetic renal disease, and/or heart failure. Close monitoring of serum potassium in patients at risk is recommended.
Aortic and mitral valve stenosis, obstructive hypertrophic cardiomyopathy: As with other vasodilators, special caution is indicated in patients suffering from aortic or mitral stenosis, or obstructive hypertrophic cardiomyopathy.
Primary aldosteronism: Patients with primary aldosteronism generally will not respond to antihypertensive medicinal products acting through inhibition of the renin-angiotensin system. Therefore, the use of telmisartan is not recommended.
General: In patients whose vascular tone and renal function depend predominantly on the activity of the renin-angiotensin-aldosterone system (e.g. patients with severe congestive heart failure or underlying renal disease, including renal artery stenosis), treatment with angiotensin converting enzyme inhibitors or angiotensin-II receptor antagonists that affect this system has been associated with acute hypotension, azotemia, oliguria, or rarely acute renal failure. As with any antihypertensive agent, excessive blood pressure decrease in patients with ischemic cardiopathy or ischemic cardiovascular disease could result in a myocardial infarction or stroke.
Renal impairment and kidney transplantation: When telmisartan is used in patients with impaired renal function, a periodic monitoring of potassium and creatinine serum levels is recommended. There is no experience regarding the administration of telmisartan in patients with a recent kidney transplantation.
Pregnancy Category D. The use of ARBs is not recommended during the first trimester of pregnancy. The use of ARBs is contraindicated during the second and third trimesters of pregnancy.
Epidemiological evidence regarding the risk of teratogenicity following exposure to ACE inhibitors during the first trimester of pregnancy has not been conclusive; however, a small increase in risk cannot be excluded. Whilst there is no controlled epidemiological data on the risk with ARBs, similar risks may exist for this class of drugs. Unless continued ARB therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with ARBs should be stopped immediately, and, if appropriate, alternative therapy should be started.
Exposure to ARB therapy during the second and third trimesters is known to induce human fetotoxicity (decreased renal function, oligohydramnios, skull ossification retardation) and neonatal toxicity (renal failure, hypotension, hyperkalemia). Should exposure to ARBs have occurred from the second trimester of pregnancy, ultrasound check of renal function and skull is recommended. Infants whose mothers have taken ARBs should be closely observed for hypotension.
Because no information is available regarding the use of telmisartan during breastfeeding, telmisartan is not recommended and alternative treatments with better established safety profiles during breastfeeding are preferable, especially while nursing a newborn or preterm infant. It is unknown whether telmisartan or its metabolites are excreted in human milk.
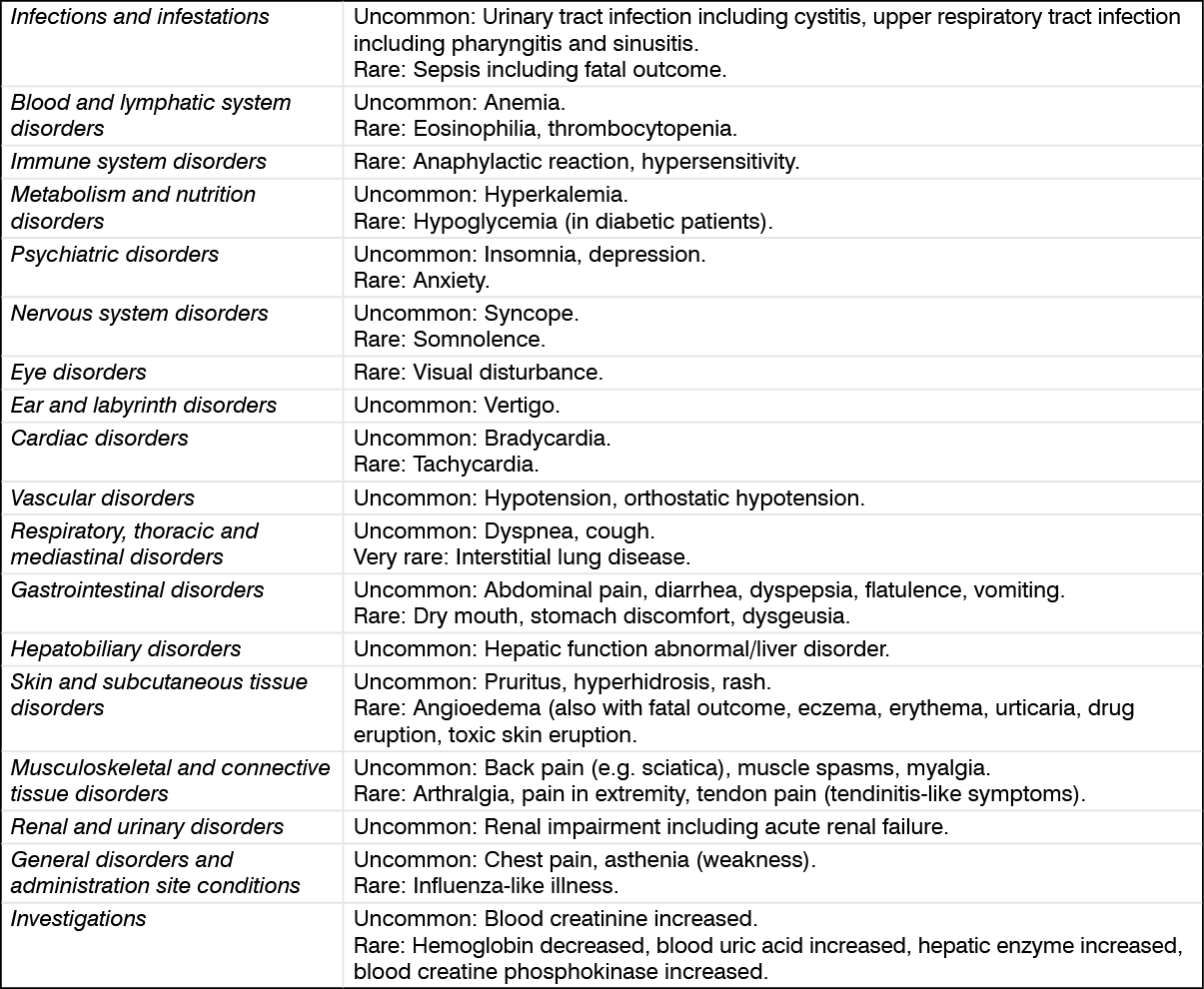
See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Digoxin: When telmisartan was co-administered with digoxin, median increases in digoxin peak plasma concentration (49%) and in trough concentration (20%) were observed. When initiating, adjusting, and discontinuing telmisartan, monitor digoxin levels in order to maintain levels within the therapeutic range.
Potassium-sparing diuretics or potassium supplements: Angiotensin II receptor antagonists such as telmisartan, attenuate diuretic induced potassium loss. Potassium sparing diuretics e.g. spironolactone, eplerenone, triamterene, or amiloride, potassium supplements, or potassium-containing salt substitutes may lead to a significant increase in serum potassium. If concomitant use is indicated because of documented hypokalemia, it should be used with caution and with frequent monitoring of serum potassium.
Lithium: Reversible increases in serum lithium concentrations and toxicity have been reported during concomitant administration of lithium with angiotensin converting enzyme inhibitors, and with angiotensin II receptor antagonists, including telmisartan. If use of the combination proves necessary, careful monitoring of serum lithium levels is recommended.
Non-steroidal anti-inflammatory medicinal products: NSAIDs (i.e. aspirin at anti-inflammatory dosage regimens, COX-2 inhibitors and non-selective NSAIDs) may reduce the antihypertensive effect of angiotensin II receptor antagonists.
Diuretics (thiazide or loop diuretics): Prior treatment with high dose diuretics such as furosemide (loop diuretic) and hydrochlorothiazide (thiazide diuretic) may result in volume depletion, and in a risk of hypotension when initiating therapy with telmisartan.
Other antihypertensive agents: The blood pressure lowering effect of telmisartan can be increased by concomitant use of other antihypertensive medicinal products. Dual blockade of the RAAS through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is associated with a higher frequency of adverse events such as hypotension, hyperkalemia and decreased renal function (including acute renal failure) compared to the use of a single RAAS-acting agent.
Based on their pharmacological properties it can be expected that the following medicinal products may potentiate the hypotensive effects of all antihypertensives including telmisartan: baclofen, amifostine. Furthermore, orthostatic hypotension may be aggravated by alcohol, barbiturates, narcotics, or antidepressants.
Corticosteroids (systemic route): Reduction of the antihypertensive effect.
Store at temperatures not exceeding 30°C.
C09CA07 - telmisartan ; Belongs to the class of angiotensin II receptor blockers (ARBs). Used in the treatment of cardiovascular disease.
Telmigen tab 40 mg
10's;30's
Telmigen tab 80 mg
10's;30's



 Sign Out
Sign Out