


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of action: Golimumab is a human monoclonal antibody that forms high affinity, stable complexes with both the soluble and transmembrane bioactive forms of human TNF-α, which prevents the binding of TNF-α to its receptors.
Pharmacodynamic effects: The binding of human TNF by golimumab was shown to neutralize TNF-α-induced cell-surface expression of the adhesion molecules E-selectin, vascular cell adhesion molecule (VCAM)-1 and intercellular adhesion molecule (ICAM)-1 by human endothelial cells. In vitro, TNF-induced secretion of interleukin (IL)-6, IL-8 and granulocyte-macrophage colony-stimulating factor (GM-CSF) by human endothelial cells was also inhibited by golimumab.
Improvement in C-reactive protein (CRP) levels were observed relative to placebo groups and treatment with Golimumab (Simponi) resulted in significant reductions from baseline in serum levels of IL-6, ICAM-1, matrix-metalloproteinase (MMP)-3 and vascular endothelial growth factor (VEGF) compared to control treatment. In addition, levels of TNF-α were reduced in RA and AS patients and levels of IL-8 were reduced in PsA patients. These changes were observed at the first assessment (week 4) after the initial Golimumab (Simponi) administration and were generally maintained through week 24.
Clinical efficacy: Rheumatoid arthritis: The efficacy of Golimumab (Simponi) was demonstrated in three multi-center, randomized, double-blind, placebo-controlled studies in over 1500 patients ≥18 years of age with moderately to severely active RA, diagnosed according to the American College of Rheumatology (ACR) criteria for at least 3 months prior to screening. Patients had at least 4 swollen and 4 tender joints. Golimumab (Simponi) or placebo were subcutaneously administered every 4 weeks.
GO-FORWARD evaluated 444 patients who had active RA despite a stable dose of at least 15 mg/week of MTX and who had not been previously treated with an anti-TNF agent. Patients were randomized to receive placebo + MTX, Golimumab (Simponi) 50 mg + MTX, Golimumab (Simponi) 100 mg + MTX or Golimumab (Simponi) 100 mg + placebo. Patients receiving placebo + MTX were switched to Golimumab (Simponi) 50 mg + MTX after Week 24. At Week 52, patients entered an open-label long-term extension.
GO-AFTER evaluated 445 patients who were previously treated with one or more of the anti-TNF agents adalimumab, etanercept, or infliximab. Patients were randomized to receive placebo, Golimumab (Simponi) 50 mg, or Golimumab (Simponi) 100 mg. Patients were allowed to continue concomitant DMARD therapy with MTX, sulfasalazine (SSZ), and/or hydroxychloroquine (HCQ) during the study. The stated reasons for discontinuation of prior anti-TNF therapies were lack of efficacy (58%), intolerance (13%), and/or reasons other than safety or efficacy (29%, mostly for financial reasons).
GO-BEFORE evaluated 637 patients with active RA who were MTX-naïve and had not previously been treated with an anti-TNF agents. Patients were randomized to receive placebo + MTX, Golimumab (Simponi) 50 mg + MTX, Golimumab (Simponi) 100 mg + MTX or Golimumab (Simponi) 100 mg + placebo. At week 52, patients entered an open-label, long-term extension in which patients receiving placebo + MTX who had at least 1 tender or swollen joint were switched to Simponi 50 mg + MTX.
In GO-FORWARD, the (co-)primary endpoints were the percentage of patients achieving an ACR 20 response at Week 14 and the improvement from baseline in Health Assessment Questionnaire (HAQ) at Week 24. In GO-AFTER, the primary endpoint was the percentage of patients achieving an ACR 20 response at Week 14. In GO-BEFORE, the co-primary endpoints were the percentage of patients achieving ACR 50 response at Week 24 and the change from baseline in the van der Heijde-modified Sharp (vdH-S) score at Week 52. In addition to the primary endpoint(s), additional assessments of the impact of Golimumab (Simponi) treatment on the signs and symptoms of arthritis, radiographic response, physical function, and health-related quality of life were performed.
In general, no clinically meaningful differences in measures of efficacy were observed between the Golimumab (Simponi) 50 and 100 mg dosing regimens with concomitant MTX, through week 104 in GO-FORWARD and GO-BEFORE and through week 24 in GO-AFTER. In each of the RA studies by study design, patients in the long-term extension may have switched between the 50 mg and 100 mg Golimumab (Simponi) doses at the discretion of the study physician.
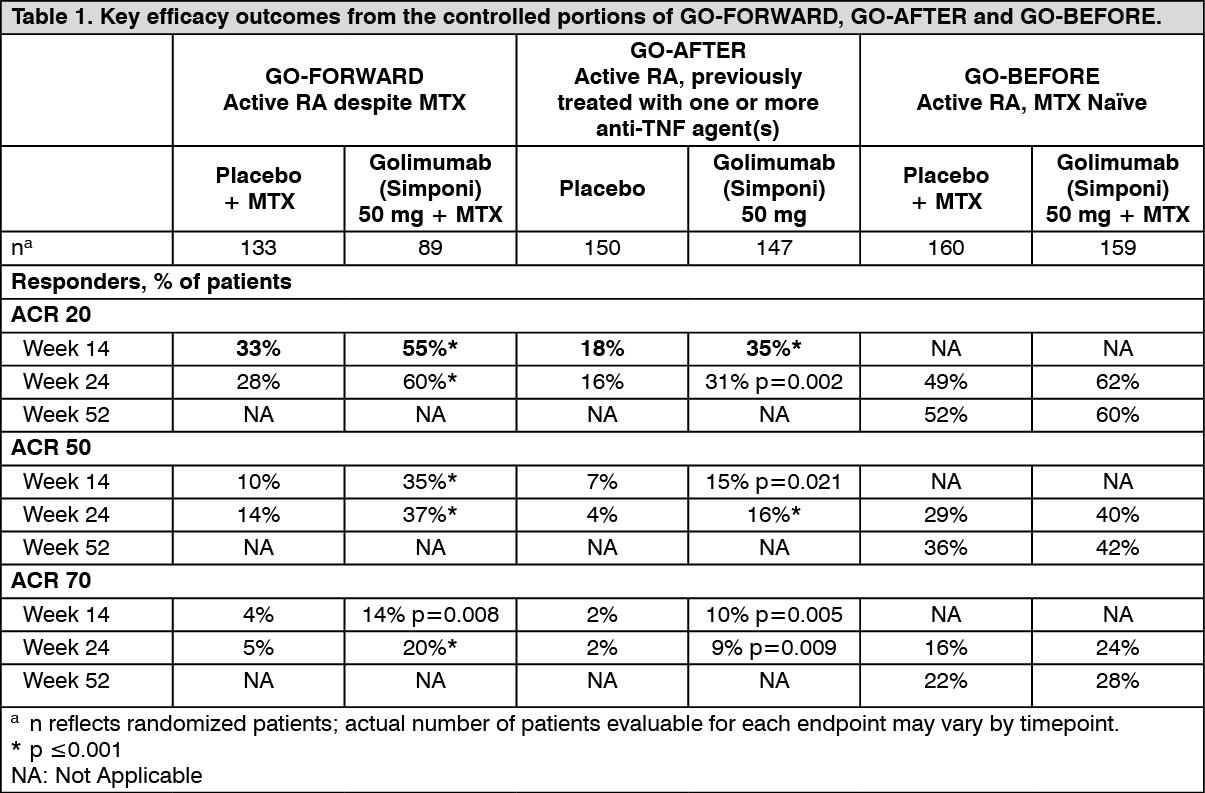
Signs and symptoms: Key ACR results for the Golimumab (Simponi) 50-mg dose at weeks 14, 24, and 52 for GO-FORWARD, GO-AFTER, and GO-BEFORE are shown in Table 1 and are described as follows.
Responses were observed at the first assessment (Week 4) after the initial Golimumab (Simponi) administration.
In GO-FORWARD, among 89 patients randomized to Golimumab (Simponi) 50 mg + MTX, 48 were still on this treatment at week 104. Among those, 40, 33 and 24 patients had ACR 20/50/70 response, respectively at week 104. Among patients remaining in the study and treated with Golimumab (Simponi), similar rates of ACR 20/50/70 response was observed from week 104 through week 256.
In GO-AFTER, the percentage of patients achieving an ACR 20 response was greater for patients receiving Golimumab (Simponi) than for patients receiving placebo regardless of the reason reported for discontinuation of one or more prior anti-TNF therapies. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn GO-BEFORE the primary analysis in patients with moderate to severe rheumatoid arthritis (combined Golimumab (Simponi) 50 mg and 100 mg + MTX groups vs MTX alone for ACR 50) was not statistically significant at week 24 (p=0.053). At week 52 in the overall population, the percentage of patients in the Golimumab (Simponi) 50 mg + MTX group who achieved an ACR response was generally higher but not significantly different when compared with MTX alone (see Table 1). Additional analyses were performed in subsets representative of the indicated population of patients with severe, active and progressive RA. A generally greater effect of Golimumab (Simponi) 50 mg + MTX versus MTX alone was demonstrated in the indicated population compared with the overall population.
In GO‑FORWARD and GO‑AFTER, clinically meaningful and statistically significant responses in Disease Activity Scale (DAS)28 were observed at each prespecified timepoint, at week 14 and at week 24 (p≤0.001). Among patients who remained on the Golimumab (Simponi) treatment to which they were randomized at study start, DAS28 responses were maintained through week 104. Among patients remaining in the study and treated with Golimumab (Simponi), DAS28 responses were similar from week 104 through week 256.
In GO‑BEFORE, major clinical response, defined as the maintenance of an ACR 70 response over a continuous 6‑month period, was measured. At week 52, 15% of patients in the Golimumab (Simponi) 50 mg + MTX group achieved a major clinical response compared with 7% of patients in the placebo + MTX group (p=0.018). Among 159 patients randomized to Golimumab (Simponi) 50 mg + MTX, 96 were still on this treatment at week 104. Among patients remaining in the study and treated with Golimumab (Simponi), similar rates of ACR 20/50/70 response were observed from week 104 through week 256.
Radiographic response: In GO‑BEFORE, the change from baseline in the vdH‑S score, a composite score of structural damage that radiographically measures the number and size of joint erosions and the degree of joint space narrowing in hands/wrists and feet, was used to assess the degree of structural damage. Key results for the Golimumab (Simponi) 50‑mg dose at Week 52 are presented in Table 2.
The number of patients with no new erosions or a change from baseline in total vdH‑S Score ≤ 0 was significantly higher in the Golimumab (Simponi) treatment group than in the control group (p=0.003). The radiographic effects observed at week 52 were maintained through week 104. Among patients remaining in the study and treated with Golimumab (Simponi), radiographic effects were similar from week 104 through week 256. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePhysical function and health‑related quality of life: Physical function and disability were assessed as a separate endpoint in GO‑FORWARD and GO‑AFTER using the disability index of the HAQ DI. In these studies, Golimumab (Simponi) demonstrated clinically meaningful and statistically significant improvement in HAQ DI from baseline versus control at week 24. Among patients who remained on the Golimumab (Simponi) treatment to which they were randomized at study start, improvement in HAQ DI was maintained through week 104. Among patients remaining in the study and treated with Golimumab (Simponi), improvement in HAQ DI was similar from week 104 through week 256.
In GO‑FORWARD clinically meaningful and statistically significant improvements were demonstrated in health‑related quality of life as measured by the physical component score of the SF‑36 in patients treated with Golimumab (Simponi) versus placebo at week 24. Among patients who remained on the Golimumab (Simponi) treatment to which they were randomized at study start, improvement of the SF‑36 physical component was maintained through week 104 through week 256. In GO‑FORWARD and GO‑AFTER, statistically significant improvements were observed in fatigue as measured by functional assessment of chronic illness therapy‑fatigue scale (FACIT‑F).
Psoriatic arthritis: The safety and efficacy of Golimumab (Simponi) were evaluated in a multi‑center, randomized, double‑blind, placebo‑controlled study (GO‑REVEAL) in 405 adult patients with active PsA (≥ 3 swollen joints and ≥ 3 tender joints) despite non‑steroidal anti‑inflammatory (NSAID) or DMARD therapy. Patients in this study had a diagnosis of PsA for at least 6 months and had at least mild psoriatic disease. Patients with each sub‑type of psoriatic arthritis were enrolled, including polyarticular arthritis with no rheumatoid nodules (43%), asymmetric peripheral arthritis (30%), distal interphalangeal (DIP) joint arthritis (15%), spondylitis with peripheral arthritis (11%), and arthritis mutilans (1%). Previous treatment with an anti‑TNF agent was not allowed. Golimumab (Simponi) or placebo were administered subcutaneously every 4 weeks. Patients were randomly assigned to placebo, Golimumab (Simponi) 50 mg, or Golimumab (Simponi) 100 mg. Patients receiving placebo were switched to Golimumab (Simponi) 50 mg after week 24. Patients entered an open-label, long‑term extension at week 52. Approximately forty‑eight percent of patients continued on stable doses of methotrexate (≤ 25 mg/week). The co‑primary endpoints were the percentage of patients achieving ACR 20 response at week 14 and change from baseline in total PsA modified vdH‑S score at week 24.
In general, no clinically meaningful differences in measures of efficacy were observed between the Golimumab (Simponi) 50 mg and 100 mg dosing regimens through week 104. By study design, patients in the long‑term extension may have switched between the 50 mg and 100 mg Golimumab (Simponi) doses at the discretion of the study physician.
Signs and symptoms: Key results for the 50 mg dose at weeks 14 and 24 are shown in Table 3 and described as follows. (See Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageResponses were observed at the first assessment (Week 4) after the initial Golimumab (Simponi) administration. Similar ACR 20 responses at Week 14 were observed in patients with polyarticular arthritis with no rheumatoid nodules and asymmetric peripheral arthritis PsA subtypes. The number of patients with other PsA subtypes was too small to allow meaningful assessment. Responses observed in the Golimumab (Simponi)‑treated groups were similar in patients receiving and not receiving concomitant MTX. Among 146 patients randomized to Golimumab (Simponi) 50 mg, 70 were still on this treatment at week 104. Of these 70 patients, 64, 46, and 31 patients had an ACR 20/50/70 response, respectively. Among patients remaining in the study and treated with Golimumab (Simponi), similar rates of ACR 20/50/70 response was observed from week 104 through week 256.
Statistically significant responses in DAS28 were also observed at weeks 14 and 24 (p<0.05).
At week 24 improvements in parameters of peripheral activity characteristic of psoriatic arthritis (e.g. number of swollen joints, number of painful/tender joints, dactylitis and enthesitis) were seen in the Golimumab (Simponi)‑treated patients. Golimumab (Simponi) treatment resulted in significant improvement in physical function as assessed by HAQ DI, as well as significant improvements in health‑related quality of life as measured by the physical and mental component summary scores of the SF‑36. Among patients who remained on the Golimumab (Simponi) treatment to which they were randomized at study start, DAS28 and HAQ DI responses were maintained through week 104. Among patients remaining in the study and treated with Golimumab (Simponi), DAS28 and HAQ DI responses were similar from week 104 through week 256.
Radiographic response: Structural damage in both hands and feet was assessed radiographically by the change from baseline in the vdH‑S score, modified for PsA by addition of hand distal interphalangeal (DIP) joints.
Golimumab (Simponi) 50‑mg treatment reduced the rate of progression of peripheral joint damage compared with placebo treatment at week 24 as measured by change from baseline in total modified vdH‑S Score (mean ± SD score was 0.27 ± 1.3 in the placebo group compared with ‑0.16 ±1.3 in the Golimumab (Simponi) group; p=0.011). Out of 146 patients who were randomized to Golimumab (Simponi) 50 mg, 52‑week X‑ray data were available for 126 patients, of whom 77% showed no progression compared to baseline. At week 104, X‑ray data were available for 114 patients, and 77% showed no progression from baseline. Among patients remaining in the study and treated with Golimumab (Simponi), similar rates of patients showed no progression from baseline from week 104 through week 256.
Axial spondyloarthritis: Ankylosing spondylitis: The safety and efficacy of Golimumab (Simponi) were evaluated in a multi‑center, randomized, double‑blind, placebo‑controlled study (GO‑RAISE) in 356 adult patients with active ankylosing spondylitis (defined as a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥ 4 and a VAS for total back pain of ≥ 4, on a scale of 0 to 10 cm). Patients enrolled in this study had active disease despite current or previous NSAID or DMARD therapy and had not previously been treated with anti‑TNF therapy. Golimumab (Simponi) or placebo were administered subcutaneously every 4 weeks. Patients were randomly assigned to placebo, Golimumab (Simponi) 50 mg, and Golimumab (Simponi) 100 mg and were allowed to continue concomitant DMARD therapy (MTX, SSZ, and/or HCQ). The primary endpoint was the percentage of patients achieving Ankylosing Spondylitis Assessment Study Group (ASAS) 20 response at week 14. Placebo‑controlled efficacy data were collected and analyzed through week 24.
Key results for the 50 mg dose are shown in Table 4 and described as follows. In general, no clinically meaningful differences in measures of efficacy were observed between the Golimumab (Simponi) 50 mg and 100 mg dosing regimens through week 24. By study design, patients in the long-term extension may have switched between the 50 mg and 100 mg Golimumab (Simponi) doses at the discretion of the study physician. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAmong patients remaining in the study and treated with Golimumab (Simponi), the proportion of patients with an ASAS 20 and ASAS 40 response were similar from week 24 through week 256.
Statistically significant responses in BASDAI 50, 70 and 90 (p≤0.017) were also seen at weeks 14 and 24. Improvements in key measures of disease activity were observed at the first assessment (week 4) after the initial Golimumab (Simponi) administration and were maintained through week 24. Among patients remaining in the study and treated with Golimumab (Simponi), similar rates of change from baseline in BASDAI were observed from week 24 through week 256. Consistent efficacy was seen in patients regardless of use of DMARDs (MTX, sulfasalazine, and/or hydroxychloroquine), HLA‑B27 antigen status, or baseline CRP levels as assessed by ASAS 20 responses at week 14.
Golimumab (Simponi) treatment resulted in significant improvements in physical function as assessed by changes from baseline in BASFI at weeks 14, 24. Health‑related quality of life as measured by the physical component score of the SF‑36 was also improved significantly at weeks 14 and 24. Among patients remaining in the study and treated with Golimumab (Simponi), improvements in physical function and health‑related quality of life were similar from week 24 through week 256.
Non-radiographic axial spondyloarthritis: The safety and efficacy of Golimumab (Simponi) were evaluated in a multi‑centre, randomised, double‑blind, placebo‑controlled study (GO‑AHEAD) in 197 adult patients with severe active nr‑Axial SpA (defined as those patients meeting the ASAS classification criteria of axial spondyloarthritis but did not meet the modified New York criteria for AS). Patients enrolled in this study had active disease (defined as a BASDAI ≥ 4 and a Visual Analogue Scale (VAS) for total back pain of ≥ 4, each on a scale of 0‑10 cm) despite current or previous NSAID therapy and had not previously been treated with any biological agents including anti‑TNF therapy. Patients were randomly assigned to placebo or Golimumab (Simponi) 50 mg administered subcutaneously every 4 weeks. At week 16, patients entered an open label period in which all patients received Golimumab (Simponi) 50 mg administered subcutaneously every 4 weeks through week 48 with efficacy assessments performed through week 52 and safety follow-up through week 60. Approximately 93% of patients who were receiving Golimumab (Simponi) at the beginning of the open-label extension (week 16) remained on treatment through the end of the study (week 52). Analyses were performed on both the All Treated (AT, N = 197) and Objective Signs of Inflammation (OSI, N = 158, defined by elevated CRP and/or evidence of sacroiliitis on MRI at baseline) populations. Placebo‑controlled efficacy data were collected and analyzed through week 16. The primary endpoint was the proportion of patients achieving ASAS 20 response at week 16. Key results are shown in Table 5 and described as follows.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStatistically significant improvements in signs and symptoms of severe active nr‑Axial SpA were demonstrated in patients treated with Golimumab (Simponi) 50 mg compared to placebo at week 16 (Table 5). Improvements were observed at the first assessment (week 4) after the initial Golimumab (Simponi) administration. SPARCC score as measured by MRI showed statistically significant reductions in SI joint inflammation at week 16 in patients treated with Golimumab (Simponi) 50 mg compared to placebo (Table 5). Pain as assessed by the Total Back Pain and Nocturnal Back Pain VAS, and disease activity as measured by ASDAS‑C also showed statistically significant improvement from baseline to week 16 in patients treated with Golimumab (Simponi) 50 mg compared to placebo (p < 0.0001).
Statistically significant improvements in spinal mobility as assessed by BASMI (Bath Ankylosing Spondylitis Metrology Index) and in physical function as assessed by the BASFI were demonstrated in Golimumab (Simponi) 50 mg‑treated patients as compared to placebo‑treated patients (p < 0.0001). Patients treated with Golimumab (Simponi) experienced significantly more improvements in health‑related quality of life as assessed by ASQoL, EQ‑5D, and physical and mental components of SF‑36, and experienced significantly more improvements in productivity as assessed by greater reductions in overall work impairment and in activity impairment as assessed by the WPAI questionnaire than patients receiving placebo.
For all of the endpoints described as previously mentioned, statistically significant results were also demonstrated in the OSI population at week 16.
In both the AT and OSI populations, the improvements in signs and symptoms, spinal mobility, physical function, quality of life, and productivity observed at week 16 among patients treated with Golimumab (Simponi) 50 mg continued in those remaining in the study at week 52.
Ulcerative colitis: The efficacy of Golimumab (Simponi) was evaluated in two randomized, double‑blind, placebo‑controlled clinical studies in adult patients.
The induction study (PURSUIT‑Induction) evaluated patients with moderately to severely active ulcerative colitis (Mayo score 6 to 12; Endoscopy subscore ≥ 2) who had an inadequate response to or failed to tolerate conventional therapies, or were corticosteroid dependent. In the dose confirming portion of the study, efficacy was evaluated in 761 patients who were randomized to receive either 400 mg Golimumab (Simponi) SC at week 0 and 200 mg at week 2, 200 mg Golimumab (Simponi) SC at week 0 and 100 mg at week 2, or placebo SC at weeks 0 and 2. Concomitant stable doses of oral aminosalicylates, corticosteroids, and/or immunomodulatory agents were permitted. The efficacy of Golimumab (Simponi) through week 6 was assessed in this study.
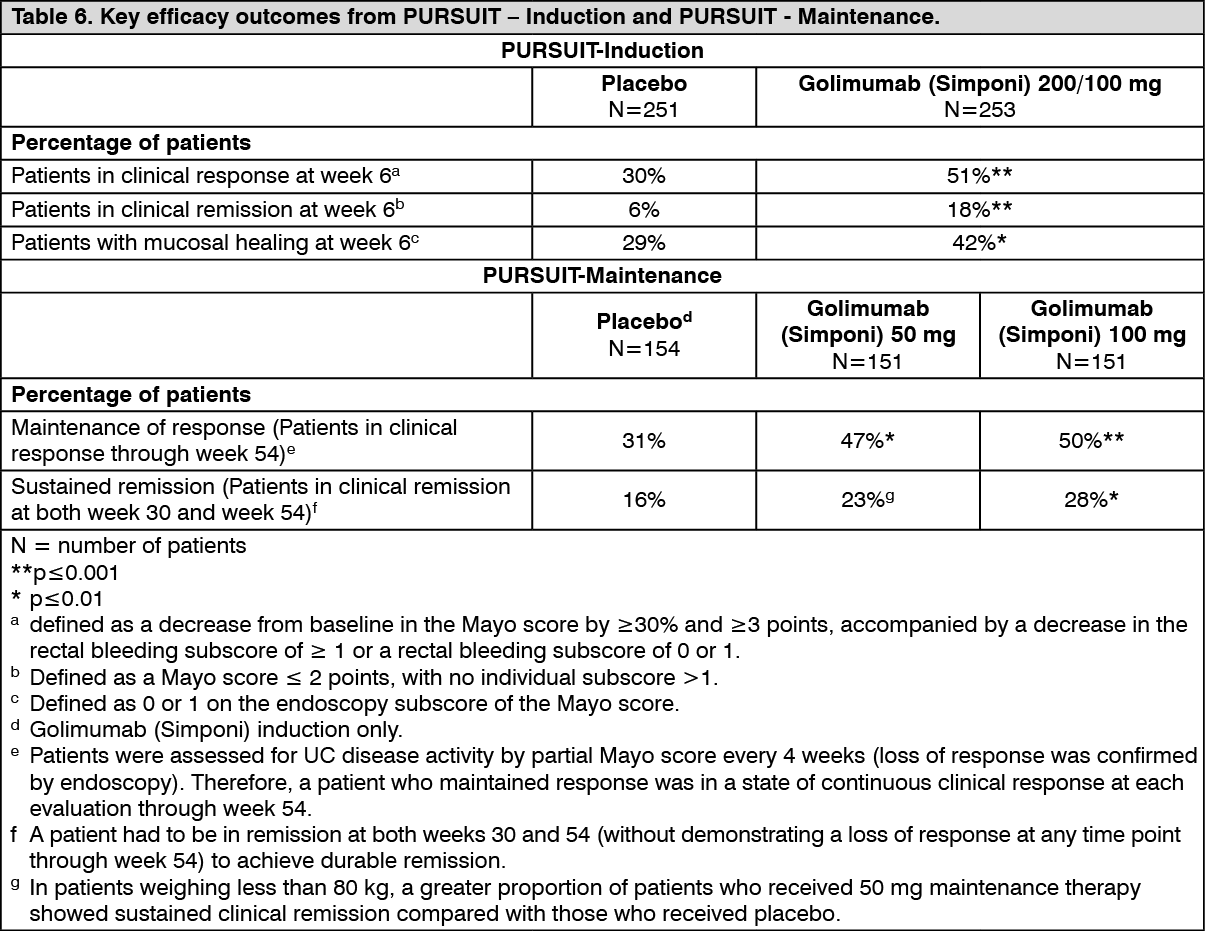
The results of the maintenance study (PURSUIT‑Maintenance) were based on evaluation of 456 patients who achieved clinical response from previous induction with Golimumab (Simponi). Patients were randomized to receive Golimumab (Simponi) 50 mg, Golimumab (Simponi) 100 mg, or placebo administered subcutaneously every 4 weeks. Concomitant stable doses of oral aminosalicylates, and/or immunomodulatory agents were permitted. Corticosteroids were to be tapered at the start of the maintenance study. The efficacy of Golimumab (Simponi) through week 54 was assessed in this study. Patients who completed the maintenance study through week 54 continued treatment in a study extension, with efficacy evaluated through week 216. Efficacy evaluation in the study extension was based on changes in corticosteroid use, Physician's Global Assessment (PGA) of disease activity, and improvement in quality of life as measured by Inflammatory Bowel Disease Questionnaire (IBDQ). (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMore Golimumab (Simponi)‑treated patients demonstrated sustained mucosal healing (patients with mucosal healing at both week 30 and week 54) in the 50‑mg group (42%, nominal p<0.05) and 100‑mg group (42%, p<0.005) compared with patients in the placebo group (27%).
Among the 54% of patients (247/456) who were receiving concomitant corticosteroids at the start of PURSUIT‑Maintenance, the proportion of patients who maintained clinical response through week 54 and were not receiving concomitant corticosteroids at week 54 was greater in the 50 mg group (38%, 30/78) and 100‑mg group (30%, 25/82) compared with the placebo group (21%, 18/87). The proportion of patients who eliminated corticosteroids by Week 54 was greater in the 50‑mg group (41%, 32/78) and 100‑mg group (33%, 27/82) compared with the placebo group (22%, 19/87). Among patients who entered the study extension, the proportion of subjects who remained corticosteroid-free was generally maintained through week 216.
Patients who did not achieve clinical response at week 6 in the PURSUIT-Induction studies were dosed Golimumab (Simponi) 100 mg every 4 weeks in the PURSUIT-Maintenance study. At week 14, 28% of these patients achieved response defined by partial Mayo score (decreased by ≥ 3 points compared with start of induction). At week 54, the clinical outcomes observed in these patients were similar to the clinical outcomes reported for the patients achieving clinical response at week 6.
At week 6, Golimumab (Simponi) significantly improved quality of life as measured by change from baseline in a disease specific measure, IBDQ (inflammatory bowel disease questionnaire). Among patients who received Golimumab (Simponi) maintenance treatment, the improvement in quality of life as measured by IBDQ was maintained through week 54.
Approximately 63% of patients, who were receiving Golimumab (Simponi) at the beginning of the study extension (week 56), remained on treatment through the end of the study (last golimumab administration at week 212).
Immunogenicity: Across the Phase III RA, PsA and AS studies through week 52, antibodies to golimumab were detected by the enzyme immunoassay (EIA) method in 5% (105/2062) of golimumab treated patients and, where tested, nearly all antibodies were neutralising in vitro. Similar rates were shown across rheumatologic indications. Treatment with concomitant MTX resulted in a lower proportion of patients with antibodies to golimumab than patients receiving golimumab without MTX (approximately 3% [41/1235] versus 8% [64/827], respectively).
In nr‑Axial SpA, antibodies to golimumab were detected in 7% (14/193) of golimumab treated patients through week 52 by the EIA method.
In the Phase II and III UC studies through week 54, antibodies to golimumab were detected by the EIA method in 3% (26/946) of golimumab treated patients. Sixty-eight percent (21/31) of antibody‑positive patients had neutralising antibodies in vitro. Treatment with concomitant immunomodulators (azathioprine, 6‑mercaptopurine and MTX) resulted in a lower proportion of patients with antibodies to golimumab than patients receiving golimumab without immunomodulators (1% (4/308) versus 3% (22/638), respectively). Of patients that continued in the study extension and had evaluable samples through week 228, antibodies to golimumab were detected in 4% (23/604) of golimumab treated patients. Eighty-two percent (18/22) of antibody-positive patients had neutralizing antibodies in vitro.
A drug‑tolerant EIA method was used in the pJIA study for the detection of antibodies to golimumab. Due to the higher sensitivity and the improved drug tolerance, a higher incidence of antibodies to golimumab was expected to be detected with the drug‑tolerant EIA method compared to the EIA method. In the Phase III pJIA study through week 48, antibodies to golimumab were detected by the drug‑tolerant EIA method in 40% (69/172) of golimumab treated children of which a majority had a titre lower than 1:1000. An effect on serum golimumab concentrations was seen at titres of > 1:100 while an effect on efficacy was not seen until titres of > 1:1000, though the numbers of children with titres of > 1:1000 were low (N = 8). Among the children who tested positive for antibodies to golimumab, 39% (25/65) had neutralising antibodies. The higher incidence of antibodies with the drug‑tolerant EIA method, because they were mainly low titre antibodies, did not have an apparent impact on drug levels, efficacy and safety and therefore does not represent any new safety signal.
The presence of antibodies to golimumab may increase the risk of injection site reactions. The small number of patients positive for antibodies to golimumab limits the ability to draw definitive conclusions regarding the relationship between antibodies to golimumab and clinical efficacy or safety measures.
Because immunogenicity analyses are product‑ and assay‑specific, comparison of antibody rates with those from other products is not appropriate.
Pediatric population: Polyarticular juvenile idiopathic arthritis: The safety and efficacy of Golimumab (Simponi) was evaluated in a randomised, double-blind, placebo‑controlled, withdrawal study (GO-KIDS) in 173 children (2 to 17 years of age) with active pJIA with at least 5 active joints and an inadequate response to MTX. Children with polyarticular course JIA (rheumatoid factor positive or negative polyarthritis, extended oligoarthritis, juvenile psoriatic arthritis or systemic JIA with no current systemic symptoms) were included in the study. The baseline median number of active joints was 12, and median CRP was 0.17 mg/dL.
Part 1 of the study consisted of a 16‑week open/autoinjector (SmartJect)‑label phase in which 173 enrolled children received Golimumab (Simponi) 30 mg/m2 (maximum 50 mg) subcutaneously every 4 weeks and MTX. The 154 children who achieved an ACR Ped 30 response at week 16 entered Part 2 of the study, the randomised withdrawal phase, and received Golimumab (Simponi) 30 mg/m2 (maximum 50 mg) + MTX or placebo + MTX every 4 weeks. After disease flare, children received Golimumab (Simponi) 30 mg/m2 (maximum 50 mg) + MTX. At week 48, children entered a long‑term extension.
Children in this study demonstrated ACR Ped 30, 50, 70, and 90 responses as early as week 4.
At week 16, 87% of children were ACR Ped 30 responders, and 79%, 66%, and 36% of children were ACR Ped 50, ACR Ped 70, and ACR Ped 90 responders, respectively. At week 16, 34% of children had inactive disease defined as having the presence of all of the following: no joints with active arthritis; no fever, rash, serositis, splenomegaly, hepatomegaly, or generalised lymphadenopathy attributable to JIA; no active uveitis; normal ESR (< 20 mm/hour) or CRP (< 1.0 mg/dL); physician global assessment of disease activity (≤ 5 mm on the VAS); duration of morning stiffness < 15 minutes.
At week 16, all ACR Ped components demonstrated clinically relevant improvement from baseline (see Table 7).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe primary endpoint, the proportion of children who were ACR Ped 30 responders at week 16 and who did not experience a flare between week 16 and week 48, was not achieved. The majority of children did not experience a flare between week 16 and week 48 (59% in the Golimumab (Simponi) + MTX and 53% in the placebo + MTX groups, respectively; p = 0.41).
Pre-specified subgroup analyses of the primary endpoint by baseline CRP (≥ 1 mg/dL vs < 1 mg/dL) demonstrated higher flare rates in placebo + MTX vs Golimumab (Simponi) + MTX treated subjects among subjects with baseline CRP ≥ 1 mg/dL (87% vs 40% p = 0.0068).
At week 48, 53% and 55% of children in the Golimumab (Simponi) + MTX group and placebo + MTX group, respectively, were ACR Ped 30 responders, and 40% and 28% of children in the Golimumab (Simponi) + MTX group and placebo + MTX group, respectively, achieved inactive disease.
Pharmacokinetics: Absorption: Following a single subcutaneous administration of golimumab to healthy subjects or patients with RA, the time to reach maximum serum concentrations (Tmax) ranged from 2 to 6 days. A subcutaneous injection of 50 mg golimumab to healthy subjects produced a mean ± standard deviation maximum serum concentration (Cmax) of 3.2 ± 1.4 μg/mL.
Following a single subcutaneous injection of 100 mg, the absorption of golimumab was similar in the upper arm, abdomen, and thigh, with a mean absolute bioavailability of 51%. Since golimumab exhibited approximately dose proportional PK following a SC administration, the absolute bioavailability of a golimumab 50 mg or 200 mg dose is expected to be similar.
Distribution: Following a single IV administration, the mean volume of distribution was 115 ± 19 mL/kg.
Elimination: The systemic clearance of golimumab was estimated to be 6.9 ± 2.0 mL/day/kg. Terminal half‑life value was estimated to be approximately 12 ± 3 days in healthy subjects and similar values were observed in patients with RA, PsA, AS, or UC.
When 50 mg Golimumab (Simponi) was administered subcutaneously to patients with RA, PsA, or AS every 4 weeks, serum concentrations reached steady state by week 12. With concomitant use of MTX, treatment with 50 mg golimumab subcutaneous every 4 weeks resulted in a mean (± standard deviation) steady‑state trough serum concentration of approximately 0.6 ± 0.4 mg/mL in RA patients with active RA despite MTX therapy, and approximately 0.5 ± 0.4 mg/mL in patients with active PsA and approximately 0.8 ± 0.4 mcg/mL in patients with AS. Steady‑state mean trough serum golimumab concentrations in patients with nr‑Axial SpA were similar to those observed in patients with AS following subcutaneous administration of 50 mg golimumab every 4 weeks.
Patients with RA, PsA, or AS who did not receive concomitant MTX had approximately 30% lower steady‑state trough concentrations of golimumab than those who received golimumab with MTX. In a limited number of RA patients treated with subcutaneous golimumab over a 6‑month period, concomitant use of MTX reduced the apparent clearance of golimumab by approximately 36%. However, population pharmacokinetic analysis indicated that concomitant use of NSAIDs, oral corticosteroids or sulfasalazine did not influence the apparent clearance of golimumab.
Following induction doses of 200 mg and 100 mg golimumab at week 0 and week 2, respectively, and maintenance doses of 50 mg or 100 mg Golimumab (Simponi) subcutaneously every 4 weeks thereafter to patients with UC, serum golimumab concentrations reached steady state approximately 14 weeks after the start of therapy. Treatment with 50 mg or 100 mg golimumab subcutaneous every 4 weeks during maintenance resulted in a mean steady‑state trough serum concentration of approximately 0.9 ± 0.5 μg/mL and 1.8 ± 1.1 μg/mL, respectively.
In UC patients treated with 50 mg or 100 mg golimumab subcutaneously every 4 weeks, concomitant use of immunomodulators did not have a substantial effect on steady‑state trough levels of golimumab.
Patients who developed anti‑golimumab antibodies generally had low trough steady‑state serum concentrations of golimumab (see Pharmacology: Pharmacodynamics as previously mentioned).
Linearity: Golimumab exhibited approximately dose‑proportional pharmacokinetics in patients with RA over the dose range of 0.1 to 10.0 mg/kg following a single intravenous dose. Following a single SC dose in healthy subjects, approximately dose‑proportional pharmacokinetics were also observed over a dose range of 50 mg to 400 mg.
Effect of weight on pharmacokinetics: There was a trend toward higher apparent clearance of golimumab with increasing weight (see Dosage & Administration).
Pediatric population: The pharmacokinetics of golimumab were determined in 173 children with pJIA with an age range from 2 to 17 years of age. In the pJIA study, children who received golimumab 30 mg/m2 (maximum 50 mg) subcutaneously every 4 weeks, had median steady‑state trough golimumab concentrations which were similar across different age groups, and which were also similar to or slightly higher than those seen in adult RA patients who received 50 mg golimumab every 4 weeks.
Population pharmacokinetic/pharmacodynamic modeling and simulation in children with pJIA confirmed the relationship between golimumab serum exposures and clinical efficacy and supports that the dosing regimen of golimumab 50 mg every 4 weeks in children with pJIA of at least 40 kg achieves similar exposures to those shown to be efficacious in adults.
Toxicology: Pre-clinical safety data: Non‑clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, toxicity to reproduction and development.
No mutagenicity studies, animal fertility studies nor long‑term carcinogenic studies have been conducted with golimumab.
In a fertility and general reproductive function study in mouse, using an analogous antibody that selectively inhibits the functional activity of mouse TNFα, the number of pregnant mice was reduced. It is not known whether this finding was due to effects on the males and/or the females. In a developmental toxicity study conducted in mice following administration of the same analogous antibody, and in cynomolgus monkeys using golimumab, there was no indication of maternal toxicity, embryotoxicity or teratogenicity.