


 Sign Out
Sign Out

The most common adverse reactions were diarrhea, rash, alopecia and hand-foot skin syndrome (corresponds to palmar-plantar erythrodysesthesia syndrome in MedDRA).
Adverse reactions reported in multiple clinical trials or through post-marketing use are listed in Tables 3 and 4, by system organ class (in MedDRA) and frequency. Frequencies are defined as: Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10,000 to <1/1000), not known (cannot be estimated from the data available).
Within each frequency grouping, adverse effects are presented in order of decreasing seriousness. (See Tables 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image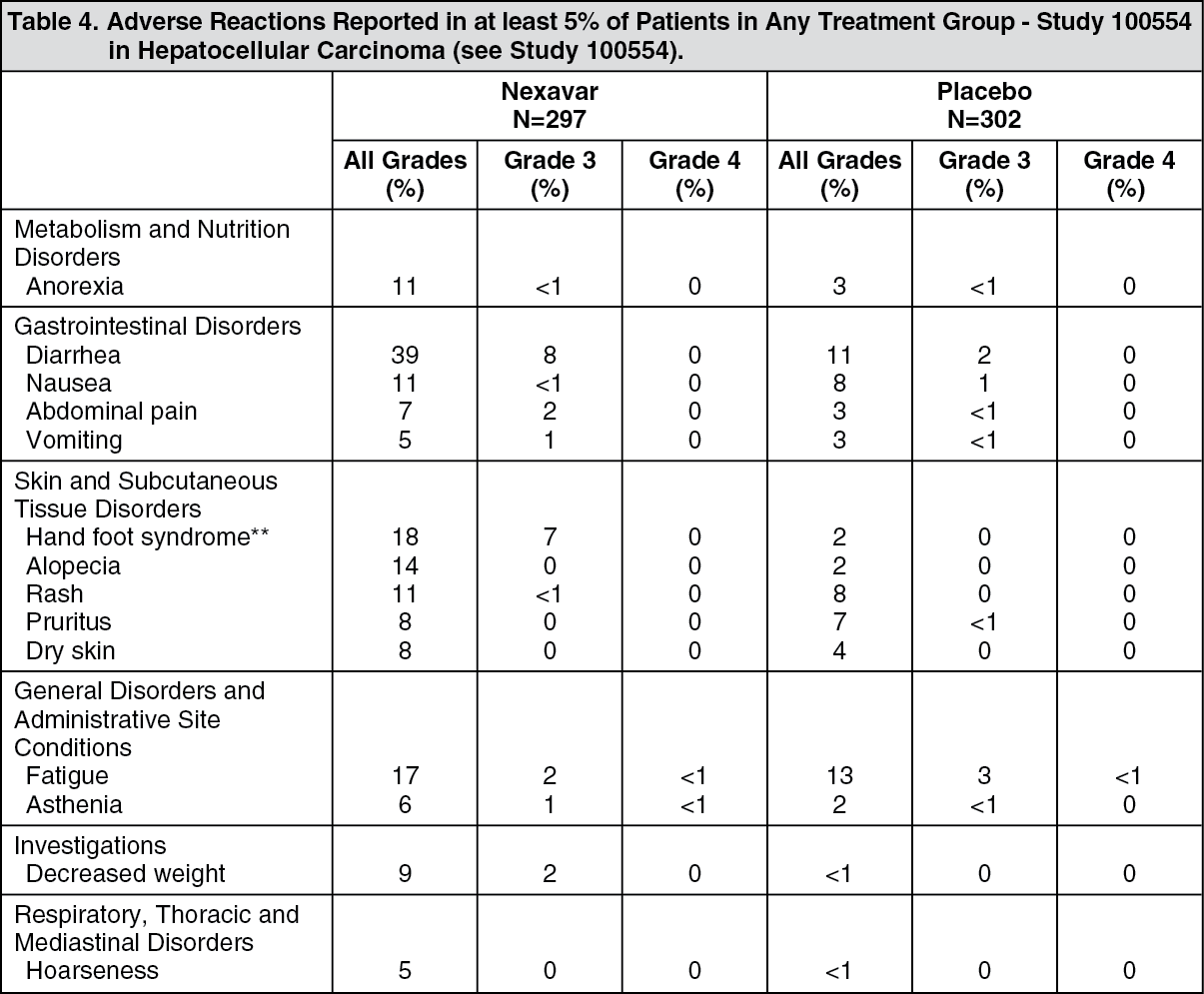 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePalmar-plantar erythrodysesthesia syndrome in MedDRA.
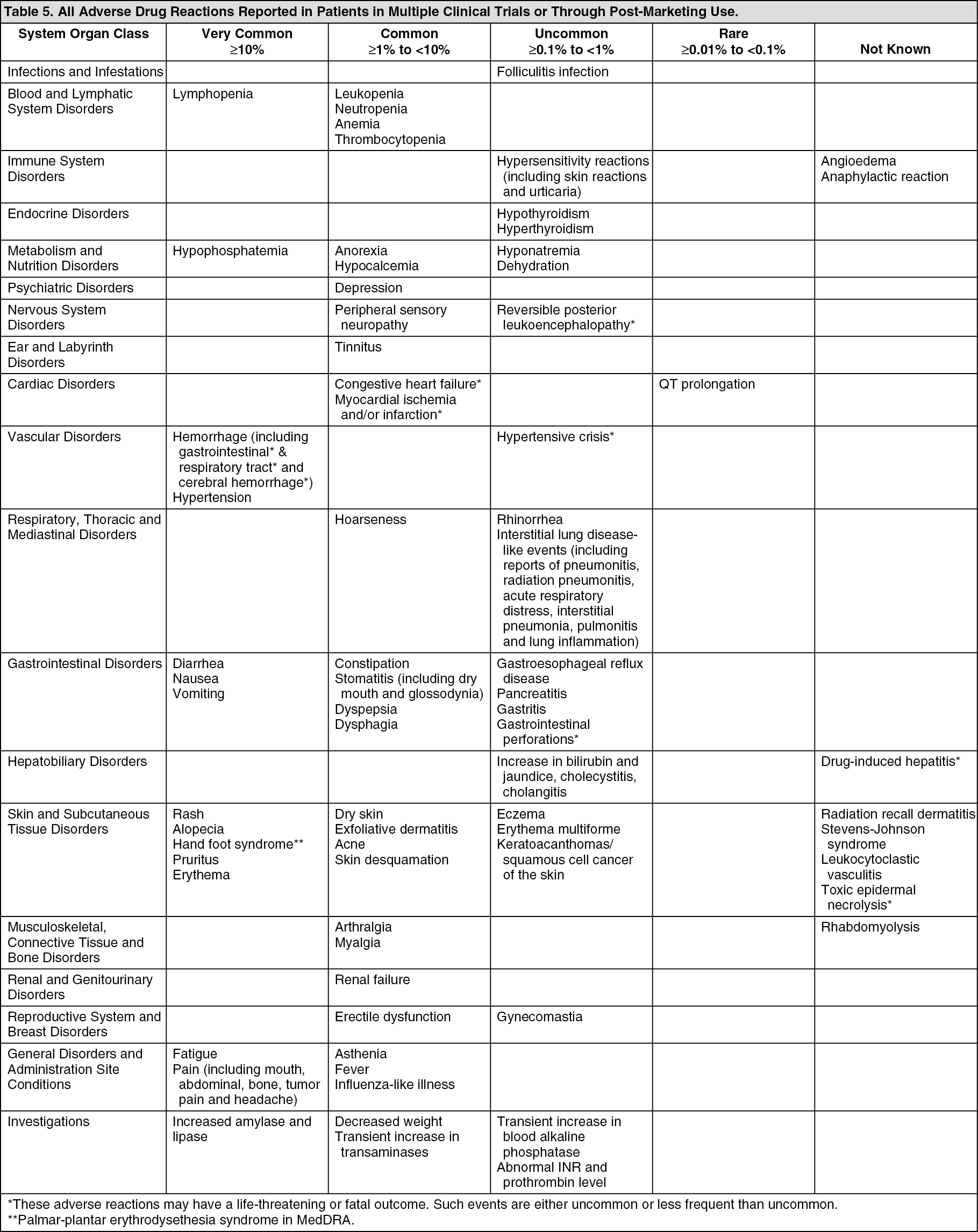
Adverse reactions that occurred either during clinical studies or have been identified through post-marketing use are listed in Table 5, by system organ class (in MedDRA) and frequency. Frequencies are defined as: Very common (≥1/10), common (≥1/100, <1/10), uncommon (≥1/1000, <1/100), rare (≥1/10,000, <1/1000), not known (cannot be estimated from the data available).
Within each frequency grouping, adverse effects are presented in order of decreasing seriousness. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCongestive Heart Failure: In company sponsored clinical trials, congestive heart failure was reported as an adverse event in 1.9% of patients treated with sorafenib (N=2276). In Study 11213 (RCC) adverse events consistent with congestive heart failure were reported 1.7% of those treated with sorafenib and 0.7% receiving placebo. In Study 100554 (HCC), 0.99% of those treated with sorafenib and in 1.1% receiving placebo were reported with these events.
Special Populations: Two randomized placebo-controlled trials comparing safety and efficacy of sorafenib in combination with doublet platinum-based chemotherapies (carboplatin/paclitaxel and separately gemcitabine/cisplatin) versus the respective doublet platinum-based chemotherapies alone as 1st line treatment for patients with advanced non-small cell lung cancer (NSCLC) did not meet their primary endpoint of improved overall survival. Safety events were generally consistent with those previously reported. However, in both trials, higher mortality was observed in the subset of patients with squamous cell carcinoma of the lung treated with sorafenib and doublet platinum-based chemotherapies versus those treated with doublet platinum-based chemotherapies alone (Paclitaxel/Carboplatin: HR 1.81, 95% CI 1.19-2.74; Gemcitabine/Cisplatin: HR 1.22, 95% CI 0.82-1.8). No definitive cause was identified for the findings.
Safety was also assessed in a phase 2 study pool comprised of 638 sorafenib-treated patients, including 202 patients with RCC, 137 patients with hepatocellular carcinoma, and 299 patients with other cancers. The most common drug-related adverse events reported in sorafenib-treated patients in this pool were rash (38%), diarrhea (37%), hand-foot skin reaction (35%), and fatigue (33%). The respective rates of CTC (v 2.0) grade 3 and 4 drug-related adverse events in sorafenib-treated patients were 37% and 3%, respectively.
Laboratory Test Abnormalities in RCC Patients (Study 11213): Elevated lipase and amylase levels were very commonly reported. In Study 11213, Common Terminology Criteria for Adverse Events (CTCAE) grade 3 or 4 lipase elevations occurred in 12% of patients in the sorafenib group compared to 7% of patients in the placebo group. CTCAE grade 3 or 4 amylase elevations were reported in 1% of patients in the sorafenib group compared to 3% of patients in the placebo group. Clinical pancreatitis was reported in 2/451 sorafenib-treated patients (CTCAE grade 4) and 1/451 patients (CTCAE grade 2) in the placebo group in Study 1.
Hypophosphatemia was a common laboratory finding, observed in 45% of sorafenib treated patients compared to 11% of placebo patients. CTCAE grade 3 hypophosphatemia (1-2 mg/dL) occurred in 13% on sorafenib treated patients and 3% of patients in the placebo group. There were no cases of CTCAE grade 4 hypophosphatemia (<1 mg/dL) reported in either sorafenib or placebo patients. The etiology of hypophosphatemia associated with sorafenib is not known.
CTCAE grade 3 or 4 were reported for lymphopenia in 13% of sorafenib treated patients and 7% of placebo patients, for neutropenia in 5% of sorafenib treated patients and 2% of placebo patients, for anemia in 2% of sorafenib treated patients and 4% of placebo patients and for thrombocytopenia in 1% of sorafenib treated patients and 0% of placebo patients.
Hypocalcemia was reported in 12% of sorafenib treated patients compared to 7.5% of placebo patients. Most reports of hypocalcemia were low grade (CTCAE grade 1 and 2). CTCAE grade 3 hypocalcemia (6-7 mg/dL) occurred in 1.1% of sorafenib treated patients and 0.2% of patients in the placebo group, and CTCAE grade 4 hypocalcemia (<6 mg/dL) occurred in 1.1% of sorafenib treated patients and 0.5% of patients in the placebo group. The etiology of hypocalcemia associated with sorafenib is not known.
Laboratory Test Abnormalities in HCC Patients (Study 100554): Elevated lipase was observed in 40% of patients treated with Nexavar compared to 37% of patients in the placebo group. CTCAE grade 3 or 4 lipase elevations occurred in 9% of patients in each group. Elevated amylase was observed in 34% of patients treated with Nexavar compared to 29% of patients in the placebo group. CTCAE grade 3 or 4 amylase elevations were reported in 2% of patients in each group. Many of the lipase and amylase elevations were transient, and in the majority of cases, Nexavar treatment was not interrupted. Clinical pancreatitis was reported in 1 of 297 Nexavar-treated patients (CTCAE grade 2).
Hypophosphatemia was a common laboratory finding, observed in 35% of Nexavar-treated patients compared to 11% of placebo patients; CTCAE grade 3 hypophosphatemia (1-2 mg/dL) occurred in 11% of Nexavar-treated patients and 2% of patients in the placebo group; there was 1 case of CTCAE grade 4 hypophosphatemia (<1 mg/dL) reported in the placebo group. The etiology of hypophosphatemia associated with Nexavar is not known.
Elevations in liver function tests were comparable between the 2 arms of the study. Elevated AST was observed in 94% of Nexavar-treated patients and 91% of placebo patients; CTCAE grade 3 or 4 AST elevations were reported in 16% of Nexavar-treated patients and 17% of patients in the placebo group. ALT elevations were observed in 69% of Nexavar-treated patients and 68% of placebo patients; CTCAE grade 3 or 4 ALT elevations were reported in 3% of Nexavar-treated patients and 8% of placebo treated patients. Elevated bilirubin was observed in 47% of Nexavar-treated patients and 45% of placebo patients; CTCAE grade 3 or 4 bilirubin elevations were reported in 10% of Nexavar-treated patients and 11% of placebo treated patients. Hypoalbuminemia was observed in 59% of Nexavar-treated patients and 47% of placebo patients; no CTCAE grade 3 or 4 hypoalbuminemia was observed in either group.
Alkaline phosphatase elevations were observed in 82.2% of Nexavar-treated patients and 82.5% of placebo patients; CTCAE grade 3 alkaline phosphatase elevations were reported in 6.2% of Nexavar-treated patients and 8.2% of placebo treated patients; no CTCAE grade 4 alkaline phosphatase elevation was observed in either group.
International normalized ratio elevations were observed in 42% of Nexavar-treated patients and 34% of placebo patients; CTCAE grade 3 INR elevations were reported in 4% of Nexavar-treated patients and 2% of placebo patients; there was no CTCAE grade 4 INR elevation in either group.
Lymphopenia was observed in 47% of Nexavar-treated patients and 42% of placebo patients; CTCAE grade 3 or 4 lymphopenia was reported in 6% of patients in each group. Neutropenia was observed in 11% of Nexavar-treated patients and 14% of placebo patients; CTCAE grade 3 or 4 neutropenia was reported in 1% of patients in each group.
Anemia was observed in 59% of Nexavar-treated patients and 64% of placebo patients; CTCAE grade 3 or 4 anemia was reported in 3% of patients in each group.
Thrombocytopenia was observed in 46% of Nexavar-treated patients and 41% of placebo patients; CTCAE grade 3 or 4 thrombocytopenia was reported in 4% of Nexavar-treated patients and <1% of placebo patients.
Hypocalcaemia was reported in 26.5% of sorafenib-treated patients compared to 14.8% of placebo patients. Most reports of hypocalcemia were low grade (CTCAE grade 1 and 2). CTCAE grade 3 hypocalcemia (6-7 mg /dL) occurred in 1.8% of sorafenib-treated patients and 1.1% of patients in the placebo group, and CTCAE grade 4 hypocalcemia (<6 mg/dL) occurred in 0.4% of sorafenib-treated patients and 0% of patients in the placebo group. The etiology of hypocalcemia associated with sorafenib is not known.
View ADR Monitoring Form