Body as a Whole: Moniliasis, fungal infection including Candida infection, edema, multiorgan failure, pyrexia, asthenia, pain (including pain in back, chest, and extremities), injection site reaction.
Cardiovascular: Chest pain, cardiac arrest, palpitation, ventricular tachycardia, ventricular arrhythmia, syncope, phlebitis, torsades de pointes, electrocardiogram QT prolonged, tachycardia, vasodilation, vasculitis, benign intracranial hypertension, hypotension.
CNS: Insomnia, anxiety, agitation, confusion, depression, hallucination, nightmare, sleep disorder, abnormal dreaming, psychosis, paranoia, isolated reports of suicide attempt and suicidal ideation, headache, dizziness, tremor, convulsions, paresthesia, vertigo, hypertonia, hyperkinesia, abnormal gait, somnolence, peripheral neuropathy (may be irreversible), isolated reports of encephalopathy, abnormal EEG, dysphonia, exacerbation of myasthenia gravis, amnesia, pseudotumor cerebri, nervousness, peripheral sensory neuropathy, peripheral sensory motor neuropathy, dyskinesia, extrapyramidal disorder.
Dermatologic and Sensitivity Reactions: Rash; pruritus; urticaria; allergic reaction; angioedema, hypersensitivity reactions, sometimes fatal including: anaphylactic/anaphylactoid reactions, anaphylactic shock, angioneurotic edema, serum sickness; bullous eruptions to include: Stevens-Johnson syndrome, toxic epidermal necrolysis, erythema multiforme, photosensitivity/phototoxicity reaction, leukocytoclastic vasculitis; hyperhidrosis; mucocutaneous reactions.
Endocrine and Metabolic: Hyperglycemia, hypoglycemia, hypoglycemic coma, hyperkalemia, anorexia.
Gastrointestinal: Nausea, diarrhea, constipation, abdominal pain, vomiting, dyspepsia, gastritis, stomatitis, pancreatitis, esophagitis, gastroenteritis, glossitis, pseudomembranous/C. difficile colitis, flatulence.
Hepatic: Abnormal hepatic function, increased hepatic enzymes (ALT/ASTCGT), increased alkaline phosphatase, hepatic failure (including fatal cases), hepatitis, jaundice, hepatic necrosis, blood bilirubin increased.
Hematologic: Anemia, thrombocytopenia, thrombocytopenia including thrombotic thrombocytopenic purpura, agranulocytosis, granulocytopenia, pancytopenia, aplastic anemia, leukopenia, hemolytic anemia, eosinophilia, neutropenia, prothrombin time prolonged, international normalized ratio (INR) prolonged.
Musculoskeletal: Tendon disorder including tendinitis, arthralgia, myalgia, skeletal pain, tendon rupture, muscle injury (including rupture), rhabdomyolysis, myositis, myalgia, ligament rupture, muscle rupture, arthritis, muscle enzymes increased (CPK).
Reproductive/Urogenital System: Vaginitis, genital moniliasis, abnormal renal function, acute renal failure, interstitial nephritis, nephrosis, glomerulonephritis, blood creatinine increased.
Respiratory: Dyspnea, epistaxis, allergic pneumonitis, interstitial pneumonia, laryngeal edema, apnea, bronchospasm.
Special Senses: Uveitis, vision disturbance (including diplopia), visual acuity reduced, vision blurred, transient vision loss, scotoma, hypoacusis, tinnitus, hearing loss, hearing impaired, anosmia, parosmia, dysgeusia, ageusia.


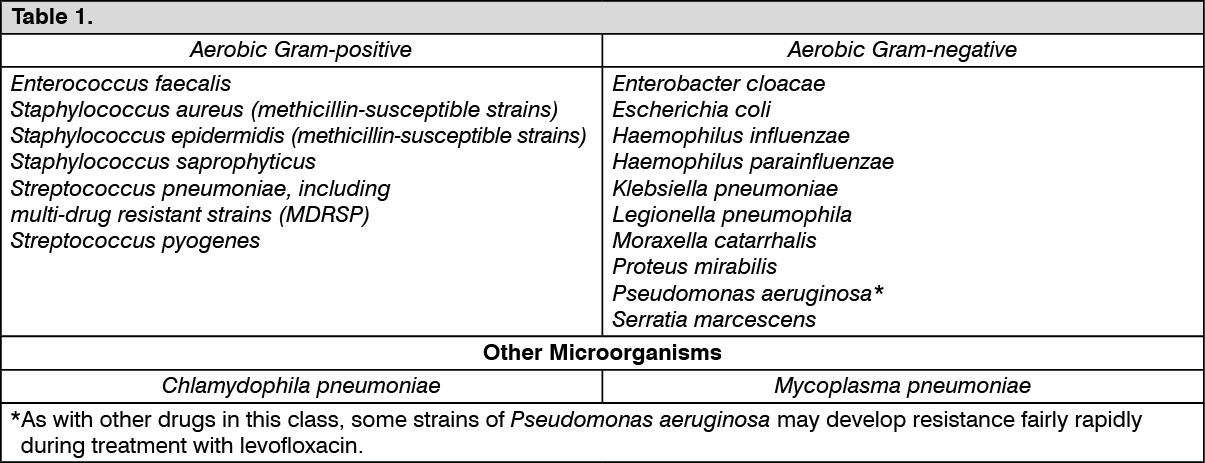 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image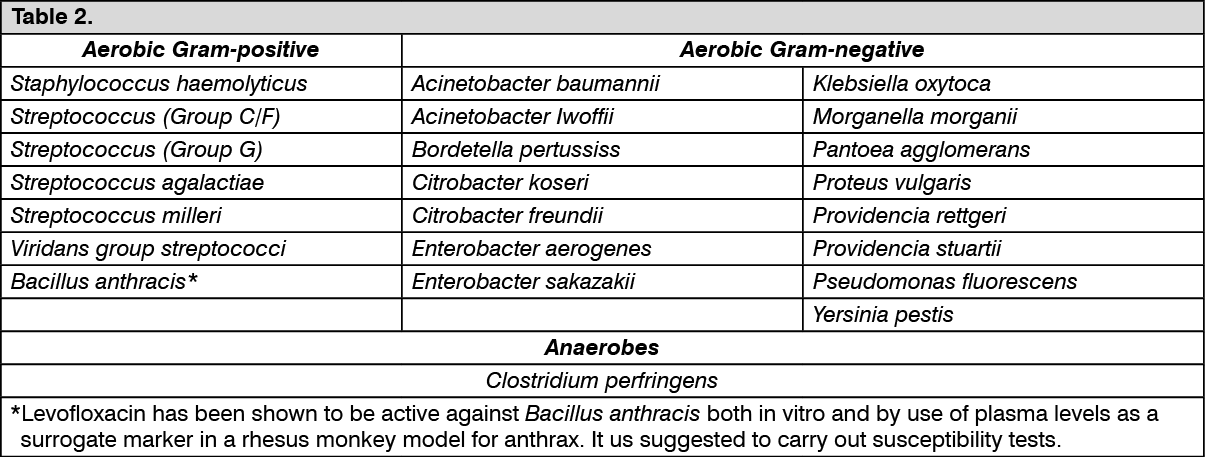 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image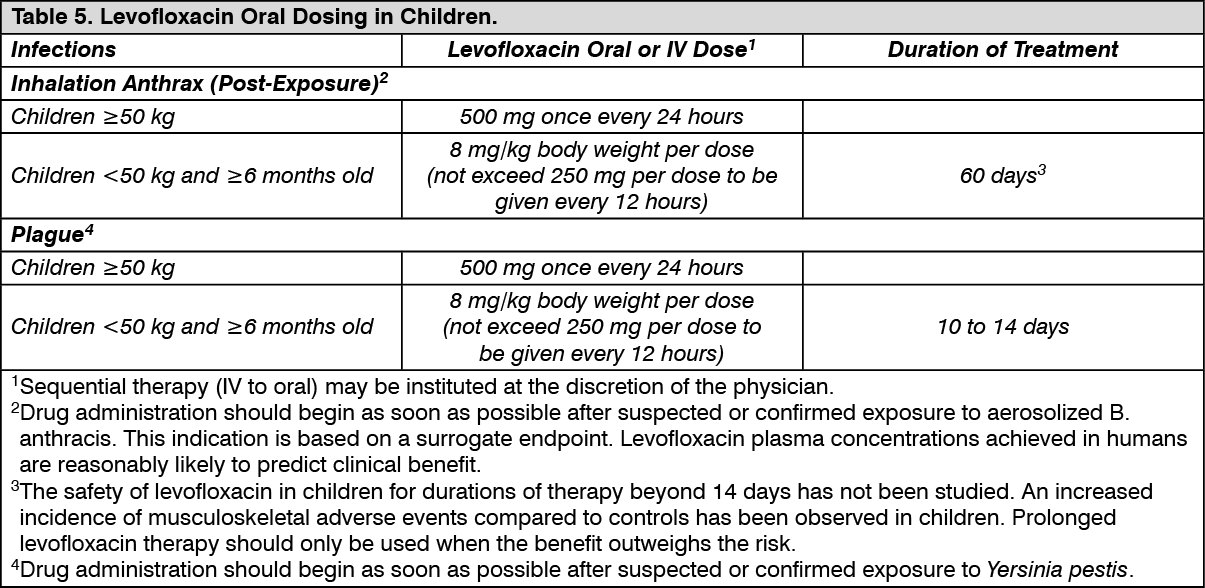 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
