Clinical Trial Data and Post-Marketing Data: Summary of the Safety Profile: The adverse event profile presented as follows is based on the analysis of pooled placebo-controlled clinical trials with all indications studied, with a total of 3,416 patients treated with levetiracetam. These data are supplemented with the use of levetiracetam in corresponding open-label extension studies as well as post-marketing experience. The most frequently reported adverse reactions were nasopharyngitis, somnolence, headache, fatigue and dizziness. The safety profile of levetiracetam is generally similar across age groups (adult and pediatric patients) and across the approved epilepsy indications.
Adverse reactions (ADRs) are listed as follows by MedDRA system organ class and by frequency.
Frequencies are defined as: Very common ≥1/10; common ≥1/100 to <1/10; uncommon ≥1/1,000 to <1/100; rare ≥1/10,000 to <1/1,000; very rare <1/10,000; not known (cannot be estimated from the available data).
Infections and Infestations: Very Common: Nasopharyngitis. Rare: Infection.
Blood and Lymphatic System Disorders: Uncommon: Thrombocytopenia, leukopenia. Rare: Pancytopenia, neutropenia, agranulocytosis.
Immune System Disorders: Rare: Drug reaction with eosinophilia and systemic symptoms (DRESS), hypersensitivity (including angioedema and anaphylaxis).
Metabolism and Nutrition Disorders: Common: Anorexia. Uncommon: Weight decreased, weight increase. Rare: Hyponatremia.
Psychiatric Disorders: Common: Depression, hostility/aggression, anxiety, insomnia, nervousness/irritability. Uncommon: Suicide attempt, suicidal ideation, psychotic disorder, abnormal behavior, hallucination, anger, confusional state, affect lability/mood swings, agitation. Rare: Completed suicide, personality disorder, abnormal thinking.
Nervous System Disorders: Very Common: Somnolence, headache. Common: Convulsion, balance disorder, dizziness, lethargy, tremor. Uncommon: Amnesia, memory impairment, abnormal coordination/ataxia, paresthesia, disturbance in attention. Rare: Choreoathetosis, dyskinesia, hyperkinesia.
Eye Disorders: Uncommon: Diplopia, blurred vision.
Ear and Labyrinth Disorders: Common: Vertigo.
Respiratory, Thoracic and Mediastinal Disorders: Common: Cough.
Gastrointestinal Disorders: Common: Abdominal pain, diarrhea, dyspepsia, vomiting, nausea. Rare: Pancreatitis.
Hepatobiliary Disorders: Uncommon: Liver function test abnormal. Rare: Hepatic failure, hepatitis.
Skin and Subcutaneous Tissue Disorders: Common: Rash. Uncommon: Alopecia, eczema, pruritus. Rare: Toxic epidermal necrolysis, Stevens-Johnson syndrome, erythema multiforme.
Musculoskeletal and Connective Tissue Disorders: Uncommon: Muscular weakness, myalgia.
General Disorders and Administration Site Conditions: Common: Asthenia/fatigue.
Injury, Poisoning and Procedural Complications: Uncommon: Injury.
Description of Selected Adverse Reactions: The risk of anorexia is higher when topiramate is co-administered with levetiracetam.
In several cases of alopecia, recovery was observed when levetiracetam was discontinued.
Bone marrow suppression was identified in some of the cases of pancytopenia.
Pediatric Population: In patients aged 1 month to less than 4 years, a total of 190 patients have been treated with levetiracetam in placebo-controlled and open-label extension studies. Sixty of these patients were treated with levetiracetam in placebo-controlled studies. In patients aged 4-16 years, a total of 645 patients have been treated with levetiracetam in placebo-controlled and open-label extension studies. 233 of these patients were treated with levetiracetam in placebo-controlled studies. In both these pediatric age ranges, these data are supplemented with the post-marketing experience of the use of levetiracetam.
In addition, 101 infants aged less than 12 months have been exposed in a post authorization safety study. No new safety concerns for levetiracetam were identified for infants less than 12 months of age with epilepsy.
The adverse event profile of levetiracetam is generally similar across age groups and across the approved epilepsy indications. Safety results in paediatric patients in placebo-controlled clinical studies were consistent with the safety profile of levetiracetam in adults except for behavioural and psychiatric adverse reactions which were more common in children than in adults. In children and adolescents aged 4 to 16 years, vomiting (very common, 11.2%), agitation (common, 3.4%), mood swings (common, 2.1%), affect lability (common, 1.7%), aggression (common, 8.2%), abnormal behaviour (common, 5.6%), and lethargy (common, 3.9%) were reported more frequently than in other age ranges or in the overall safety profile. In infants and children aged 1 month to less than 4 years, irritability (very common, 11.7%) and coordination abnormal (common, 3.3%) were reported more frequently than in other age groups or in the overall safety profile.
A double-blind, placebo-controlled paediatric safety study with a non-inferiority design has assessed the cognitive and neuropsychological effects of levetiracetam in children 4 to 16 years of age with partial onset seizures. It was concluded that levetiracetam was not different (non inferior) from placebo with regard to the change from baseline of the Leiter-R Attention and Memory, Memory Screen Composite score in the per-protocol population. Results related to behavioural and emotional functioning indicated a worsening in levetiracetam treated patients on aggressive behaviour as measured in a standardised and systematic way using a validated instrument (CBCL-Achenbach Child Behavior Checklist). However subjects, who took levetiracetam in the long-term open label follow-up study, did not experience a worsening, on average, in their behavioural and emotional functioning; in particular measures of aggressive behaviour were not worse than baseline.




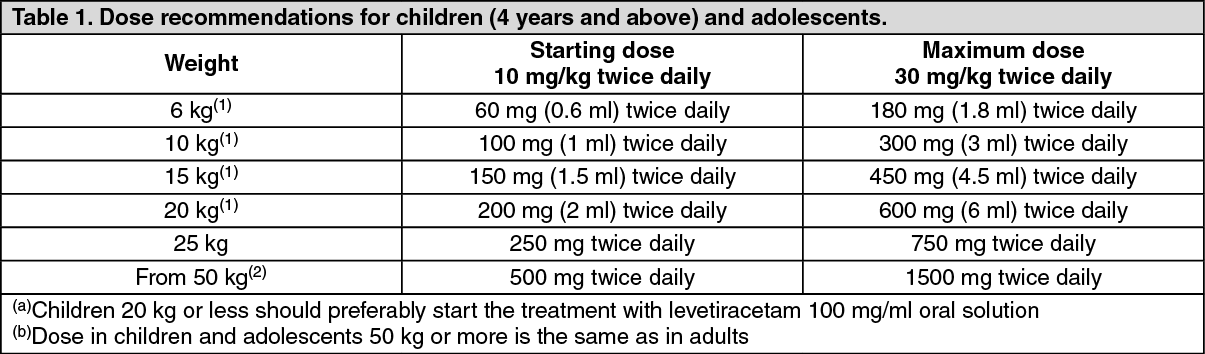 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image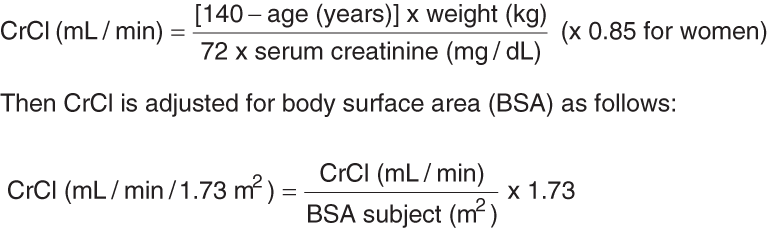 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image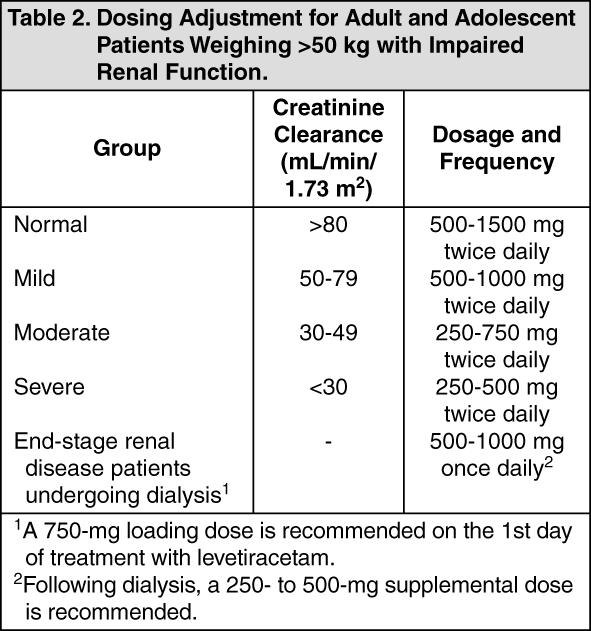 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image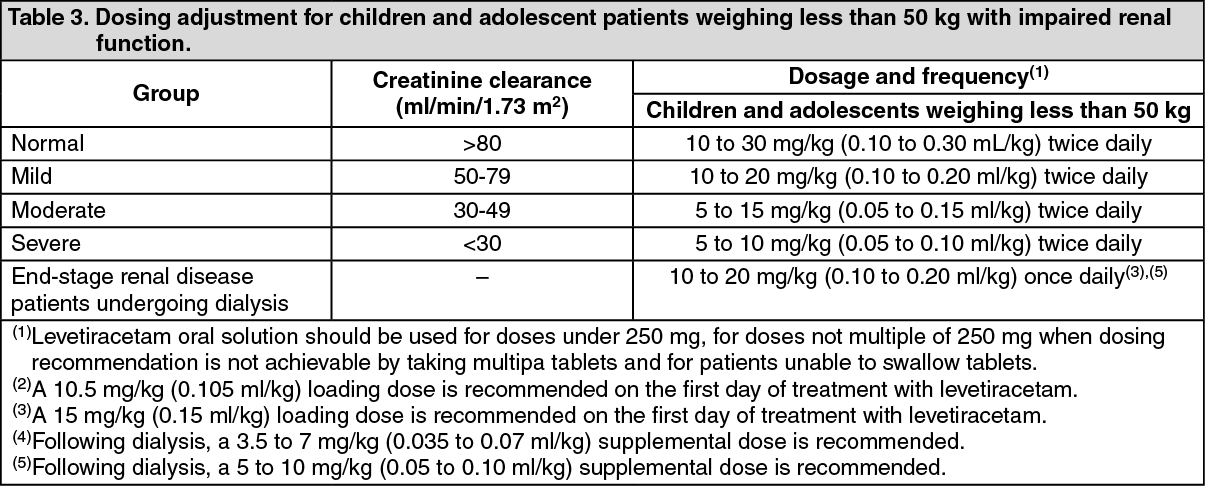 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
