Pharmaco-therapeutic group: Calcium homeostasis, parathyroid hormones and analogues.
ATC code: H05 AA02.
Pharmacology: Pharmacodynamics: Mechanism of action: Endogenous 84-amino-acid parathyroid hormone (PTH) is the primary regulator of calcium and phosphate metabolism in bone and kidney. Teriparatide (Forteo) [rhPTH(1-34)] is the active fragment (1-34) of endogenous human parathyroid hormone. Physiological actions of PTH include stimulation of bone formation by direct effects on bone forming cells (osteoblasts) indirectly increasing the intestinal absorption of calcium and increasing the tubular re-absorption of calcium and excretion of phosphate by the kidney.
Pharmacodynamic effects: Teriparatide (Forteo) is a bone formation agent to treat osteoporosis. The skeletal effects of Teriparatide (Forteo) depend upon the pattern of systemic exposure. Once-daily administration of Teriparatide (Forteo) increases apposition of new bone on trabecular and cortical bone surfaces by preferential stimulation of osteoblastic activity over osteoclastic activity.
Clinical efficacy: Risk Factors: Independent risk factors, for example, low BMD, age, the existence of previous fracture, family history of hip fractures, high bone turnover and low body mass index should be considered in order to identify women and men at increased risk of osteoporotic fractures who could benefit from treatment.
Premenopausal women with glucocorticoid-induced osteoporosis should be considered at high risk for fracture if they have a prevalent fracture or a combination of risk factors that place them at high risk for fracture (e.g. low bone density [e.g., T score ≤-2], sustained high dose glucocorticoid therapy [e.g., ≥7.5 mg/day for at least 6 months], high underlying disease activity, low sex steroid levels).
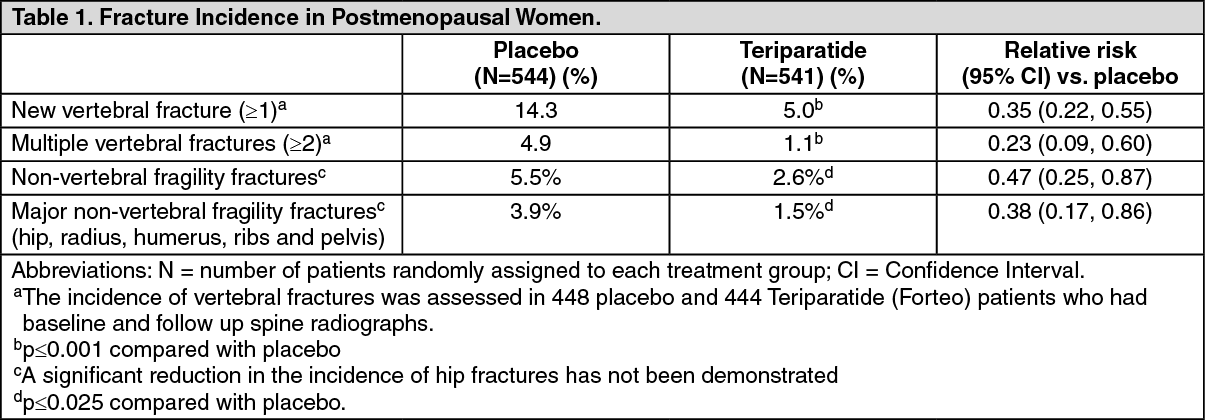
Postmenopausal osteoporosis: The pivotal study included 1637 postmenopausal women (mean age 69.5 years). At baseline, ninety percent of the patients had one or more vertebral fractures, and on average, vertebral BMD was 0.82 g/cm
2 (equivalent to a T-score = -2.6). All patients were offered 1000 mg calcium per day and at least 400 IU vitamin D per day. Results from up to 24 months (median: 19 months) treatment with Teriparatide (Forteo) demonstrate statistically significant fracture reduction (Table 1). To prevent one or more new vertebral fractures, 11 women had to be treated for a median of 19 months. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
After 19 months (median) treatment, bone mineral density (BMD) had increased in the lumbar spine and total hip, respectively, by 9% and 4% compared with placebo (p<0.001).
Post-treatment management: Following treatment with Teriparatide (Forteo), 1262 postmenopausal women from the pivotal trial enrolled in a post-treatment follow-up study. The primary objective of the study was to collect safety data of Teriparatide (Forteo). During this observational period, other osteoporosis treatments were allowed and additional assessment of vertebral fractures was performed.
During a median of 18 months following discontinuation of Teriparatide (Forteo) there was a 41% reduction (p=0.004) compared with placebo in the number of patients with a minimum of one new vertebral fracture.
In an open-label study, 503 postmenopausal women with severe osteoporosis and a fragility fracture within the previous 3 years (83% had received previous osteoporosis therapy) were treated with Teriparatide (Forteo) for up to 24 months. At 24 months, the mean increase from baseline in lumbar spine, total hip and femoral neck BMD was 10.5%, 2.6% and 3.9% respectively. The mean increase in BMD from 18 to 24 months was 1.4%, 1.2% and 1.6% at the lumbar spine, total hip and femoral neck, respectively.
A 24-month, randomized, double-blind, comparator-controlled Phase 4 study included 1,360 postmenopausal women with established osteoporosis. 680 subjects were randomized to Teriparatide (Forteo) and 680 subjects were randomized to oral risedronate 35 mg/week. At baseline, the women had a mean age of 72.1 years and a median of 2 prevalent vertebral fractures; 57.9% of patients had received previous bisphosphonate therapy and 18.8% took concomitant glucocorticoids during the study. 1,013 (74.5%) patients completed the 24-month follow-up. The mean (median) cumulative dose of glucocorticoid was 474.3 (66.2) mg in the teriparatide arm and 898.0 (100.0) mg in the risedronate arm. The mean (median) vitamin D intake for the teriparatide arm was 1433 IU/day (1400 IU/day) and for the risedronate arm was 1191 IU/day (900 IU/day). For those subjects who had baseline and follow-up spine radiographs, the incidence of new vertebral fractures was 28/516 (5.4%) in Teriparatide (Forteo) - and 64/533 (12.0%) in risedronate-treated patients, relative risk (95% CI) = 0.44 (0.29-0.68), P<0.0001. The cumulative incidence of pooled clinical fractures (clinical vertebral and non-vertebral fractures) was 4.8% in Teriparatide (Forteo) and 9.8% in risedronate-treated patients, hazard ratio (95% CI) = 0.48 (0.32-0.74), p=0.0009.
Male osteoporosis: 437 patients (mean age 58.7 years) were enrolled in a clinical trial for men with hypogonadal (defined as low morning free testosterone or an elevated FSH or LH) or idiopathic osteoporosis. Baseline spinal and femoral neck bone mineral density mean T-scores were -2.2 and -2.1, respectively. At baseline, 35% of patients had a vertebral fracture and 59% had a non-vertebral fracture.
All patients were offered 1000 mg calcium per day and at least 400 IU vitamin D per day. Lumbar spine BMD significantly increased by 3 months. After 12 months, BMD had increased in the lumbar spine and total hip by 5% and 1%, respectively, compared with placebo. However, no significant effect on fracture rates was demonstrated.
Glucocorticoid-induced osteoporosis: The efficacy of Teriparatide (Forteo) in men and women (N=428) receiving sustained systemic glucocorticoid therapy (equivalent to 5 mg or greater of prednisone for at least 3 months) was demonstrated in the 18-month, primary phase of a 36 month, randomized, double-blind, comparator-controlled study (alendronate 10 mg/day). Twenty-eight percent of patients had one or more radiographic vertebral fractures at baseline. All patients were offered 1000 mg calcium per day and 800 IU vitamin D per day.
This study included postmenopausal women (N=277), premenopausal women (N=67), and men (N=83). At baseline, the postmenopausal women had a mean age of 61 years, mean lumbar spine BMD T score of -2.7, median prednisone equivalent dose of 7.5 mg/day, and 34% had one or more radiographic vertebral fractures; premenopausal women had a mean age of 37 years, mean lumbar spine BMD T score of -2.5, median prednisone equivalent dose of 10 mg/day, and 9% had one or more radiographic vertebral fractures; and men had a mean age of 57 years, mean lumbar spine BMD T score of -2.2, median prednisone equivalent dose of 10 mg/day, and 24% had one or more radiographic vertebral fractures.
Sixty-nine percent of patients completed the 18-month primary phase. At the 18 month endpoint, Teriparatide (Forteo) significantly increased lumbar spine BMD (7.2%) compared with alendronate (3.4%) (p<0.001). Teriparatide (Forteo) increased BMD at the total hip (3.6%) compared with alendronate (2.2%) (p<0.01), as well as at the femoral neck (3.7%) compared with alendronate (2.1%) (p<0.05). In patients treated with teriparatide, lumbar spine, total hip and femoral neck BMD increased between 18 and 24 months by an additional 1.7%, 0.9%, and 0.4%, respectively.
At 36 months, analysis of spinal X-rays from 169 alendronate patients and 173 Teriparatide (Forteo) patients showed that 13 patients in the alendronate group (7.7%) had experienced a new vertebral fracture compared with 3 patients in the Teriparatide (Forteo) group (1.7%) (p=0.01). In addition, 15 of 214 patients in the alendronate group (7.0%) had experienced a non-vertebral fracture compared with 16 of 214 patients in the Teriparatide (Forteo) group (7.5%) (p=0.84).
In premenopausal women, the increase in BMD from baseline to 18 month endpoint was significantly greater in the Teriparatide (Forteo) group compared with the alendronate group at the lumbar spine (4.2% versus -1.9%; p<0.001) and total hip (3.8% versus 0.9%; p=0.005). However, no significant effect on fracture rates was demonstrated.
Pharmacokinetics: Distribution: The volume of distribution is approximately 1.7 L/kg. The half-life of Teriparatide (Forteo) is approximately 1 hour when administered subcutaneously, which reflects the time required for absorption from the injection site.
Biotransformation: No metabolism or excretion studies have been performed with Teriparatide (Forteo) but the peripheral metabolism of parathyroid hormone is believed to occur predominantly in liver and kidney.
Elimination: Teriparatide (Forteo) is eliminated through hepatic and extra-hepatic clearance (approximately 62 L/hr in women and 94 L/hr in men).
Elderly: No differences in Teriparatide (Forteo) pharmacokinetics were detected with regard to age (range 31 to 85 years). Dosage adjustment based on age is not required.
Toxicology: Preclinical safety data: Teriparatide (Forteo) was not genotoxic in a standard battery of tests. It produced no teratogenic effects in rats, mice or rabbits. There were no important effects observed in pregnant rats or mice administered teriparatide at daily doses of 30 to 1000 μg/kg. However, fetal resorption and reduced litter size occurred in pregnant rabbits administered daily doses of 3 to 100 μg/kg. The embryotoxicity observed in rabbits may be related to their much greater sensitivity to the effects of PTH on blood ionized calcium compared with rodents.
Rats treated with near-life time daily injections had dose-dependent exaggerated bone formation and increased incidence of osteosarcoma most probably due to an epigenetic mechanism. Teriparatide did not increase the incidence of any other type of neoplasia in rats. Due to the differences in bone physiology in rats and humans, the clinical relevance of these findings is probably minor. No bone tumors were observed in ovariectomised monkeys treated for 18 months or during a 3-year follow up period after treatment cessation. In addition, no osteosarcomas have been observed in clinical trials or during the post treatment follow-up study.
Animal studies have shown that severely reduced hepatic blood flow decreases exposure of PTH to the principal cleavage system (Kupffer cells) and consequently clearance of PTH(1-84).





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
