Ciprofloxacin (tab: hydrochloride; infusion: lactate).
Ciprofloxacin (Ciprobay) film-coated tablets 500 mg: Each film-coated tablet contains: Ciprofloxacin hydrochloride 500 mg.
Ciprofloxacin (Ciprobay) solution for infusion (0.9% NaCl): Each mL contains: Ciprofloxacin (as lactate) 2 mg.
200 mg/100 mL: Each glass bottle with 100 mL solution for infusion contains 200 mg ciprofloxacin. The sodium content is 354 mg (15.4 mmol).
400 mg/200 mL: Each glass bottle with 200 mL solution for infusion contains 400 mg ciprofloxacin. The sodium content is 708 mg (30.8 mmol).
Excipients/Inactive Ingredients: Ciprofloxacin (Ciprobay) film-coated tablets: Tablet core: Cellulose microcrystalline, Crospovidone, Maize starch, Magnesium stearate, Silica colloidal anhydrous.
Film-coat: Hypromellose, Macrogol 4000, Titanium dioxide (E171).
Ciprofloxacin (Ciprobay) solution for infusion (0.9% NaCl): Lactic acid, Sodium chloride, Hydrochloric acid concentrated, Water for injections.
Pharmacology: Pharmacodynamics: Mechanism of action: Ciprofloxacin has in vitro activity against a wide range of Gram-negative and Gram-positive organisms. The bactericidal action of ciprofloxacin results from inhibition of bacterial type II topoisomerases (DNA gyrase) and topoisomerase IV, which are required for bacterial DNA replication, transcription, repair, and recombination.
Mechanism of resistance: In vitro resistance to ciprofloxacin is commonly due to target site mutations in topoisomerase IV and DNA gyrase through multiple-step mutations. Single mutations may result in reduced susceptibility rather than clinical resistance, but multiple mutations generally result in clinical resistance to ciprofloxacin and cross-resistance across the fluoroquinolone class.
Resistance mechanisms that inactivate other antibiotics such as permeation barriers (common in Pseudomonas aeruginosa) and efflux mechanisms may affabect susceptibility to ciprofloxacin. Plasmid-mediated resistance encoded by the qnr gene has been reported. Resistance mechanisms that inactive penicillins, cephalosporins, aminoglycosides, macrolides, and tetracyclines may not interfere with the antibacterial activity of ciprofloxacin. Organisms resistant to these drugs may be susceptible to ciprofloxacin.
The minimal bactericidal concentration (MBC) generally does not exceed the minimal inhibitory concentration (MIC) by more than a factor of 2.
In vitro susceptibility to ciprofloxacin: The prevalence of acquired resistance may vary geographically and with time for selected species and local information of resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought where the local prevalence of resistance is such that utility of the agent, in at least some types of infections, is questionable.
The bacterial genus and species listed as follows have been shown to commonly be susceptible to ciprofloxacin in vitro: Aerobic Gram-positive microorganisms: Bacillus anthracis, Staphylococcus aureus (methicillin-susceptible isolates), Staphylococcus saprophyticus, Streptococcus spp.
Aerobic Gram-negative microorganisms: Aeromonas spp., Brucella spp., Citrobacter koseri, Francisella tularensis, Haemophilus ducreyi, Haemophilius influenzae, Legionella spp., Moraxella catarrhalis, Neisseria meningitidis, Pasteurella spp., Salmonella spp., Shigella spp., Vibrio spp., Yersinia pestis.
Anaerobic microorganisms: Mobiluncus.
Other microorganisms: Chlamydia trachomatis, Chlamydia pneumoniae, Mycoplasma hominis, Mycoplasma pneumoniae.
The following microorganisms show varying degrees of susceptibility to ciprofloxacin: Acinetobacter baumannii, Burkholderia cepacia, Campylobacter spp., Citrobacter freudii, Enterococcus faecalis, Enterobacter aerogenes, Enterobacter clocae, Escherichia coli, Klebsiella pneumoniae, Klebsiella oxytoca, Morganella morganii, Neisseria gonorrhoeae, Proteus mirabilis, Proteus vulgaris, Providencia spp., Pseudomonas aeruginosa, Pseudomonas fluorescens, Serratia marcescens, Peptostreptococcus spp., Propionibacterium acnes. The following microorganisms are considered inherently resistant to ciprofloxacin: Staphylococcus aureus (methicillin-resistant) and Stenotrophomonas maltophilia, Actinomyces, Enteroccus faecium, Listeria monocytogenes, Mycoplasma genitalium, Ureaplasma urealitycum, Anaerobic microorganisms (Excepted Mobiluncus, Peptostreptococus, Propionibacterium acnes).
Pharmacokinetics: Absorption: Film-coated tablet: Following oral administration of single doses of 250 mg, 500 mg, and 750 mg of Ciprofloxacin (Ciprobay) film-coated tablets, ciprofloxacin is absorbed rapidly and extensively, mainly from the small intestine, reaching maximum serum concentrations 1-2 hours later.
The absolute bioavailability is approximately 70-80%. Maximum serum concentrations (Cmax) and total areas under serum concentration vs. time curves (AUC) increased in proportion to dose.
Solution for infusion: Following an intravenous infusion of ciprofloxacin the mean maximum serum concentrations were achieved at the end of infusion. Pharmacokinetics of ciprofloxacin were linear over the dose range up to 400 mg administered intravenously.
Distribution: The protein binding of ciprofloxacin is low (20-30%), and the substance is present in plasma largely in a non-ionized form. Ciprofloxacin can diffuse freely into the extravascular space. The large steady-state distribution volume of 2-3 L/kg body weight shows that ciprofloxacin penetrates in tissues resulting in concentrations which clearly exceed the corresponding serum levels.
Metabolism: Small concentrations of four metabolites have been reported, and were identified as: desethyleneciprofloxacin (M 1), sulphociprofloxacin (M 2), oxociprofloxacin (M 3) and formylciprofloxacin (M 4). M 1 to M 3 display in vitro antimicrobial activity comparable to, or inferior to that of nalidixic acid. M 4, with the smallest quantity, is largely equivalent to norfloxacin in terms of in vitro antimicrobial activity.
Elimination: Ciprofloxacin is largely excreted unchanged both renally and, to a smaller extent, non-renally.
Children: In a study in children, Cmax and AUC were not age-dependent. No notable increase in Cmax and AUC upon multiple dosing (10 mg/kg/TID) was observed. In ten children with severe sepsis, less than 1 year of age, Cmax was 6.1 mg/L (range 4.6-8.3 mg/L) after a 1-hour intravenous infusion at a dose level of 10 mg/kg; and 7.2 mg/L (range 4.7-11.8 mg/L) for children between 1 and 5 years of age. The AUC-values were 17.4 mg*h/L (range 11.8-32.0 mg*h/L) and 16.5 mg*h/L (range 11.0-23.8 mg*h/L) in the respective age groups. These values are within the range reported for adults at therapeutic doses. Based on population, pharmacokinetic analysis of pediatric patients with various infections, the predicted mean half-life in children is approximately 4-5 hours and the bioavailability of the oral suspension approximately 60%.
Toxicology: Preclinical safety data: Acute toxicity: The acute toxicity of ciprofloxacin after oral administration can be classified as very low. Depending on the individual species, the LD50 after intravenous infusion is 125-290 mg/kg.
Chronic Toxicity: Chronic tolerability studies over 6 months: Oral administration: Doses up to and including 500 mg/kg and 30 mg/kg were tolerated without damage by rats and monkeys, respectively. Changes in the distal renal tubules were again observed in some monkeys in the highest-dose group (90 mg/kg).
Parenteral administration: In monkeys slightly elevated urea and creatinine concentrations and changes in the distal renal tubules were recorded in the highest-dose group (20 mg/kg).
Carcinogenicity: In carcinogenicity studies in mice (21 months) and rats (24 months) with doses up to approximately 1000 mg/kg body weight/day in mice and 125 mg/kg body weight/day in rats (increased to 250 mg/kg body weight/day after 22 weeks), there was no evidence of a carcinogenic potential at any dose level.
Reproduction toxicology: Fertility studies in rats: Fertility, the intrauterine and postnatal development of the young, and the fertility of F1 generation were not affected by ciprofloxacin.
Embryotoxicity studies: These yielded no evidence of any embryotoxic or teratogenic action of ciprofloxacin.
Perinatal and postnatal development in rats: No effects on the perinatal or postnatal development of the animals were detected. At the end of the rearing period histological investigations did not show any sign of articular damage in the young.
Mutagenicity: Eight in vitro mutagenicity tests have been conducted with ciprofloxacin.
Although two of the eight in vitro assays (i.e. the Mouse Lymphoma Cell Forward Mutation Assay and the Rat Hepatocyte Primary Culture DNA Repair Assay [UDS]) were positive, all of the in vivo test systems covering all relevant endpoints gave negative results.
Special tolerability studies: Articular tolerability studies: As it is also known for other gyrase inhibitors, ciprofloxacin causes damage to the large, weight-bearing joints in immature animals.
The extent of the cartilage damage varies according to age, species, and dose; the damage can be reduced by taking the weight off the joints. Studies with mature animals (rat, dog) revealed no evidence of cartilage lesions. In a study in young beagle dogs ciprofloxacin at high doses (1.3 to 3.5 times the therapeutic dose) caused articular changes after two weeks of treatment, which were still observed after five months. At therapeutic doses no effects were observed.
Uncomplicated and complicated infections caused by ciprofloxacin susceptible pathogens.
Infections of the respiratory tract: Ciprofloxacin can be regarded as an advisable treatment for pneumonias caused by Klebsiella spp., Enterobacter spp., Proteus spp., Escherichia coli, Pseudomonas aeruginosa, Haemophilus spp., Moraxella catarrhalis, Legionella spp., and staphylococci.
Infections of the middle ear (otitis media), of the paranasal sinuses (sinusitis), especially if these are caused by Gram-negative organisms including Pseudomonas aeruginosa or by staphylococci.
Infections of the eyes.
Infections of the kidneys and/or the efferent urinary tract.
Infections of the genital organs, including adnexitis, gonorrhea, prostatitis.
Infections of the abdominal cavity (e.g. infections of the gastrointestinal tract or of the biliary tract, peritonitis).
Infections of the skin and soft tissue Infections of the bones and joints.
Sepsis.
Infections or imminent risk of infection (prophylaxis) in patients whose immune system has been weakened (e.g. patients on immunosuppressants or have neutropenia).
Selective intestinal decontamination in immunosuppressed patients.
Prophylaxis of invasive infections due to Neisseria meningitidis.
Consideration should be given to available official guidance on the appropriate use of antibacterial agents.
Children: Ciprofloxacin may be used in children for the second- and third-line treatment of complicated urinary tract infections and pyelonephritis due to Escherichia coli (age range applied in clinical studies: 1-17 years) and for the treatment of acute pulmonary exacerbation of cystic fibrosis associated with Pseudomonas aeruginosa (age range applied in clinical studies: 5-17 years).
Treatment should only be initiated after careful benefit/risk evaluation, due to possible adverse events related to joints and/or surrounding tissues.
The clinical trials in children were performed in the indications listed previously. For other indications clinical experience is limited.
Inhalational anthrax (post-exposure) in adults and in children: To reduce the incidence or progression of disease following exposure to aerosolized Bacillus anthracis.
Ciprobay: Method of administration: Film-coated tablet: For oral use.
Ciprofloxacin (Ciprobay) film-coated tablets are to be swallowed whole with a small amount of fluid.
Ciprofloxacin (Ciprobay) film-coated tablets can be taken independently of mealtimes.
If they are taken on an empty stomach, the active substance is absorbed more rapidly. In this case, Ciprofloxacin (Ciprobay) film-coated tablets should not be taken concurrently with dairy products or with mineral-fortified drinks alone (e.g. milk, yoghurt, calcium-fortified orange juice) (see Interactions).
If the patient is unable to take Ciprofloxacin (Ciprobay) film-coated tablets because of the severity of the illness or for other reasons (e.g. patients on enteral nutrition), it is recommended to commence the therapy with an intravenous form of ciprofloxacin. After intravenous administration, the treatment can be continued orally.
Solution for infusion: For intravenous use.
Ciprofloxacin (Ciprobay) solution for infusion should be administered by intravenous infusion over a period of 60 minutes. Slow infusion into a large vein will minimize patient discomfort and reduce the risk of venous irritation. The solution for infusion can be infused either directly or after mixing with other compatible solutions for infusion.
Unless compatibility with other solutions for infusion/medicinal products has been confirmed, the solution for infusion must always be administered separately. The visual signs of incompatibility are e.g. precipitation, clouding and discoloration.
Incompatibility appears with all solutions for infusion/medicinal products that are physically or chemically unstable at the pH of the solution (e.g. penicillins, heparin solutions), especially on combination with solutions adjusted to an alkaline pH (pH of Ciprofloxacin (Ciprobay) solutions for infusion: 3.9 - 4.5). Only clear solutions are to be used.
Duration of treatment: The duration of treatment depends on the severity of the illness and on the clinical and bacteriological course. It is essential to continue therapy for at least 3 days after disappearance of the fever or of the clinical symptoms.
Mean duration of treatment:
Adults: 1 day for acute uncomplicated gonorrhea and cystitis; up to 7 days for infections of the kidneys, urinary tract and abdominal cavity; over the entire period of the neutropenic phase in patients with weakened body defenses; a maximum of 2 months in osteomyelitis; and 7-14 days in all other infections.
In streptococcal infections, the treatment must last at least ten days because of the risk of late complications.
Infections caused by
Chlamydia spp. should also be treated for a minimum of ten days.
Children and adolescents: Cystic Fibrosis: For acute pulmonary exacerbation of cystic fibrosis associated with
Pseudomonas aeruginosa infection in pediatric patients (aged 5-17 years), the duration of treatment is 10-14 days.
Complicated Urinary Tract Infections and Pyelonephritis: For complicate urinary tract infections or pyelonephritis due to
Escherichia coli, the duration of treatment is 10-21 days.
Dosage regimen: Unless otherwise prescribed, the following daily doses are recommended for:
Adults: Film-coated tablet: See Table 1.
 Click on icon to see table/diagram/image
Solution for infusion:
Click on icon to see table/diagram/image
Solution for infusion: See Table 2.
Click on icon to see table/diagram/image
Children and adolescents: Film-coated tablet: See Table 3.
Click on icon to see table/diagram/image
Solution for infusion: See Table 4.
Click on icon to see table/diagram/image
Missed dose: Film-coated tablet: If a dose is missed it should be taken as soon as the patient remembers and then treatment should be continued as prescribed. Double doses should not be taken to compensate for a missed dose.
Additional information on special populations: Children and adolescents: For recommended dosage regimen, see Tables 3 and 4.
Geriatric patients: Elderly patients should receive a dose as low as possible depending on the severity of their illness and the creatinine clearance (see also Patients with renal and hepatic impairment).
Patients with renal and hepatic impairment: Adults: Patients with renal impairment: Film-coated tablet: See Table 5.
Click on icon to see table/diagram/image
Solution for infusion: See Table 6.
Click on icon to see table/diagram/image
Patients with renal impairment on hemodialysis: Film-coated tablet: For patients with creatinine clearance between 30 and 60 mL/min/1.73 m
2 (moderate renal impairment) or serum creatinine concentration between 1.4 and 1.9 mg/100 mL, the maximum daily oral dose of ciprofloxacin should be 1000 mg.
For patients with creatinine clearance less than 30 mL/min/1.73 m
2 (severe renal impairment) or serum creatinine concentration equal or higher than 2.0 mg/100 mL, the maximum daily oral dose of ciprofloxacin should be 500 mg on dialysis days after dialysis.
Solution for infusion: For patients with creatinine clearance between 30 and 60 mL/min/1.73 m
2 (moderate renal impairment) or serum creatinine concentration between 1.4 and 1.9 mg/100 mL, the maximum daily intravenous dose of ciprofloxacin should be 800 mg.
For patients with creatinine clearance less than 30 mL/min/1.73 m
2 (severe renal impairment) or serum creatinine concentration equal or higher than 2.0 mg/100 mL, the maximum daily intravenous dose of ciprofloxacin should be 400 mg on dialysis days after dialysis.
Patients with renal impairment on continuous ambulatory peritoneal dialysis (CAPD): Film-coated tablet: The maximum daily oral dose of ciprofloxacin should be 500 mg (1 x 500 mg Ciprofloxacin (Ciprobay) film-coated tablet or 2 x 250 mg Ciprofloxacin (Ciprobay) film-coated tablets).
Solution for infusion: Addition of Ciprofloxacin (Ciprobay) solution for infusion to the dialysate (intraperitoneal): 50 mg ciprofloxacin / liter dialysate administered 4 times a day every 6 hours.
Patients with hepatic impairment: In patients with hepatic impairment, no dose adjustment is required.
Patients with renal and hepatic impairment: Film-coated tablet: For patients with creatinine clearance between 30 and 60 mL/min/1.73 m
2 (moderate renal impairment) or serum creatinine concentration between 1.4 and 1.9 mg/100 mL, the maximum daily oral dose of ciprofloxacin should be 1000 mg.
For patients with creatinine clearance less than 30 mL/min/1.73 m
2 (severe renal impairment) or serum creatinine concentration equal or higher than 2.0 mg/100 mL, the maximum daily oral dose of ciprofloxacin should be 500 mg.
Solution for infusion: For patients with creatinine clearance between 30 and 60 mL/min/1.73 m
2 (moderate renal impairment) or serum creatinine concentration between 1.4 and 1.9 mg/100 mL, the maximum daily intravenous dose of ciprofloxacin should be 800 mg.
For patients with creatinine clearance less than 30 mL/min/1.73 m
2 (severe renal impairment) or serum creatinine concentration equal or higher than 2.0 mg/100 mL, the maximum daily intravenous dose of ciprofloxacin should be 400 mg.
Children: Dosing in children with impaired renal and/or hepatic function has not been studied.
Film-coated tablet: In the event of acute, excessive oral overdosage, reversible renal toxicity has been reported in some cases.
Apart from routine emergency measures, it is recommended to monitor renal function, including urinary pH and acidify, if required, to prevent crystalluria. Patients should be kept well hydrated. Calcium or magnesium containing antacids may reduce the absorption of ciprofloxacin in overdoses.
Only a small quantity of ciprofloxacin (< 10%) is eliminated by hemodialysis or peritoneal dialysis.
Solution for infusion: Apart from routine emergency measures, it is recommended to monitor renal function, including urinary pH and acidify, if required, to prevent crystalluria. Patients should be kept well hydrated. Only a small quantity of ciprofloxacin (< 10%) is eliminated by hemodialysis or peritoneal dialysis.
Hypersensitivity to ciprofloxacin or other fluoroquinolone or any of the excipients (see Excipients/Inactive Ingredients under Description),
Concurrent administration of ciprofloxacin and tizanidine (see Interactions).
Severe infections and/or infections due to Gram-positive or anaerobic bacteria: For the treatment of severe infections, staphylococcal infections and infections involving anaerobic bacteria, Ciprofloxacin (Ciprobay) should be used in combination with an appropriate antibacterial agent.
Streptococcus pneumoniae infections: Ciprofloxacin (Ciprobay) is not recommended for treatment of pneumococcal infections due to limited efficacy against Streptococcus pneumoniae.
Genital tract infections: Genital tract infections may be caused by fluoroquinolone-resistant Neisseria gonorrhoeae isolates. In genital tract infections thought or known to be due to Neisseria gonorrhoeae, it is particularly important to obtain local information on the prevalence of resistance to ciprofloxacin and to confirm susceptibility based on laboratory testing.
Cardiac disorders: Ciprofloxacin (Ciprobay) is associated with cases of QT prolongation (see Adverse Reactions). As women tend to have a longer baseline QTc interval compared with men, they may be more sensitive to QTc-prolonging medications. Elderly patients may also be more susceptible to drug-associated effects on the QT interval. Precaution should be taken when using Ciprofloxacin (Ciprobay) with concomitant drugs that can result in prolongation with the QT interval (e.g. class IA or III antiarrhythmics, tricyclic antidepressants, macrolides, antipsychotics) (see Interactions) or in patients with risk factors for QT prolongation or torsade de pointes (e.g. congenital long QT syndrome, uncorrected electrolyte imbalance such as hypokalemia or hypomagnesemia and cardiac disease such as heart failure, myocardial infarction, or bradycardia).
Children and adolescents: As with medicinal products in its class, ciprofloxacin has been shown to cause arthropathy in weight-bearing joints of immature animals (see Adverse Reactions). The analysis of available safety data from ciprofloxacin use in patients less than 18 years of age, the majority of whom had cystic fibrosis, did not disclose any evidence of drug-related cartilage or articular damage. The use of Ciprofloxacin (Ciprobay) for indications other than the treatment of acute pulmonary exacerbation of cystic fibrosis caused by Pseudomonas aeruginosa infection (children aged 5-17 years), complicated urinary tract infections and pyelonephritis due to Escherichia coli (children aged 1-17 years), and for the use in inhalational anthrax (post-exposure) was not studied. For other indications, clinical experience is limited.
Hypersensitivity: In some instances, hypersensitivity and allergic reactions may occur following a single dose (see Adverse Reactions), a physician should be informed immediately.
Anaphylactic/anaphylactoid reactions in very rare instances can progress to a life-threatening shock, in some instances after the first administration (see Adverse Reactions). In these cases, Ciprofloxacin (Ciprobay) has to be discontinued and medical treatment (e.g. treatment for shock) is required.
Gastrointestinal system: In the event of severe and persistent diarrhea during or after treatment, a physician must be consulted since this symptom can hide a serious intestinal disease (life-threatening pseudomembranous colitis with possible fatal outcome), requiring immediate treatment (see Adverse Reactions). In such cases, Ciprofloxacin (Ciprobay) must be discontinued and appropriate therapy initiated (e.g. vancomycin, orally, 4 x 250 mg/day). Medicinal products that inhibit peristalsis are contraindicated in this situation.
Hepatobiliary system: Cases of hepatic necrosis and life-threatening hepatic failure have been reported with Ciprofloxacin (Ciprobay). In the event of any signs and symptoms of hepatic disease (such as anorexia, jaundice, dark urine, pruritus, or tender abdomen), treatment should be discontinued (see Adverse Reactions).
There can be a temporary increase in transaminases, alkaline phosphatase, or cholestatic jaundice, especially in patients with previous liver damage, who are treated with Ciprofloxacin (Ciprobay) (see Adverse Reactions).
Myasthenia gravis: Ciprofloxacin (Ciprobay) should be used with caution in patients with myasthenia gravis, because symptoms can be exacerbated.
Musculoskeletal system: Ciprofloxacin (Ciprobay) should be used with caution in patients with myasthenia gravis, because symptoms can be exacerbated.
Tendinitis and tendon rupture: Tendinitis and tendon rupture (predominantly Achilles tendon), sometimes bilateral, may occur with Ciprofloxacin (Ciprobay), even within the first 48 hours of treatment. Cases occurring up to several months after completion of therapy have been reported (see Adverse Reactions). The risk of tendinopathy may be increased in elderly patients, during strenuous physical activity, in patients treated concomitantly with corticosteroids, in patients with renal impairment and patients with solid organ transplants.
At any sign of tendinitis (e.g. painful swelling, inflammation), the affected extremity should be kept at rest, any inappropriate physical exercise should be avoided, a physician should be consulted and the antibiotic treatment should be discontinued. Ciprofloxacin (Ciprobay) should be used with caution in patients with a history of tendon disorders related to fluoroquinolone treatment.
Seizures: Ciprofloxacin (Ciprobay), like other fluoroquinolones, is known to trigger seizures or lower the seizure threshold. In epileptics and patients who have suffered from previous central nervous system (CNS) disorders (e.g. lowered convulsion threshold, previous history of convulsion, reduced cerebral blood flow, altered brain structure or stroke), Ciprofloxacin (Ciprobay) should only be used where the benefits of treatment exceed the risks, since these patients are endangered because of possible undesirable CNS effects. Cases of status epilepticus have been reported (see Adverse Reactions). If seizures occur, Ciprofloxacin (Ciprobay) should be discontinued.
Psychiatric Reactions: Psychiatric reactions may occur even after the first administration of fluoroquinolones, including Ciprofloxacin (Ciprobay). In rare cases, depression or psychotic reactions can progress to suicidal ideations/thoughts and self-injurious behavior, such as attempted or completed suicide (see Adverse Reactions). In the event that the patient develops these reactions, Ciprofloxacin (Ciprobay) should be discontinued and appropriate measures instituted.
Peripheral neuropathy: Cases of sensory or sensorimotor polyneuropathy resulting in paresthesias, hypoesthesias, dysesthesias, or weakness have been reported in patients receiving fluoroquinolones including Ciprofloxacin (Ciprobay). Patients under treatment with Ciprofloxacin (Ciprobay) should be advised to inform their doctor prior to continuing treatment if symptoms of neuropathy such as pain, burning, tingling, numbness, or weakness develop (see Adverse Reactions).
Skin and appendages: Ciprofloxacin has been shown to produce photosensitivity reactions. Patients taking Ciprofloxacin (Ciprobay) should avoid direct exposure to excessive sunlight or UV-light. Therapy should be discontinued if photosensitization (i.e. sunburn-like skin reactions) occurs (see Adverse Reactions).
Cytochrome P450: Ciprofloxacin is known to be a moderate inhibitor of the CYP 450 1A2 enzymes. Care should be taken when other medicinal products are administered concomitantly which are metabolized via the same enzymatic pathway (e.g. tizanidine, theophylline, methylxantines, caffeine, duloxetine, ropinirole, clozapine, olanzapine, agomelatine). Increased plasma concentrations associated with drug-specific undesirable effects may be observed due to inhibition of their metabolic clearance by ciprofloxacin (see Interactions).
Dysglycemia: As with all fluoroquinolones, disturbances in blood glucose, including both hypoglycemia and hyperglycemia have been reported with Ciprobay. In Ciprobay-treated patients, dysglycemia occurred predominantly in elderly diabetic patients receiving concomitant treatment with an oral hypoglycemic agent (e.g. sulfonylurea) or with insulin. In diabetic patients, careful monitoring of blood glucose is recommended (see Adverse Reactions).
Injection site reaction: Solution for infusion: Local intravenous site reactions have been reported with the intravenous administration of Ciprofloxacin (Ciprobay) (see Adverse Reactions). These reactions are more frequent if the infusion time is 30 minutes or less. These may appear as local skin reactions which resolve rapidly upon completion of the infusion. Subsequent intravenous administration is not contraindicated unless the reactions recur or worsen.
Interaction with tests: Ciprofloxacin in vitro potency may interfere with the Mycobacterium tuberculosis culture test by suppression of mycobacterial growth, causing false negative results in specimens from patients currently taking Ciprofloxacin (Ciprobay).
Aortic aneurysm and dissection: Epidemiologic studies report an increased risk of aortic aneurysm and dissection after intake of fluoroquinolones, particularly in the older population.
Therefore, fluoroquinolones should only be used after careful benefit-risk assessment and after consideration of other therapeutic options in patients with positive family history of aneurysm disease, or in patients diagnosed with pre-existing aortic aneurysm and/or dissection, or in presence of other risk factors or conditions predisposing for aortic aneurysm and dissection (e.g. Marfan syndrome, vascular Ehlers-Danlos syndrome, Takayasu arteritis, giant cell arteritis, Behcet´s disease, hypertension, known atherosclerosis).
In case of sudden abdominal, chest or back pain, patients should be advised to immediately consult a physician in an emergency department.
Effects on ability to drive or use machines: Fluoroquinolones including ciprofloxacin may result in an impairment of the patient's ability to drive or operate machinery due to CNS reactions (see Adverse Reactions). This applies particularly in combination with alcohol.
Pregnancy: The data, that are available from the use of ciprofloxacin in pregnant women, indicate neither malformative nor feto/neonatal toxicity. Animal studies do not indicate reproductive toxicity. Based on animal studies, it cannot be excluded that the drug could cause damage to articular cartilage in the immature fetal organism (see Pharmacology: Toxicology: Preclinical safety data under Actions), therefore, the use of Ciprofloxacin (Ciprobay) is not recommended during pregnancy.
Animal studies have not shown any evidence of teratogenic effects (malformations) (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Lactation: Ciprofloxacin is excreted in breast milk. Due to the potential risk of articular damage, the use of Ciprofloxacin (Ciprobay) is not recommended during breast-feeding (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Summary of the safety profile: Adverse drug reactions (ADRs) based on all clinical studies with ciprofloxacin (oral, parenteral) sorted by CIOMS III categories of frequency are listed as follows (overall n = 51621).
Tabulated list of adverse reactions: The frequencies of ADRs reported with Ciprofloxacin (Ciprobay) are summarized in the following table. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000).
The ADRs identified only during post marketing surveillance, and for which a frequency could not be estimated, are listed under 'not known'. (See Table 7.)
Click on icon to see table/diagram/image
In isolated instances, some serious adverse drug reactions may be long-lasting (> 30 days) and disabling; such as tendinitis, tendon rupture, musculoskeletal disorders, and other reactions affecting the nervous system including psychiatric disorders and disturbance of senses.
The following undesirable effects have a higher frequency category in the subgroups of patients receiving intravenous or sequential (intravenous to oral) treatment: See Table 8.
Click on icon to see table/diagram/image
The MedDRA preferred term is used to describe a certain reaction and its synonyms and related conditions. ADR term representation is based on MedDRA version 14.0 (except for 'Mycotic Superinfections' and 'Unspecific Pain').
Additional information on special populations: Pediatric population: The incidence of arthropathy (arthralgia, arthritis), mentioned previously, is referring to data collected in studies with adults. In children, arthropathy is reported to occur commonly (see Precautions).
Drugs known to prolong QT interval: Ciprofloxacin (Ciprobay), like other fluoroquinolones, should be used with caution in patients receiving drugs known to prolong the QT interval (e.g. Class IA and III anti-arrhythmics, tricyclic antidepressants, macrolides, antipsychotics) (see Precautions).
Probenecid: Probenecid interferes with renal secretion of ciprofloxacin. Co-administration of probenecid containing medicinal products and Ciprofloxacin (Ciprobay) increases the ciprofloxacin serum concentrations.
Tizanidine: In a clinical study in healthy subjects, there was an increase in tizanidine serum concentrations (Cmax increase: 7-fold, range: 4 to 21-fold; AUC increase: 10-fold, range: 6 to 24-fold) when given concomitantly with ciprofloxacin. Associated with the increased serum concentrations was a potentiated hypotensive and sedative effect (see Cytochrome P450 under Precautions). Tizanidine containing medicinal products must not be administered together with Ciprofloxacin (Ciprobay) (see Contraindications).
Theophylline: Concurrent administration of ciprofloxacin and theophylline containing medicinal products can cause an undesirable increase in the serum theophylline concentration. This can lead to theophylline-induced undesirable effects. In very rare cases, these undesirable effects can be life threatening or fatal.
If concurrent use of the two medicinal products is unavoidable, the serum theophylline concentration should therefore be checked and the theophylline dose appropriately reduced (see Cytochrome P450 under Precautions).
Other xanthine derivatives: On concurrent administration of ciprofloxacin and caffeine or pentoxifylline (oxpentifylline) containing products, raised serum concentrations of these xanthine derivatives were reported.
Phenytoin: Altered (decreased or increased) serum levels of phenytoin were observed in patients receiving Ciprofloxacin (Ciprobay) and phenytoin simultaneously. To avoid the loss of seizure control associated with decreased phenytoin levels, and to prevent phenytoin overdose-related undesirable effects when Ciprofloxacin (Ciprobay) is discontinued in patients receiving both agents, monitoring of phenytoin therapy, including phenytoin serum concentration measurements, is recommended during and shortly after co-administration of Ciprofloxacin (Ciprobay) with phenytoin.
Methotrexate: Renal tubular transport of methotrexate may be inhibited by concomitant administration of Ciprofloxacin (Ciprobay), potentially leading to increased plasma levels of methotrexate. This might increase the risk of methotrexate-associated toxic reactions. Therefore, patients under methotrexate therapy should be carefully monitored when concomitant Ciprofloxacin (Ciprobay) therapy is indicated.
NSAID: Animal studies have shown that the combination of very high doses of quinolones (gyrase inhibitors) and certain non-steroidal anti-inflammatory agents (but not acetylsalicylic acid) can provoke convulsions.
Cyclosporin: A transient rise in the concentration of serum creatinine was observed when ciprofloxacin and cyclosporin containing medicinal products were administered simultaneously. Therefore, it is frequently (twice a week) necessary to control the serum creatinine concentrations in these patients.
Vitamin K antagonists: Simultaneous administration of Ciprofloxacin (Ciprobay) with a vitamin K antagonist may augment its anticoagulant effects. The risk may vary with the underlying infection, age and general status of the patient so that the contribution of ciprofloxacin to the increase in INR (international normalized ratio) is difficult to assess. The INR should be monitored frequently during and shortly after co-administration of Ciprofloxacin (Ciprobay) with a vitamin K antagonist (e.g. warfarin, acenocoumarol, phenprocoumon, or fluindione).
Duloxetine: In clinical studies, it was demonstrated that concomitant use of duloxetine with strong inhibitors of the CYP450 1A2 isozyme such as fluvoxamine, may result in an increase of AUC and Cmax of duloxetine. Although no clinical data are available on a possible interaction with ciprofloxacin, similar effects can be expected upon concomitant administration (see Cytochrome P450 under Precautions).
Ropinirole: It was shown in a clinical study that concomitant use of ropinirole with ciprofloxacin, a moderate inhibitor of the CYP450 1A2 isozyme, results in an increase of Cmax and AUC of ropinirole by 60% and 84%, respectively. Monitoring ropinirole-related undesirable effects, dose adjustment as appropriate is recommended during and shortly after co-administration with Ciprofloxacin (Ciprobay) (see Cytochrome P450 under Precautions).
Lidocaine: It was demonstrated in healthy subjects that concomitant use of lidocaine containing medicinal products with ciprofloxacin, a moderate inhibitor of CYP450 1A2 isozyme, reduces clearance of intravenous lidocaine by 22%. Although lidocaine treatment was well tolerated, a possible interaction with ciprofloxacin associated with side effects may occur upon concomitant administration.
Clozapine: Following concomitant administration of 250 mg ciprofloxacin with clozapine for 7 days, serum concentrations of clozapine and N-desmethylclozapine were increased by 29% and 31%, respectively. Clinical surveillance and appropriate adjustment of clozapine dosage during and shortly after co-administration with Ciprofloxacin (Ciprobay) are advised (see Cytochrome P450 under Precautions).
Sildenafil: Cmax and AUC of sildenafil were increased approximately twofold in healthy subjects after an oral dose of 50 mg given concomitantly with 500 mg ciprofloxacin. Therefore, caution should be used prescribing Ciprofloxacin (Ciprobay) concomitantly with sildenafil taking into consideration the risks and the benefits.
Agomelatine: In clinical studies, it was demonstrated that fluvoxamine, as a strong inhibitor of the CYP450 1A2 isoenzyme, markedly inhibits the metabolism of agomelatine resulting in a 60-fold increase of agomelatine exposure. Although no clinical data are available for a possible interaction with ciprofloxacin, a moderate inhibitor of CYP450 1A2, similar effects can be expected upon concomitant administration (see Cytochrome P450 under Precautions).
Zolpidem: Co-administration of ciprofloxacin may increase blood levels of zolpidem, concurrent use is not recommended.
Film-coated tablet: Chelation complex formation: The simultaneous administration of Ciprofloxacin (Ciprobay) and multivalent cation-containing medicinal products and mineral supplements (e.g. calcium, magnesium, aluminum, iron), polymeric phosphate binders (e.g. sevelamer, lanthanum carbonate), sucralfate or antacids, and highly buffered drugs (e.g. didanosine tablets) containing magnesium, aluminum, or calcium reduce the absorption of ciprofloxacin. Consequently, Ciprofloxacin (Ciprobay) should be administered either 1-2 hours before or at least 4 hours after these preparations.
The restriction does not apply to antacids belonging to the class of H2 receptor blockers.
Food and dairy products: The concurrent administration of dairy products or mineral-fortified drinks alone (e.g. milk, yoghurt, calcium-fortified orange juice) and Ciprofloxacin (Ciprobay) should be avoided because absorption of ciprofloxacin may be reduced. Dietary calcium as part of a meal, however, does not significantly affect absorption.
Metoclopramide: Metoclopramide accelerates the absorption of ciprofloxacin resulting in a shorter time to reach maximum plasma concentrations. No effect was seen on the bioavailability of ciprofloxacin.
Omeprazole: Concomitant administration of ciprofloxacin and omeprazole containing medicinal products results in a slight reduction of Cmax and AUC of ciprofloxacin.
Instructions for use/ handling: Ciprofloxacin (Ciprobay) solution for infusion: At cool storage temperatures precipitation may occur, which will re-dissolve at room temperature. It is therefore recommended not to store the infusion solution in a refrigerator.
Incompatibilities: Film-coated tablet: None.
Solution for infusion: Ciprofloxacin (Ciprobay) solution for infusion (0.9% NaCl): Ciprofloxacin (Ciprobay) solution for infusion (0.9% NaCl) is compatible with physiological saline, Ringer solution and Ringer lactate solution, 5% and 10% glucose solutions, 10% fructose solution, and 5% glucose solution with 0.225% NaCl or 0.45% NaCl.
When Ciprofloxacin (Ciprobay) solutions for infusion (0.9% NaCl) are mixed with compatible solutions for infusion, for microbiological reasons and light sensitivity, these solutions should be administered shortly after admixture. Unless compatibility with other solutions for infusion/medicinal products has been confirmed, the solution for infusion must always be administered separately. The visual signs of incompatibility are e.g. precipitation, clouding, and discoloration.
Incompatibility appears with all solutions for infusion/medicinal products that are physically or chemically unstable at the pH of the solution (e.g. penicillins, heparin solutions), especially on combination with solutions adjusted to an alkaline pH (pH of the Ciprofloxacin (Ciprobay) solutions for infusion (0.9% NaCl: 3.9 - 4.5).
Film-coated Tablet: Store at temperatures not exceeding 25°C.
Ciprofloxacin (Ciprobay) solution for infusion: Store at temperatures not exceeding 30°C.
Protect from light. Do not refrigerate or freeze.
Remove the bottle from the box just before use.
Glass bottles (solution for infusion, 0.9% NaCl): For ease of use the infusion vial stopper should be penetrated in the central ring. Penetration of the outer ring may result in damage to the vial stopper.
J01MA02 - ciprofloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Ciprobay IV infusion 200 mg/100 mL
1's
Ciprobay IV infusion 400 mg/200 mL
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image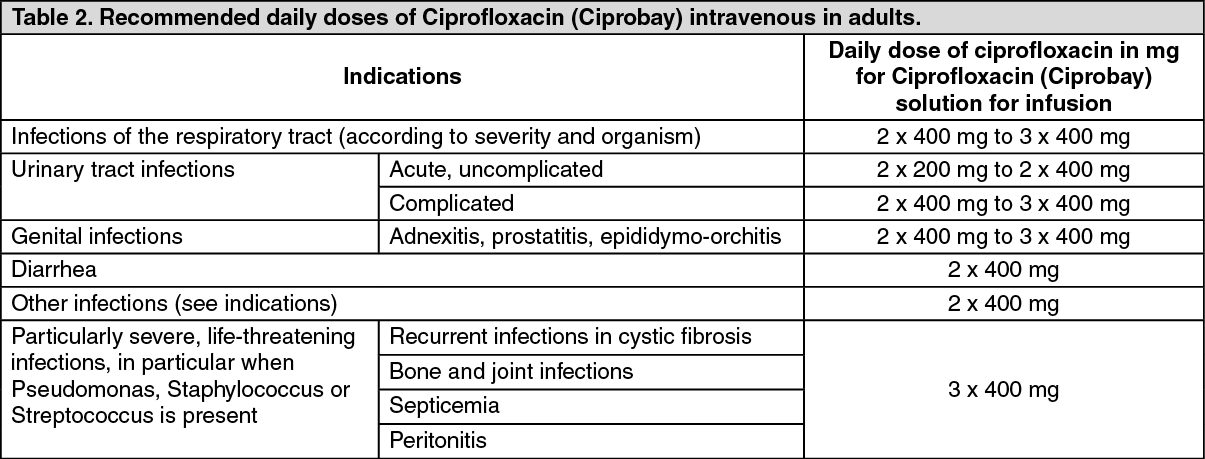 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image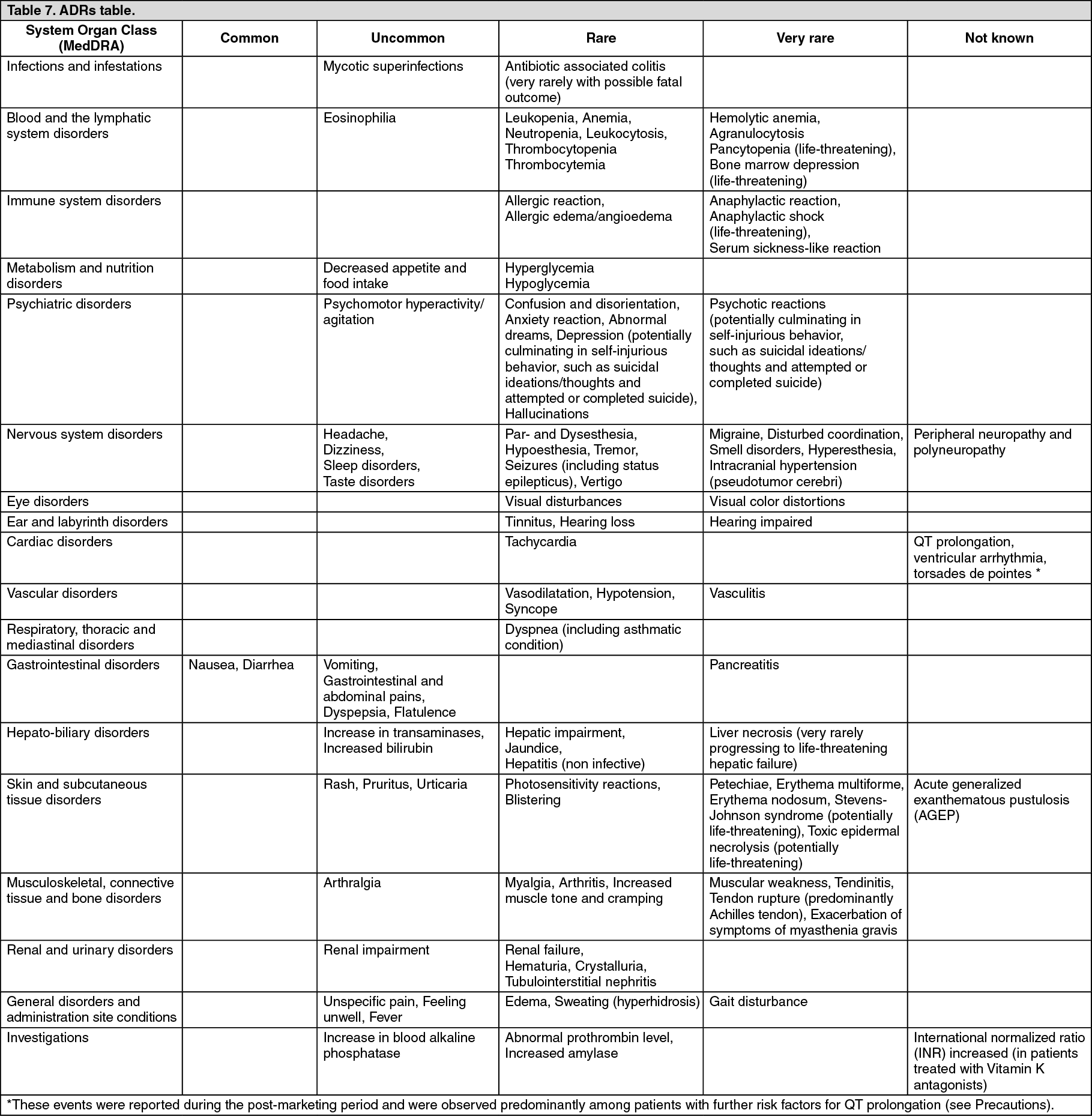 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
