Therapeutic/Pharmacologic Class of Drug: Selective Immunosuppressive agent (immunosuppressant) - Mycophenolic acid.
ATC Code: L04AA06.
Pharmacology: Pharmacodynamics: Mechanism of Action: Mycophenolate mofetil (MMF) is the 2-morpholinoethyl ester of mycophenolic acid (MPA). MPA is a potent, selective, uncompetitive and reversible inhibitor of inosine monophosphate dehydrogenase (IMPDH), and therefore inhibits the
de novo pathway of guanosine nucleotide synthesis. The mechanism by which MPA inhibits the enzymatic activity of IMPDH appears to be related to the ability of MPA to structurally mimic both nicotinamide adenine dinucleotide cofactor and a catalytic water molecule. This prevents the oxidation of IMP to xanthose-5'-monophosphate which is the committed step in
de novo guanosine nucleotide biosynthesis. Two IMPDH isoforms have been identified, isoform type I, which is present in most known cells (including resting human lymphocytes) and isoform type II, which is strongly and predominantly expressed in activated human B- and T-lymphocytes. The type II isoform is nearly five times more sensitive to inhibition by MPA than is the type I isoform. MPA has more potent cytostatic effects on lymphocytes than on other cells because T- and B-lymphocytes are critically dependent for their proliferation on
de novo synthesis of purines whereas other cell types can utilize salvage pathways.
In addition to its inhibition of IMPDH and the resulting deprivation of lymphocytes, MPA also influences cellular checkpoints responsible for metabolic programming of lymphocytes [198]. It has been shown, using human CD4+ T-cells, that MPA shifts transcriptional activities in lymphocytes from a proliferative state to catabolic processes relevant to metabolism and survival leading to an anergic state of T-cells, whereby the cells become unresponsive to their specific antigen.
Clinical/Efficacy Studies: Transplant studies: Mycophenolate mofetil (CellCept) has been administered in combination with the following agents in clinical trials for the prevention of renal, cardiac and hepatic rejection episodes: antithymocyte globulin, OKT3, ciclosporin and corticosteroids. Mycophenolate mofetil (CellCept) has also been administered in combination with ciclosporin and corticosteroids for the treatment of refractory renal rejection episodes. Prior to treatment with Mycophenolate mofetil (CellCept), patients may have also received antilymphocyte globulin, antithymocyte globulin and OKT3. Mycophenolate mofetil (CellCept) has further been used in clinical trials together with daclizumab and tacrolimus.
Prevention of organ rejection: Adults: The safety and efficacy of Mycophenolate mofetil (CellCept) in combination with corticosteroids and ciclosporin for the prevention of organ rejection were assessed in renal transplant patients in three randomized, double-blind, multicenter trials, in cardiac patients in one randomized double-blind, multicenter trial, and in hepatic patients in one randomized, double-blind, multicenter trial.
Children: The safety, pharmacokinetics and efficacy of Mycophenolate mofetil (CellCept) in combination with corticosteroids and ciclosporin for the prevention of organ rejection in pediatric renal transplant patients were assessed in an open-label, multicenter study in 100 patients (aged 3 months to 18 years).
Renal transplant: Adults: The three studies compared two dose levels of oral Mycophenolate mofetil (CellCept) (1 g twice daily and 1.5 g twice daily) with azathioprine (2 studies) or placebo (1 study) when administered in combination with ciclosporin and corticosteroids to prevent acute rejection episodes.
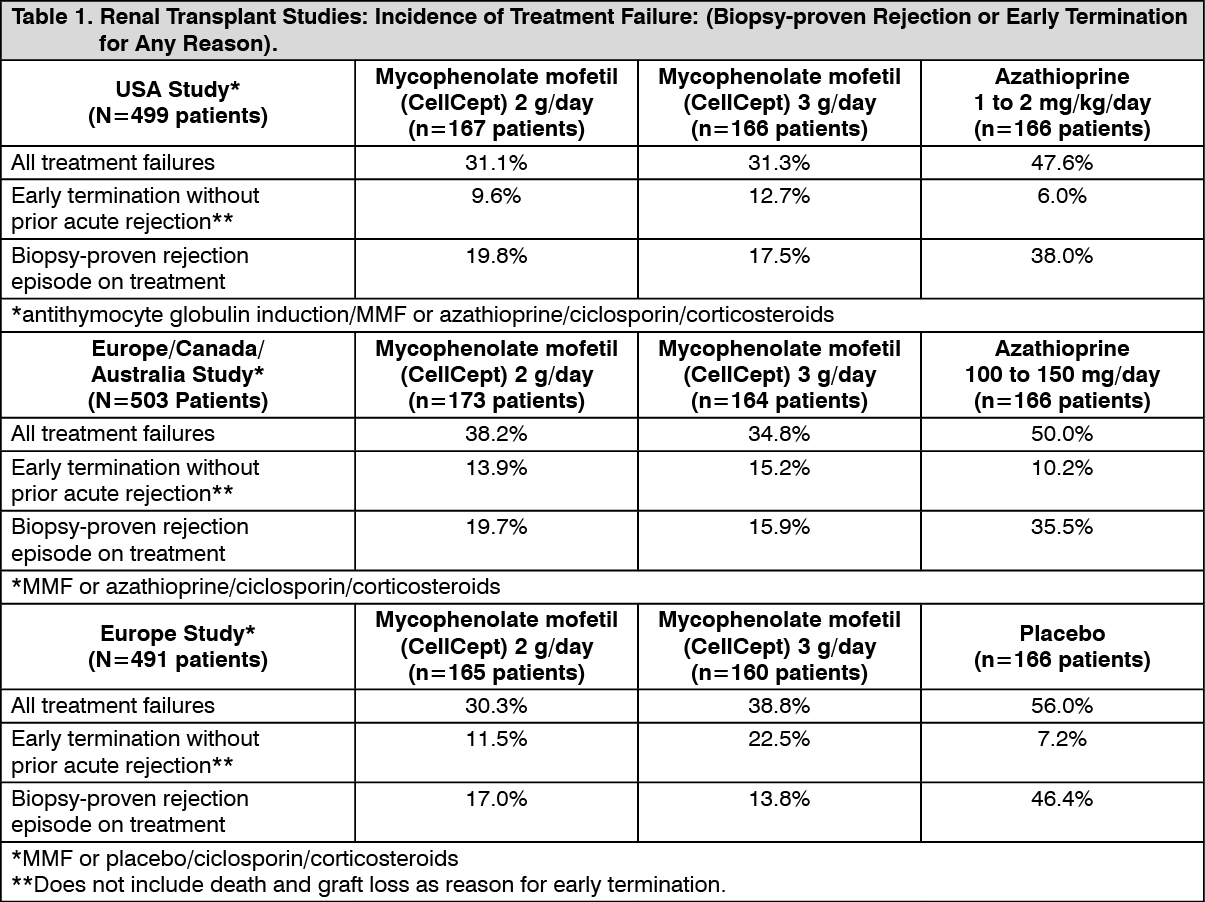
The primary efficacy endpoint was the proportion of patients in each treatment group who experienced treatment failure within the first 6 months after transplantation (defined as biopsy-proven acute rejection on treatment or the occurrence of death, graft loss or early termination from the study for any reason without prior biopsy-proven rejection). Mycophenolate mofetil (CellCept) was studied in the following three therapeutic regimens: (1) antithymocyte globulin induction/MMF or azathioprine/ciclosporin/corticosteroids, (2) MMF or azathioprine/ciclosporin/corticosteroids, and (3) MMF or placebo/ciclosporin/corticosteroids.
Mycophenolate mofetil (CellCept), in combination with corticosteroids and ciclosporin reduced (statistically significant at the <0.05 level) the incidence of treatment failure within the first 6 months following transplantation. The following tables summarize the results of these studies. Patients who prematurely discontinued treatment were followed for the occurrence of death or graft loss, and the cumulative incidence of graft loss and patient death are summarized separately. Patients who prematurely discontinued treatment were not followed for the occurrence of acute rejection after termination. More patients receiving Mycophenolate mofetil (CellCept) discontinued (without prior biopsy-proven rejection, death or graft loss) than discontinued in the control groups, with the highest rate in the Mycophenolate mofetil (CellCept) 3 g/day group. Therefore, the acute rejection rates may be underestimates, particularly in the Mycophenolate mofetil (CellCept) 3 g/day group. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Cumulative incidence of 12-month graft loss and patient death are presented as follows. No advantage of Mycophenolate mofetil (CellCept) with respect to graft loss and patient death was established. Numerically, patients receiving Mycophenolate mofetil (CellCept) 2 g/day and 3 g/day experienced a better outcome than controls in all three studies; patients receiving Mycophenolate mofetil (CellCept) 2 g/day experienced a better outcome than Mycophenolate mofetil (CellCept) 3 g/day in two of the three studies. Patients in all treatment groups who terminated treatment early were found to have a poor outcome with respect to graft loss and patient death at 1 year. (See Table 2.)
Click on icon to see table/diagram/image
Children (aged 3 months to 18 years): One open-label, safety, pharmacokinetics and efficacy study of Mycophenolate mofetil (CellCept) powder for oral suspension in combination with ciclosporin and corticosteroids for the prevention of renal allograft rejection was performed in 100 pediatric patients (aged 3 months to 18 years) at centers in the US (9), Europe (5) and Australia (1). Mycophenolate mofetil (CellCept) was dosed at 600 mg/m
2 twice daily (up to 1 g twice daily) in all age groups.
The primary efficacy endpoint was the proportion of patients experiencing an acute rejection episode in the first 6 months post-transplant. The rate of biopsy-proven rejection was similar across the age groups (3 months to <6 years, 6 years to <12 years, 12 years to 18 years). The overall biopsy-proven rejection rate at 6 months was comparable to adults. The combined incidence of graft loss (5%) and patient death (2%) at 12 months post-transplant was similar to that observed in adult renal transplant patients.
Cardiac transplant: A double-blind, randomized, comparative, parallel-group, multicenter study was performed in primary cardiac transplant recipients. The total number of patients enrolled was 650; 72 never received study drug and 578 received study drug. Patients received Mycophenolate mofetil (CellCept) 1.5 g twice daily (n=289) or azathioprine 1.5 to 3 mg/kg/day (n=289), in combination with ciclosporin and corticosteroids as maintenance immunosuppressive therapy. The two primary efficacy endpoints were: (1) the proportion of patients who, after transplantation, had at least one endomyocardial biopsy-proven rejection with hemodynamic compromise, or were retransplanted or died, within the first 6 months, and (2) the proportion of patients who died or were transplanted during the first 12 months following transplantation. Patients who prematurely discontinued treatment were followed for the occurrence of allograft rejection for up to 6 months and for the occurrence of death for 1 year.
1. Rejection: No difference was established between Mycophenolate mofetil (CellCept) and azathioprine (AZA) with respect to biopsy-proven rejection with hemodynamic compromise, as presented as follows. (See Table 3.)
Click on icon to see table/diagram/image
2. Survival: In the enrolled patients, there were no statistically significant differences between patients randomized to MMF and patients randomized to AZA for death and retransplantation. In patients who received study drug, the lower limit of the 97.5% confidence interval of the difference of death and retransplantation was 0.9 at 1 year, indicating that MMF was superior to AZA in these patients, as presented as follows. (See Table 4.)
Click on icon to see table/diagram/image
Hepatic transplant: A double-blind, randomized, comparative, parallel-group, multicenter study in primary hepatic transplant recipients was performed at 16 centers in the United States, 2 in Canada, 4 in Europe and 1 in Australia. The total number of patients enrolled was 565 and 564 received study drug. Patients either received Mycophenolate mofetil (CellCept) 1g twice daily intravenously for up to 14 days followed by Mycophenolate mofetil (CellCept) 1.5 g twice daily orally or azathioprine 1-2 mg/kg/day intravenously followed by azathioprine 1-2 mg/kg/day orally, in combination with ciclosporin and corticosteroids as maintenance immunosuppressive therapy. The two primary endpoints were: (1) the proportion of patients who experienced, in the first 6 months post transplantation, one or more episodes of biopsy-proven and treated rejection or death/retransplantation, and (2) the proportion of patients who experienced graft loss (death/retransplantation) during the first 12 months post transplantation. Patients who prematurely discontinued treatment were followed for the occurrence of allograft rejection and for the occurrence of graft loss (death/retransplantation) for 1 year.
Results: In the primary (intent-to-treat) analyses Mycophenolate mofetil (CellCept) in combination with corticosteroids and ciclosporin was superior to azathioprine for prevention of acute rejection (p = 0.025) and equivalent to azathioprine for survival. (See Table 5.)
Click on icon to see table/diagram/image
Treatment of refractory organ rejection: A randomized, open-label comparison study of MMF 3g per day against intravenous corticosteroids was conducted in 150 renal transplant recipients with refractory, acute, cellular allograft rejection. The primary endpoint was the proportion of patients who were still alive with a functioning graft at 6 months after study entry.
Results: The incidence of graft loss in the control group was unexpectedly low and the primary analysis, based on the sequential probability ratio test showed a trend toward improved graft survival in the MMF group (p=0.081). A secondary analysis, using the Cochran-Mantel-Haenszel test (not adjusted for sequential monitoring) suggested a 45% reduction in the incidence of graft loss or death at 6 months after study entry in the MMF arm (p=0.062). (See Table 6.)
Click on icon to see table/diagram/image
Lupus nephritis studies: Many studies have investigated the use of Mycophenolate mofetil (CellCept) for induction and maintenance therapy of lupus nephritis. Two large meta-analyses provide the most robust evidence to support the use of MMF in the management of lupus nephritis: The Cochrane Collaboration reviewed 50 randomized controlled trials including 2846 adults and children with biopsy-proven lupus nephritis Class III-V receiving immunosuppressive therapy. MMF with corticosteroids was found to be as effective as IV cyclophosphamide with corticosteroids in preventing death, inducing complete remission in proteinuria and achieving stable kidney function at six months with lower rates of toxicity. In maintenance therapy, MMF with corticosteroids was more effective than AZA with corticosteroids at preventing relapse with no difference in clinically important side effects.
The National Kidney Foundation reviewed 53 randomized trials including 4,222 adults and children (from 10 years of age) with proliferative lupus nephritis receiving immunosuppressive therapy. Thirty-eight of the trials in the Cochrane review were also included in this meta-analysis. MMF with corticosteroids was as effective as IV cyclophosphamide with corticosteroids for inducing remission in lupus nephritis with improved tolerability. MMF with corticosteroids was superior to AZA with corticosteroids for maintaining disease remission.
The results of these meta-analyses are in line with the results of the largest randomized controlled study in lupus nephritis, the Aspreva Lupus Management Study (ALMS), which was a two-phase study investigating the efficacy of Mycophenolate mofetil (CellCept) in induction and maintenance therapy of patients with Class III-V lupus nephritis. In the induction phase of the study, patients were randomly assigned to a target dose of 3 g/day Mycophenolate mofetil (CellCept) or 0.5 to 1.0 g/m
2/month IV cyclophosphamide for 6 months. Both groups received prednisone, tapered from a maximum starting dose of 60 mg/day. There was no significant difference in the number of patients who met the primary endpoint of a pre-specified decrease in urine protein/creatinine ratio and stabilization or improvement in serum creatinine, supporting the finding of the meta-analyses that Mycophenolate mofetil (CellCept) is as effective as IV cyclophosphamide for induction therapy. In the 36-month maintenance phase of the study, the primary endpoint was the time to treatment failure measured as the time until the first event which was defined as death, end-stage renal disease, sustained doubling of the serum creatinine level, renal flare, or the need for rescue therapy. Mycophenolate mofetil (CellCept) (2 g/day) was superior to AZA (2 mg/kg/day) in time to treatment failure (hazard ratio, 0.44; 95% confidence interval, 0.25 to 0.77; P = 0.003), supporting the finding of the meta-analyses that MMF is more effective than azathioprine at preventing relapse.
Immunogenicity: No data available.
Pharmacokinetics: The pharmacokinetics of MMF have been studied in renal, cardiac and hepatic transplant patients and in patients with lupus nephritis.
In general, the pharmacokinetic profile of MPA is similar in renal and in cardiac transplant patients. In the early transplant period, hepatic transplant patients receiving a 1.5 g oral MMF dose or 1 g i.v. MMF dose have similar MPA levels compared to renal transplant patients receiving 1 g oral or i.v. MMF. The pharmacokinetic profile of MPA in lupus nephritis is similar to that reported in transplantation (including the high variability in exposure to active drug observed) but is complicated by more unpredictable changes in renal function in lupus nephritis patients.
Absorption: Following oral and intravenous administration, mycophenolate mofetil undergoes rapid and extensive absorption and complete presystemic metabolism to the active metabolite, MPA. The mean bioavailability of oral mycophenolate mofetil, based on MPA AUC, is 94% relative to i.v. mycophenolate mofetil. Mycophenolate mofetil can be measured systemically during intravenous infusion; however, after oral administration it is below the limit of quantitation (0.4 μg/mL).
Immediately post-transplant (<40 days) renal, cardiac and hepatic transplant patients had mean MPA AUCs approximately 30% lower and Cmax approximately 40% lower compared to the late transplant period (3-6 months post transplant). This is referred to as non-stationarity of MPA pharmacokinetics. MPA AUC values obtained following administration of 1 g twice daily intravenous Mycophenolate mofetil (CellCept) at the recommended infusion rate to renal patients in the immediate post-transplant phase are comparable to those observed following oral dosing. In hepatic transplant patients, administration of 1 g twice daily intravenous Mycophenolate mofetil (CellCept) followed by 1.5 g twice daily oral Mycophenolate mofetil (CellCept) resulted in MPA AUC values similar to those found in renal transplant patients administered 1 g Mycophenolate mofetil (CellCept) twice daily.
Food had no effect on the extent of absorption (MPA AUC) of mycophenolate mofetil administered at doses of 1.5 g twice daily to renal transplant patients. However, MPA C
max was decreased by 40% in the presence of food.
Equivalence of oral dosage forms: Bioequivalence of Mycophenolate mofetil (CellCept) oral dosage forms have been evaluated. Two 500 mg tablets have been shown to be bioequivalent to four 250 mg capsules. Likewise, 1 g/5 mL of Mycophenolate mofetil (CellCept) constituted powder for oral suspension has been shown to be bioequivalent to four 250 mg capsules (see Dosage & Administration).
Distribution: Secondary increases in plasma MPA concentrations are usually observed at approximately 6-12 hours post-dose, consistent with enterohepatic recirculation. A reduction of approximately 40% in the AUC of MPA is associated with coadministration of cholestyramine (4 g three times daily), consistent with interruption of enterohepatic recirculation.
At clinically relevant concentrations, MPA is 97% bound to plasma albumin. This value is dependent on renal function; changes in albumin binding after initiating therapy may explain the non-stationarity in the pharmacokinetics of MPA.
Metabolism: MPA is conjugated primarily by glucuronyltransferase (isoform UGT1A9) to form the inactive phenolic glucuronide of MPA (MPAG).
In vivo, MPAG is converted back to free MPA via enterohepatic recirculation. A minor acylglucuronide (AcMPAG) is also formed. AcMPAG is pharmacologically active and is suspected to be responsible for some of MMF's side effects (diarrhea, leucopenia).
Elimination: Oral administration of radiolabelled mycophenolate mofetil resulted in complete recovery of the administered dose, with 93% of the dose recovered in the urine and 6% recovered in the feces. Most (about 87%) of a dose is excreted in the urine as MPAG. A negligible amount of drug (<1% of dose) is excreted as MPA in the urine.
Enterohepatic recirculation interferes with accurate determination of MPA's disposition parameters; only apparent values can be indicated. In healthy volunteers and patients with autoimmune disease approximate clearance values of 10.6 L/h and 8.27 L/h respectively and half-life values of 17 h were observed. In transplant patients mean clearance values were higher (range 11.9-34.9 L/h) and mean half-life values shorter (5-11 h) with little difference between renal, hepatic or cardiac transplant patients. In the individual patients, these elimination parameters vary based on type of co-treatment with other immunosuppressants, time post-transplantation, plasma albumin concentration and renal function. These factors explain why reduced exposure is seen when Mycophenolate mofetil (CellCept) is co-administered with cyclosporine (see Interactions) and why plasma concentrations tend to increase over time compared to what is observed immediately after transplantation (see non-stationarity in Absorption and Distribution as previously mentioned).
At clinically encountered concentrations, MPA and MPAG are not removed by hemodialysis. However, at high MPAG concentrations (>100 μg/mL), small amounts of MPAG are removed. By interfering with enterohepatic circulation of the drug, bile acid sequestrants, such as cholestyramine, reduce MPA AUC (see Overdosage).
MPA's disposition depends on several transporters. Organic anion-transporting polypeptides (OATPs) and multidrug resistance-associated protein 2 (MRP2) are involved in MPA's disposition; OATP isoforms, MRP2 and breast cancer resistance protein (BCRP) are transporters associated with the glucuronides' biliary excretion. Multidrug resistance protein 1 (MDR1) is also able to transport MPA, but its contribution seems to be confined to the absorption process. In the kidney MPA and its metabolites potently interact with renal organic anion transporters.
Pharmacokinetics in Special Populations: Renal impairment: In a single-dose study (6 subjects per group), mean plasma MPA AUCs observed after oral dosing in subjects with severe chronic renal impairment (glomerular filtration rate <25 mL/min/1.73 m
2) were 28-75% higher than those observed in normal healthy subjects or subjects with lesser degrees of renal impairment. The mean single-dose MPAG AUC was 3- to 6-fold higher in subjects with severe renal impairment than in subjects with mild renal impairment and normal healthy subjects, consistent with the known renal elimination of MPAG.
Multiple dosing of mycophenolate mofetil in patients with severe chronic renal impairment has not been studied.
There is also a paucity of information available for lupus nephritis patients with severe renal impairment. Therapeutic drug monitoring in lupus nephritis patients with GFR <30 mL/min is advisable.
Patients with delayed renal graft function post-transplant: In patients with delayed renal graft function post-transplant, mean MPA AUC
0-12 was comparable to that seen in post-transplant patients without delayed renal graft function. There may be a transient increase in the free-fraction and concentration of plasma MPA in patients with delayed renal graft function. Dose adjustment of Mycophenolate mofetil (CellCept) does not appear to be necessary (see Special Dosage Instructions under Dosage & Administration). Mean plasma MPAG AUC
0-12 was 2- to 3-fold higher than in post-transplant patients without delayed renal graft function.
In patients with primary non-functioning graft following renal transplantation, plasma concentrations of MPAG accumulated; accumulation of MPA, if any, was much smaller.
Hepatic impairment: Overall, the pharmacokinetics of MPA and MPAG were relatively unaffected by hepatic parenchymal disease in volunteers with alcoholic cirrhosis dosed with oral or intravenous MMF. Effects of hepatic disease on these processes probably depend on the particular disease. Hepatic disease with predominantly biliary damage, such as primary biliary cirrhosis, may show a different effect.
Pediatric Population (aged ≤18 years): Pharmacokinetic parameters were evaluated in 55 pediatric renal transplant patients (ranging from 1 year to 18 years of age) given 600 mg/m
2 mycophenolate mofetil orally twice daily (up to a maximum of 1 g twice daily). This dose achieved MPA AUC values similar to those seen in adult renal transplant patients receiving Mycophenolate mofetil (CellCept) at a dose of 1 g twice daily in the early and late post-transplant period. MPA AUC values across age groups were similar in the early and late post-transplant period.
Pharmacokinetics have not been formally evaluated in pediatric lupus nephritis patients. However, in patients with systemic lupus erythematosus (some with renal involvement), similar typical MPA AUC
0-12 values following MMF administration were observed in children, adolescent, and adult patients.
Geriatric Population (≥ 65 years): The pharmacokinetics of mycophenolate mofetil and its metabolites have not been found to be altered in geriatric transplant patients when compared to younger transplant patients.
Toxicology: Nonclinical Safety: The hematopoietic and lymphoid systems were the primary organs affected in toxicology studies conducted with mycophenolate mofetil in the rat, mouse, dog and monkey. These effects occurred at systemic exposure levels that are equivalent to or less than the clinical exposure at the recommended dose of 2 g/day for renal transplant recipients. Gastrointestinal effects were observed in the dog at systemic exposure levels equivalent to or less than the clinical exposure at the recommended doses. Gastrointestinal and renal effects consistent with dehydration were also observed in the monkey at the highest dose (systemic exposure levels equivalent to or greater than clinical exposure). The nonclinical toxicity profile of mycophenolate mofetil appears to be consistent with adverse events observed in human clinical trials which now provide safety data of more relevance to the patient population (see Adverse Reactions).
Carcinogenicity: In experimental models, mycophenolate mofetil was not tumorigenic. The highest dose tested in the animal carcinogenicity studies resulted in approximately 2-3 times the systemic exposure (AUC or C
max) observed in renal transplant patients at the recommended clinical dose of 2 g/day and 1.3-2 times the systemic exposure (AUC or C
max) observed in cardiac transplant patients at the recommended clinical dose of 3 g/day.
Genotoxicity: Two genotoxicity assays (the mouse lymphoma/thymidine kinase assay and the mouse micronucleus aberration assay) indicated a potential of mycophenolate mofetil to cause chromosomal instability at severely cytotoxic dose levels. Other genotoxicity tests (the bacterial mutation assay, the yeast mitotic gene conversion assay or the Chinese hamster ovary cell chromosomal aberration assay) did not demonstrate mutagenic activity.
Impairment of Fertility: Mycophenolate mofetil had no effect on fertility of male rats at oral doses up to 20 mg/kg/day. The systemic exposure at this dose represents 2 to 3 times the clinical exposure at the recommended clinical dose of 2 g/day in renal transplant patients and 1.3-2 times the clinical exposure at the recommended clinical dose of 3 g/day in cardiac transplant patients. In a female fertility and reproduction study conducted in rats, oral doses of 4.5 mg/kg/day caused malformations (including anophthalmia, agnathia, and hydrocephaly) in the first generation offspring in the absence of maternal toxicity. The systemic exposure at this dose was approximately 0.5 times the clinical exposure at the recommended clinical dose of 2 g/day for renal transplant patients and approximately 0.3 times the clinical exposure at the recommended clinical dose of 3 g/day for cardiac transplant patients. No effects on fertility or reproductive parameters were evident in the dams or in the subsequent generation.
Reproductive Toxicity: In teratology studies in rats and rabbits, fetal resorptions and malformations occurred in rats at 6 mg/kg/day (including anophthalmia, agnathia, and hydrocephaly) and in rabbits at 90 mg/kg/day (including cardiovascular and renal anomalies, such as ectopia cordis and ectopic kidneys, and diaphragmatic and umbilical hernia), in the absence of maternal toxicity. The systemic exposure at these levels are approximately equivalent to or less than 0.5 times the clinical exposure at the recommended clinical dose of 2 g/day for renal transplant patients and approximately 0.3 times the clinical exposure at the recommended clinical dose of 3 g/day for cardiac transplant patients.
Refer to Pregnancy under Use in Pregnancy & Lactation.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image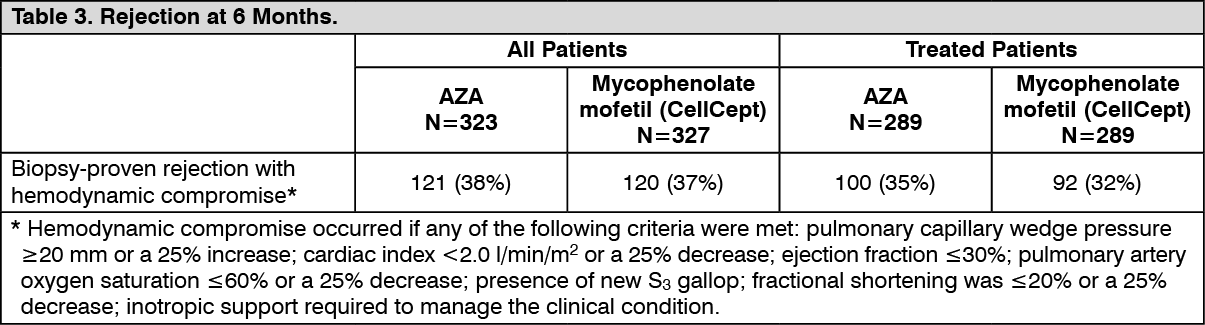 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image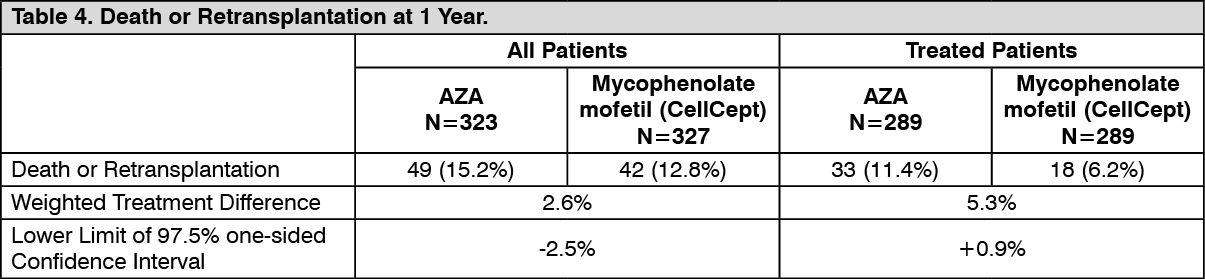 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image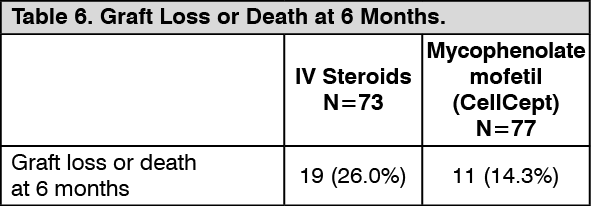 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image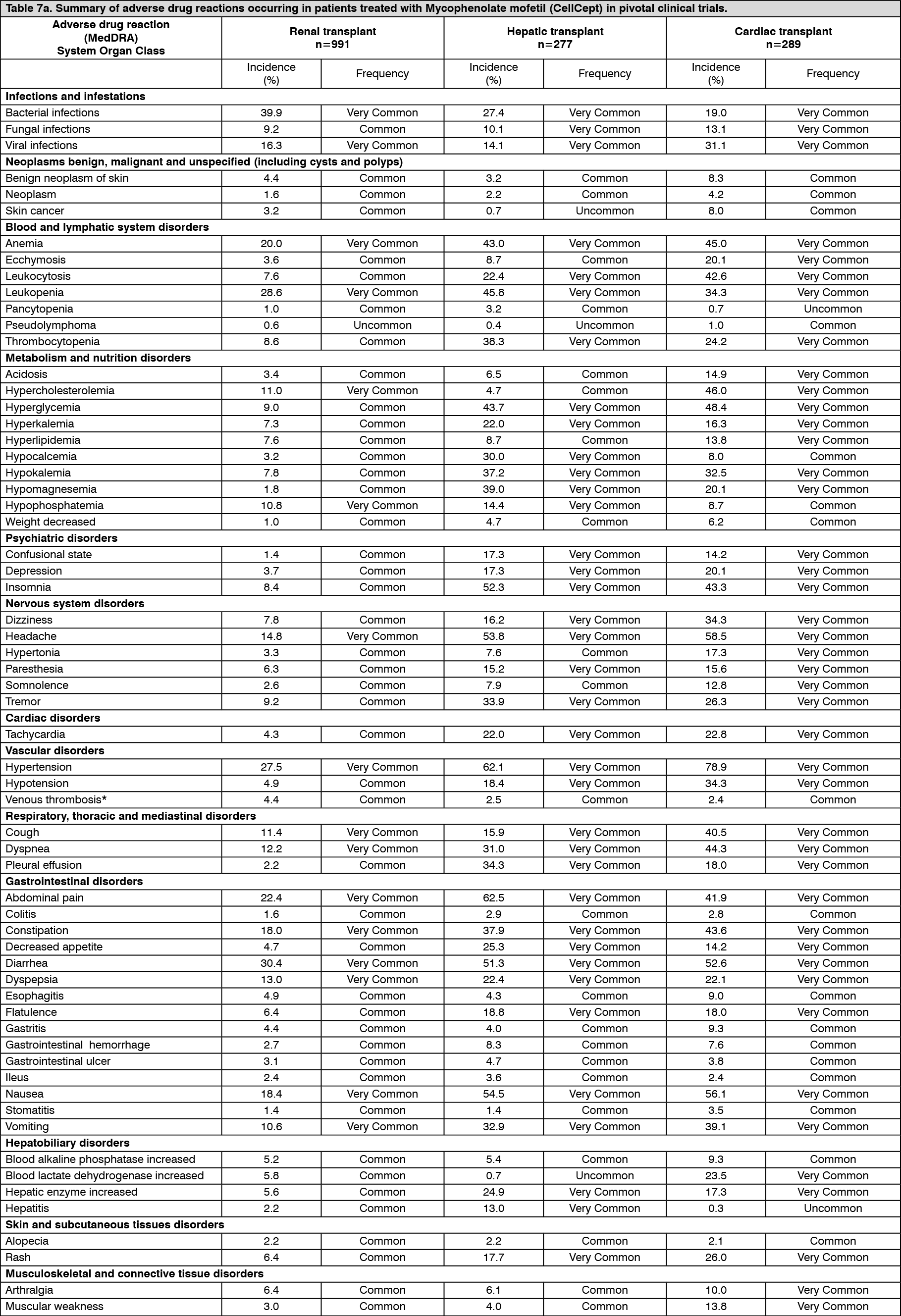 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image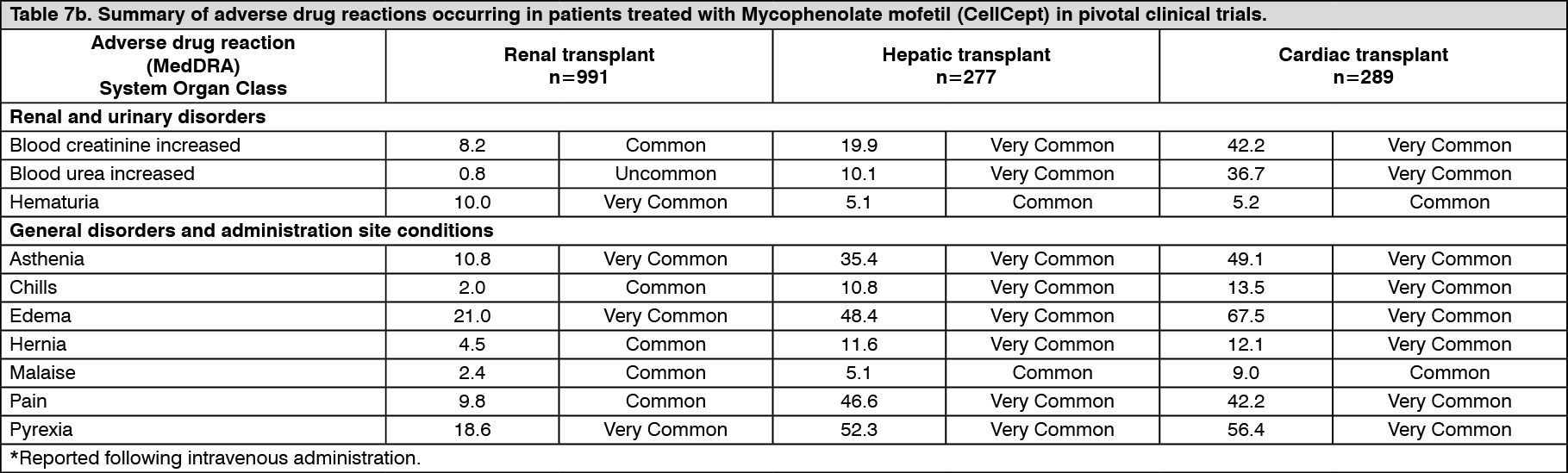 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
