Adult: 300 mg once daily, given w/ ritonavir 100 mg. Alternatively, for treatment-naive patient: 400 mg once daily (if patient cannot tolerate ritonavir). Child: ≥3 mth As powd: 5-<15 kg: 200 mg once daily, given w/ ritonavir 80 mg; 15-<25 kg: 2250 mg once daily, given w/ ritonavir 80 mg. >6 yr As cap/powd: 15-<20 kg: 150 mg once daily, given w/ ritonavir 100 mg; 20-<40 kg: 200 mg once daily, given w/ ritonavir 100 mg; ≥40 kg: Same as adult dose.
Renal Impairment
Treatment-experienced patient on haemodialysis: Contraindicated.
Perform LFTs before and during treatment. Monitor viral load, CD4, blood lipids and glucose, and bilirubin. Monitor ECG esp in patient w/ pre-existing prolonged PR interval.
Overdosage
Symptoms: Jaundice, hyperbilirubinaemia, asymptomatic bifascicular block, PR interval prolongation. Management: Supportive treatment. Induce emesis or employ gastric lavage; activated charcoal may also be given.
Drug Interactions
Decreased concentration w/ PPIs, efavirenz, nevirapine, and rifampicin. May increase serum concentration of inhaled fluticasone and salmeterol. Potentially Fatal: Increased risk for myopathy (i.e. rhabdomyolysis) w/ simvastatin and lovastatin. Increased risk for cardiac arrhythmia w/ cisapride. May increase risk of hypotension w/ alfuzosin. May increase potential of serious AR of amiodarone, bepridil, quinidine, and systemic lidocaine. May increase serum concentration of astemizole, terfenadine, pimozide, quetiapine, dihydroergotamine, ergometrine, ergotamine, methylergometrine, triazolam, and oral midazolam. May increase risk for hypotension, visual changes, and priapism w/ sildenafil (when used for pulmonary arterial HTN). May inhibit UGT1A1 causing an increase toxicity of irinotecan. May cause indirect hyperbilirubinaemia w/ indinavir.
Food Interaction
Enhanced absorption w/ food. Decreased concentration w/ St John’s wort.
Action
Description: Mechanism of Action: Atazanavir, a synthetic azapeptide, is a selective, competitive, and reversible HIV-1 protease inhibitor. It inhibits the cleavage of viral Gag and Gag-Pol polyprotein precursors into individual functional proteins, preventing the processing of the polyproteins into mature and infectious virions. Pharmacokinetics: Absorption: Rapidly absorbed from the GI tract. Enhanced absorption w/ food. Time to peak plasma concentration: Approx 2-2.5 hr. Distribution: Distributed in the CSF and semen in low concentration. Plasma protein binding: 86%, w/ similar affinity to albumin and α1-acid glycoprotein. Metabolism: Extensively metabolised in the liver by CYP3A4 enzyme, mainly via mono-oxygenation and deoxygenation into inactive metabolites; also undergoes glucuronidation, N-dealkylation, hydrolysis, and oxygenation w/ dehydrogenation into 2 minor inactive metabolites. Excretion: Via faeces (79%, 20% as unchanged drug) and urine (13%, 7% as unchanged drug). Terminal elimination half-life: Approx 7 hr.
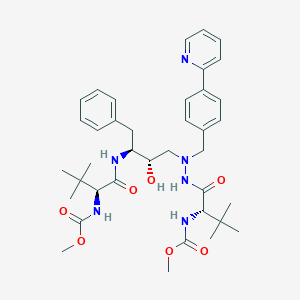
Chemical Structure
Atazanavir Source: National Center for Biotechnology Information. PubChem Database. Atazanavir, CID=148192, https://pubchem.ncbi.nlm.nih.gov/compound/Atazanavir (accessed on Jan. 21, 2020)
J05AE08 - atazanavir ; Belongs to the class of protease inhibitors. Used in the systemic treatment of viral infections.
References
Anon. Atazanavir. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 12/10/2016.Buckingham R (ed). Atazanavir Sulfate. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 12/10/2016.Joint Formulary Committee. Atazanavir. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 12/10/2016.McEvoy GK, Snow EK, Miller J et al (eds). Atazanavir Sulfate. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 12/10/2016.Reyataz Capsule, Gelatin Coated (A-S Medication Solutions). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 12/10/2016.



 Sign Out
Sign Out