


 Sign Out
Sign Out

Pharmacology: Inhibits cell wall mucopeptide synthesis.
Pharmacokinetics: Absorptions: Oral Bioavailability: Maximal plasma cefdinir concentrations occur 2 to 4 hours postdose following capsule or suspension administration. Plasma cefdinir concentrations increase with dose, but the increases are less than dose-proportional from 300 mg (7 mg/kg) to 600 mg (14 mg/kg). Following administration of suspension to healthy adults, cefdinir bioavailability is 120% relative to capsules. Estimated bioavailability of cefdinir capsules is 21% following administration of a 300 mg capsule dose, and 16% following administration of a 600mg capsule dose. Estimated absolute bioavailability of cefdinir suspension is 25%. Cefdinir oral suspension of 250 mg/5ml strength was shown to be bioequivalent to the 125mg/5 ml strength in healthy adults under fasting conditions.
Effect of Food: The Cmax and AUC of cefdinir from the capsules are reduced by 16% and 10%, respectively, when given with a high-fat meal. In adults given the 250mg/5ml oral suspension with a high-fat meal, the Cmax and AUC of cefdinir are reduced by 44% and 33%, respectively. The magnitude of these reductions is not likely to be clinically significant because the safely and efficacy studies of oral suspension in pediatric patients were conducted without regard to food intake. Therefore, cefdinir may be taken without regard to food.
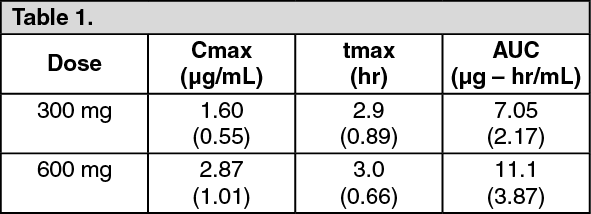
Cefdinir Capsules: Cefdinir plasma concentrations and pharmacokinetic parameter values following administration of single 300- and 600-mg oral doses of cefdinir to adult subjects are presented in the following table. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMultiple Dosing: Cefdinir does not accumulate in plasma following once- or twice-daily administration to subjects with normal renal function.
Distribution: The mean volume of distribution (Vdarea) of cefdinir in adult subjects is 0.35 L/kg (± 0.29); in pediatric subjects (age 6 months - 12 years), cefdinir Vdarea is 0.67 L/kg (± 0.38). Cefdinir is 60% to 70% bound to plasma proteins in both adult and pediatric subjects; binding is independent of concentration.
Skin Blister: In adult subjects, median (range) maximal blister fluid cefdinir concentrations of 0.65 (0.33-1.1) and 1.1 (0.49-1.9) μg/mL were observed 4 to 5 hours following administration of 300- and 600-mg doses, respectively. Mean (±SD) blister Cmax and AUC (0 - x) values were 48% (±13) and 91% (± 18) of corresponding plasma values.
Tonsil Tissue: In adult patients undergoing elective tonsillectomy, respective median tonsil tissue cefdinir concentrations 4 hours after administration of single 300- and 600-mg doses were 0.25 (0.22-0.46) and 0.36 (0.22-0.80) μg/g. Mean tonsil tissue concentrations were 24% (± 8) of corresponding plasma concentrations.
Sinus Tissue: In adult patients undergoing elective maxillary and ethmoid sinus surgery, respective median tissue cefdinir concentrations 4 hours after administration of single 300- and 600-mg doses were < 0.12. (<0.12-2.0) μg/g. Mean sinus tissue concentrations were 16% (±20) of corresponding plasma concentrations.
Lung Tissue: In adult patients undergoing diagnostic bronchoscopy, respective median bronchial mucosa cefdinir concentrations 4 hours after administration of single 300- and 600-mg doses were 0.78 (< 0.06-1.33) and 1.14 (< 0.06 - 1.92) μg/mL, and were 31% (± 18) of corresponding plasma concentrations. Respective median epithelial lining fluid concentrations were 0.29 (< 0.3-4.73) and 0.49 (< 0.3-0.59) μg/ml, and were 35% (± 83) of corresponding plasma concentrations.
Middle Ear Fluid: In 14 pediatric patients with acute bacterial otitis media, respective median middle ear fluid cefdinir concentrations 3 hours after administration of single 7- and 14-mg/kg doses were 0.21 (< 0.09-0.94) and 0.72 (0.14-1.42) μg/ml. Mean middle ear fluid concentrations were 15% (± 15) of corresponding plasma concentrations.
CSF: Data on cefdinir penetration into human cerebrospinal fluid are not available.
Metabolism and Excretion: Cefdinir is not appreciably metabolized. Activity is primarily due to parent drug. Cefdinir is eliminated principally via renal excretion with a mean plasma elimination half-life (t½) of 1.7 (± 0.6) hours. In healthy subjects with normal renal function, renal clearance is 2.0 (± 1.0) mL/min/kg, and apparent oral clearance is 11.6 (± 6.0) and 15.5 (± 5.4) mL/min/kg following doses of 300- and 600-mg, respectively. Mean percent of dose recovered unchanged in the urine following 300- and 600-mg doses is 18.4% (± 6.4) and 11.6% (± 4.6), respectively. Cefdinir clearance is reduced in patients with renal dysfunction. Because renal excretion is the predominant pathway of elimination, dosage should be adjusted in patients with markedly compromised renal function or who are undergoing hemodialysis.
Special Populations: Patients with Renal Insufficiency: Cefdinir pharmacokinetics were investigated in 21 adult subjects with varying degrees of renal function. Decreases in cefdinir elimination rate, apparent oral clearance (CL/F), and renal clearance were approximately proportional to the reduction in creatinine clearance (Cl cr). As a result, plasma cefdinir concentrations were higher and persisted longer in subjects with renal impairment than in those without renal impairment. In subjects with CL cr between 30 and 60 mL/min, Cmax and t½ increased by approximately 2-fold and AUC by approximately 3-fold. In subjects with Cl cr < 30 mL/min, Cmax increased by approximately 2-fold. t½ by approximately 5-fold, and AUC by approximately 6-fold. Dosage adjustment is recommended in patients with markedly compromised (renal) function (creatinine clearance < 30 mL/min).
Hemodialysis: Cefdinir pharmacokinetics were studied in 8 adult subjects undergoing hemodialysis. Dialysis (4 hours duration) removed 63% of cefdinir from the body and reduced apparent elimination t½ from 16 (± 3.5) to 3.2 (± 1.2) hours. Dosage adjustment is recommended in this patient population.
Hepatic Disease: Because cefdinir is predominantly renally eliminated and not appreciably metabolized, studies in patients with hepatic impairment were not conducted. It is not expected that dosage adjustment will be required in this population.
Geriatric Patients: The effect of age on cefdinir pharmacokinetics after a single 300-mg dose was evaluated in 32 subjects 19 to 91 years of age. Systemic exposure to cefdinir was substantially increased in older subjects (N = 16), Cmax by 44% and AUC by 86%. This increase was due to a reduction in cefdinir clearances. The apparent volume od distribution was also reduced, thus no appreciable alterations in apparent elimination t½ were observed (elderly : 2.2 ± 0.6 hours vs young: 1.8 ± 0.4 hours). Since clearance has been shown to be primarily related to changes in renal function rather than age, elderly patients do not require dosage adjustment unless they have markedly compromised renal function (creatinine clearance < 30mL/min).
Gender and Race: The results of a meta-analysis of clinical pharmacokinetics (N = 217) indicated no significant impact of either gender or race on cefdinir pharmacokinetics.