Teriparatide [r-human parathyroid hormone (1-34)].
Each ml of TERIPARATIDE (r-Human Parathyroid Hormone) (1-34) Injection contains: Recombinant human Parathyroid Hormone (1-34) IHS 250 mcg, Succinic acid USP 0.29 mg, Sodium Hydroxide USP 0.05 mg, Glycerol USP 50 mg, M-Cresol USP 3 mg, Water for Injection USP q.s.
Teriparatide (rDNA origin) contains recombinant human parathyroid hormone (1-34), and is also called rhPTH (1-34). It has an identical sequence to the 34 N-terminal amino acids (the biologically active region) of the 84-amino acid human parathyroid hormone.
Teriparatide has a molecular weight of 4117.8 daltons.
Teriparatide (rDNA origin) is manufactured using a strain of Escherichia coli modified by recombinant DNA technology.
Excipients/Inactive Ingredients: Succinic acid USP/NF, Sodium hydroxide USP/NF, Glycerol USP/NF, m-cresol USP/NF, Water for injection USP/NF.
Pharmacology: Mechanism of Action: Endogenous 84-amino acid parathyroid hormone (PTH) is the primary regulator of calcium and phosphate metabolism in bone and kidney. Teriparatide is the active fragment (1-34) of endogenous human parathyroid hormone. Physiological actions of PTH include stimulation of bone formation by direct effects on bone forming cells (osteoblasts), indirectly increasing the intestinal absorption of calcium and increasing the tubular re-absorption of calcium and excretion of phosphate by the kidney.
Pharmacodynamic Effects: Teriparatide is a bone formation agent to treat osteoporosis. The skeletal effects of Teriparatide depend upon the pattern of systemic exposure. Once daily administration of Teriparatide increases apposition of new bone on trabecular and cortical bone surfaces by preferential stimulation of osteoblastic activity over osteoclastic activity.
Pharmacokinetics: Teriparatide is extensively absorbed after subcutaneous injection; peak plasma concentrations are reached after about 30 minutes. Absolute bioavailability is reported to be about 95%. Teriparatide is eliminated through hepatic and extra hepatic clearance (approximately 62 L/hr in women and 94 L/hr in men). The volume of distribution is approximately 1.7 L/Kg. The half-life of teriparatide is approximately 1 hr. when administered subcutaneously, which reflects the time required for absorption from the injection site. No metabolism or excretion studies with teriparatide have been reported but the peripheral metabolism of parathyroid hormone is believed to occur predominantly in liver and kidney.
Pharmacokinetics in special population: Teriparatide is extensively absorbed after subcutaneous injection; the absolute bioavailability is approximately 95% based on pooled data from 20, 40, and 80-mcg doses. The rates of absorption and elimination are rapid. The peptide reaches peak serum concentrations about 30 minutes after subcutaneous injection of a 20-mcg dose and declines to non-quantifiable concentrations within 3 hours.
Systemic clearance of teriparatide (approximately 62 L/hr in women and 94 L/hr in men) exceeds the rate of normal liver plasma flow, consistent with both hepatic and extra-hepatic clearance. Volume of distribution, following intravenous injection, is approximately 0.12 L/kg. Intersubject variability in systemic clearance and volume of distribution is 25% to 50%. The half-life of teriparatide in serum is 5 minutes when administered by intravenous injection and approximately 1 hour when administered by subcutaneous injection. The longer half-life following subcutaneous administration reflects the time required for absorption from the injection site.
No metabolism or excretion studies have been performed with teriparatide. Peripheral metabolism of PTH is believed to occur by non-specific enzymatic mechanisms in the liver followed by excretion via the kidneys.
Special Populations: Pediatric: Pharmacokinetic data in pediatric patients are not available.
Geriatric: No age-related differences in teriparatide pharmacokinetics were detected (range 31 to 85 years).
Gender: Although systemic exposure to teriparatide was approximately 20% to 30% lower in men than women, the recommended dose for both genders is 20 mcg/day.
Race: The populations included in the pharmacokinetic analyses were 98.5% Caucasian. The influence of race has not been determined.
Renal insufficiency: No pharmacokinetic differences were identified in 11 patients with mild or moderate renal insufficiency [creatinine clearance (CrCl) 30 to 72 mL/min] administered a single dose of teriparatide. In 5 patients with severe renal insufficiency (CrCl <30 mL/min), the AUC and t½ of teriparatide were increased by 73% and 77%, respectively. Maximum serum concentration of teriparatide was not increased. No studies have been performed in patients undergoing dialysis for chronic renal failure.
Heart failure: No clinically relevant pharmacokinetic, blood pressure, or pulse rate differences were identified in 13 patients with stable New York Heart Association Class I to III heart failure after the administration of two 20-mcg doses of teriparatide.
Hepatic insufficiency: Non-specific proteolytic enzymes in the liver (possibly Kupffer cells) cleave PTH(1-34) and PTH(1-84) into fragments that are cleared from the circulation mainly by the kidney. No studies have been performed in patients with hepatic impairment.
Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenesis: Two carcinogenicity bioassays were conducted in Fischer 344 rats. In the first study, male and female rats were given daily subcutaneous teriparatide injections of 5, 30, or 75 mcg/kg/day for 24 months from 2 months of age. These doses resulted in systemic exposures that were, respectively, 3, 20, and 60 times higher than the systemic exposure observed in humans following a subcutaneous dose of 20 mcg (based on AUC comparison). Teriparatide treatment resulted in a marked dose-related increase in the incidence of osteosarcoma, a rare malignant bone tumor, in both male and female rats. Osteosarcomas were observed at all doses and the incidence reached 40% to 50% in the high-dose groups. Teriparatide also caused a dose-related increase in osteoblastoma and osteoma in both sexes. No osteosarcomas, osteoblastomas or osteomas were observed in untreated control rats. The bone tumors in rats occurred in association with a large increase in bone mass and focal osteoblast hyperplasia.
The second 2-year study was carried out in order to determine the effect of treatment duration and animal age on the development of bone tumors. Female rats were treated for different periods between 2 and 26 months of age with subcutaneous doses of 5 and 30 mcg/kg (equivalent to 3 and 20 times the human exposure at the 20-mcg dose, based on AUC comparison). The study showed that the occurrence of osteosarcoma, osteoblastoma and osteoma was dependent upon dose and duration of exposure. Bone tumors were observed when immature 2-month old rats were treated with 30 mcg/kg/day for 24 months or with 5 or 30 mcg/kg/day for 6 months. Bone tumors were also observed when mature 6-month old rats were treated with 30 mcg/kg/day for 6 or 20 months. Tumors were not detected when mature 6-month old rats were treated with 5 mcg/kg/day for 6 or 20 months. The results did not demonstrate a difference in susceptibility to bone tumor formation, associated with teriparatide treatment, between mature and immature rats.
The relevance of these rat findings to humans is uncertain.
Mutagenesis: Teriparatide was not genotoxic in any of the following test systems: the Ames test for bacterial mutagenesis; the mouse lymphoma assay for mammalian cell mutation; the chromosomal aberration assay in Chinese hamster ovary cells, with and without metabolic activation; and the in vivo micronucleus test in mice.
Impairment of fertility: No effects on fertility were observed in male and female rats given subcutaneous teriparatide doses of 30, 100, or 300 mcg/kg/day prior to mating and in females continuing through gestation Day 6 (16 to 160 times the human dose of 20 mcg based on surface area, mcg/m2).
Pregnancy: Pregnancy Category C: In pregnant rats given subcutaneous teriparatide doses up to 1000 mcg/kg/day, there were no mortality. In pregnant mice given subcutaneous doses of 225 or 1000 mcg/kg/day (≥ 60 times the human dose based on surface area, mcg/m2) from gestation Day 6 through 15, the fetuses showed an increased incidence of skeletal deviations or variations (interrupted rib, extra vertebra or rib).
Developmental effects in a perinatal/postnatal study in pregnant rats given subcutaneous doses of teriparatide from gestation day 6 through postpartum Day 20 included mild growth retardation in female offspring at doses ≥ 225 mcg/kg/day (≥ 120 times the human dose based on surface area, mcg/m2), and in male offspring at 1000 mcg/kg/day (540 times the human dose based on surface area, mcg/m2). There was also reduced motor activity in both male and female offspring at 1000 mcg/kg/day. There were no developmental or reproductive effects in mice or rats at a dose of 30 mcg/kg (8 or 16 times the human dose based on surface area, mcg/m2). The effect of teriparatide treatment on human fetal development has not been studied. Teriparatide (rDNA origin) is not indicated for use in pregnancy.
Nursing Mothers: Because Teriparatide (rDNA origin) is indicated for the treatment of osteoporosis in postmenopausal women, it should not be administered to women who are nursing their children. There have been no clinical studies to determine if teriparatide is secreted into breast milk.
Pediatric Use: The safety and efficacy of Teriparatide (rDNA origin) have not been established in pediatric populations. Teriparatide is not indicated for use in pediatric patients.
Geriatric Use: Of the patients receiving Teriparatide (rDNA origin) in the osteoporosis trial of 1637 postmenopausal women, 75% were 65 years of age and over and 23% were 75 years of age and over. Of the patients receiving Teriparatide in the osteoporosis trial of 437 men, 39% were 65 years of age and over and 13% were 75 years of age and over. No significant differences in bone response or adverse reactions were seen in geriatric patients receiving Teriparatide as compared with younger patients. Nonetheless, as with many medications, elderly patients may have greater sensitivity to the adverse effects of Teriparatide.
Treatment of Postmenopausal Women with Osteoporosis at High Risk for Fracture: Teriparatide (rDNA origin) injection is indicated for the treatment of postmenopausal women with osteoporosis at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or patients who have failed or are intolerant to other available osteoporosis therapy. In postmenopausal women with osteoporosis, teriparatide (rDNA origin) injection reduces the risk of vertebral and nonvertebral fractures.
Increase of Bone Mass in Men with Primary or Hypogonadal Osteoporosis at High Risk for Fracture: Teriparatide (rDNA origin) injection is indicated to increase bone mass in men with primary or hypogonadal osteoporosis at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or patents who have failed or are intolerant to other available osteoporosis therapy.
Treatment of Men and Women with Glucocorticoid-Induced Osteoporosis at High Risk for Fracture: Teriparatide injection is indicated for the treatment of men and women with osteoporosis associated with sustained systemic glucocorticoid therapy (daily dosage equivalent to 5 mg or greater of prednisone) at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or patients who have failed or are intolerant to other available osteoporosis therapy.
Route of administration: Subcutaneous Injection.
Treatment of Postmenopausal Women with Osteoporosis at High Risk for Fracture: The recommended dose is 20 mcg subcutaneously once a day.
Increase of Bone Mass in Men with Primary or Hypogonadal Osteoporosis at High Risk for Fracture: The recommended dose is 20 mcg subcutaneously once a day.
Treatment of Men and Women with Glucocorticoid-Induced Osteoporosis at High Risk for Fracture: The recommended dose is 20 mcg subcutaneously once a day.
Administration: Teriparatide (rDNA origin) injection should be administered as a subcutaneous injection into the thigh or abdominal wall. There are no data available on the safety or efficacy of intravenous or intramuscular injection of teriparatide (rdna origin) injection.
Teriparatide (rDNA origin) injection should be administered initially under circumstances in which the patient can sit or lie down if symptoms of orthostatic hypotension occur.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. Teriparatide (rDNA origin) injection is a clear and colorless liquid. Do not use if solid particles appear or if the solution is cloudy or colored.
Patients and caregivers who administer Teriparatide (rDNA origin) injection should receive appropriate training and instruction on the proper use of the Teriparatide (rDNA origin) injection delivery device from a qualified health professional.
Pediatric: There is no experience in children. rhPTH (1-34) (teriparatide for injection) should not be used in pediatric patients or young adults with open epiphyses.
Geriatric: Dosage adjustment based on age is not required.
MISSED DOSE: If the patient misses a dose, use it as soon as remembered. If it is near the time of the next dose, skip the missed dose and resume the usual dosing schedule. Do not double the dose to catch up.
Treatment Duration: The safety and efficacy of Teriparatide (rDNA origin) injection have not been evaluated beyond 2 years of treatment. Consequently, use of the drug for more than 2 years during a patient's lifetime is not recommended.
Signs and symptoms: No cases of overdose were reported. Teriparatide has been administered in single doses of up to 100 mcg and in repeated doses of up to 60 mcg/day for 6 weeks. The effects of overdose that might be expected include delayed hypercalcemia and risk of orthostatic hypotension. Nausea, vomiting, dizziness and headache can also occur.
Overdose experience based on post-marketing spontaneous reports: There have been cases of medication error where the entire contents (up to 800 mcg) of the Teriparatide have been administered as multiple doses. Transient events reported have included nausea, weakness/lethargy and hypotension. In some cases, no adverse events occurred as a result of the overdose. No fatalities associated with overdose of Teriparatide have been reported.
Overdose management: There is no specific antidote for Teriparatide. Treatment of suspected overdose should include transitory discontinuation of teriparatide, monitoring of serum calcium, and implementation of appropriate supportive measures, such as hydration.
rh PTH(1-34)(Teriparatide for Injection) is contraindicated in the following patients: Hypersensitivity to teriparatide or to any of the excipients of this product; Pre-existing hypercalcaemia; Severe renal impairment; Metabolic bone diseases other than primary osteoporosis (including HyperParathyroidism and Paget's disease of bone); Unexplained elevations of alkaline phosphatase; Prior external beam or implant radiation therapy to the skeleton; Patients with skeletal malignancies or bone metastases should be excluded from treatment with teriparatide.
POTENTIAL RISK OF OSTEOSARCOMA: In male and female rats, teriparatide caused an increase in the incidence of osteosarcoma (a malignant bone tumor) that was dependent on dose and treatment duration. The effect was observed at systemic exposures to teriparatide ranging from 3 to 60 times the exposure in humans given a 20-mcg dose. Because of the uncertain relevance of the rat osteosarcoma finding to humans, prescribe teriparatide (rDNA origin) injection only for patients for whom the potential benefits are considered to outweigh the potential risk. Teriparatide (rDNA origin) injection should not be prescribed for patents who are at increased baseline risk for osteosarcoma including those with Paget's disease of bone or unexplained elevations of alkaline phosphatase, pediatric and young adult patients with open epiphyses, or prior external beam or implant radiation therapy involving the skeleton.
General: Teriparatide has not been studied in patients with active urolithiasis in reported clinical trials.
Teriparatide should be used with caution in patients with active or recent urolithiasis because of the potential to exacerbate this condition. In reported short term clinical studies with teriparatide injection, isolated episodes of transient orthostatic hypotension were observed. Typically, an event began within 4 hours of dosing and spontaneously resolved within a few minutes to a few hours. When transient orthostatic hypotension occurred, it happened within the first several doses, was relieved by placing subjects in a reclining position, and did not preclude continued treatment.
In a reported study of 15 healthy people administered digoxin daily to steady state, a single dose of teriparatide did not alter the effect of digoxin on the systolic time interval from electrocardiographic Q-wave onset to aortic valve closure, a measure of digoxin's calcium mediated cardiac effect).
However, sporadic case reports have suggested that hypercalcemia may predispose patients to digitalis toxicity. Because teriparatide transiently increases serum calcium, Teriparatide should be used with caution in patients taking digitalis. In normocalcaemic patients, slight and transient elevations of serum calcium concentrations reach a maximum between 4 and 6 hours and return to baseline by 16 to 24 hours after each dose of Teriparatide.
Routine calcium monitoring during therapy is not required.
Therefore, if any blood samples are taken from a patient, this should be done at least 16 hours after the most recent Teriparatide injection.
Teriparatide may cause small increases in urinary calcium excretion.
Limited information is available to evaluate safety in patients with hepatic, renal and cardiac disease.
No clinically important adverse renal effects were observed in reported clinical studies.
Assessments included creatinine clearance; measurements of blood urea nitrogen (BUN), creatinine, and electrolytes in serum; urine specific gravity and pH; and examination of urine sediment. Longterm evaluation of patients with severe renal insufficiency, patients undergoing acute or chronic dialysis, or patients who have functioning renal transplants has not been reported. Caution should be exercised in patients with moderate renal impairment.
Teriparatide therapy was associated with increased incidence of elevated uric acid, with the incidence being highest in patients with moderately impaired renal function and in those receiving teriparatide 40 mcg/day. Even so, adverse event data did not suggest an increased incidence of gout or arthralgia or of nephrolithiasis in teriparatide treated patients with normal, mild or moderate renal impairment.
Effects on ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed. However, transient, orthostatic hypotension or dizziness was observed in some patients. These patients should refrain from driving or the use of machines until symptoms have subsided.
Use in Pregnancy: Reported studies in rabbits have shown reproductive toxicity. The potential risk for humans is unknown. Given the indication, Teriparatide should not be used during pregnancy.
Pregnancy: Reported studies in rabbits have shown reproductive toxicity. The potential risk for humans is unknown. Given the indication, Teriparatide should not be used during pregnancy.
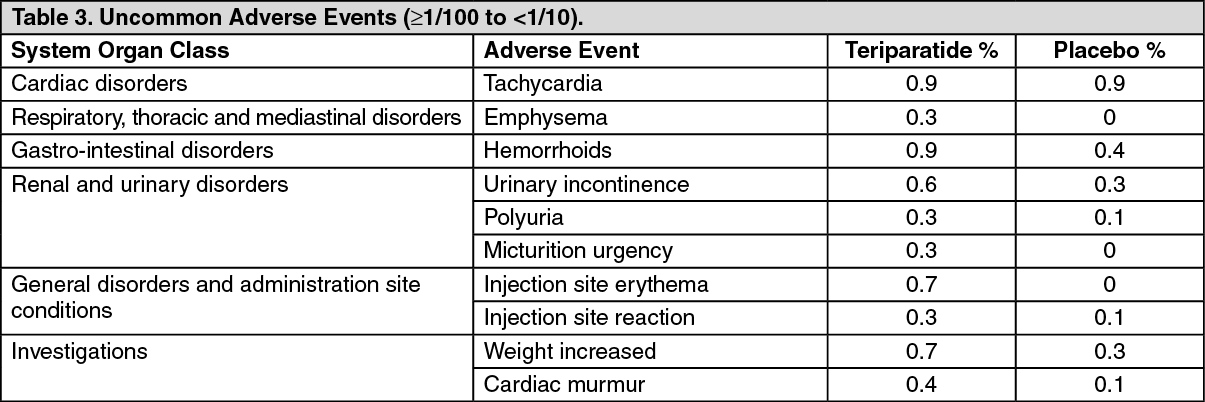
The following convention has been used for the classification of the adverse reactions: very common (≥1/10), common (≥1/100 to < 1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). The most commonly reported adverse events in patients heated with teriparatide are nausea, pain in limb, headache and dizziness. (See Tables 1, 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Teriparatide increases serum uric acid concentrations. However, the hyperuricemia does not result in an increase in gout, arthralgia or urolithiasis. Antibodies that cross-reacted with teriparatide were detected in women receiving teriparatide. Generally, antibodies were first detected following 12 months of treatment and diminished after withdrawal of therapy. There was no evidence of hypersensitivity reactions, allergic reactions, effects on serum calcium, or effects on bone mineral density (BMD) response.
There have been spontaneous reports of the following adverse reactions. (See Table 4.)
Click on icon to see table/diagram/image
Digoxin: A single teriparatide (rdna origin) injection dose did not alter the effect of digoxin on the systolic time interval (from electrocardiographic Q-wave onset to aortic valve closure, a measure of digoxin's calcium-mediated cardiac effect). However, because teriparatide (rdna origin) injection may transiently increase serum calcium, teriparatide (rdna origin) injection should be used with caution in patients taking digoxin.
Hydrochlorothiazide: The coadministration of hydrochlorothiazide 25 mg with teriparatide did not affect the serum calcium response to teriparatide 40 mcg. The effect of coadministration of a higher dose of hydrochlorothiazide with teriparatide on serum calcium levels has not been studied.
Furosemide: Coadministration of intravenous furosemide (20 to 100 mg) with teriparatide 40 mcg in healthy people and patients with mild, moderate or severe renal impairment (CrCl 13 to 72 mL/min) resulted in small increases in the serum calcium (2%) and 24-hour urine calcium (37%) responses to teriparatide that did not appear to be clinically important.
Protect from light and moisture.
Store between 2 to 8°C.
Do not freeze.
Shelf Life: Not more than 24 months from the date of manufacture when stored at temperature 2 - 8°C.
H05AA02 - teriparatide ; Belongs to the class of parathyroid hormones and analogues. Used in the management of calcium homeostasis.
Inj (multi-dose cartridge) 750 mcg/3 mL (clear and colourless solution) x 1's.



 Sign Out
Sign Out