Adult: As enalaprilat: 1.25 mg 6 hourly via slow infusion over 5 minutes.
Oral Hypertension
Adult: Initially, 5 mg once daily. Maintenance: 10-20 mg once daily, up to 40 mg in severe cases, may be given in 2 divided doses if control is inadequate. Dose should be individualised according to patient profile and blood pressure response. Max: 40 mg daily. Child: 20-<50 kg: Initially, 2.5 mg once daily, may increase to Max 20 mg once daily if necessary. ≥50 kg: Initially, 5 mg once daily, increase to Max 40 mg once daily if necessary. Elderly: Initially, 2.5 mg once daily, adjust subsequent dose according to response.
Oral Asymptomatic left ventricular dysfunction, Heart failure
Adult: Initially, 2.5 mg once daily, increased gradually up to 20 mg. Usual maintenance dose: 20 mg daily as a single dose or in 2 divided doses, titrated according to patient tolerance over 2-4 weeks. Max: 40 mg daily in 2 divided doses. Elderly: Initially, 2.5 mg once daily, adjust subsequent dose according to response.
Special Patient Group
Hypertension PO
Patients taking diuretic: Initially, 2.5 mg daily. Discontinue diuretic 2-3 days before enalapril administration.
IV
Patients taking diuretic: Half the initial dose.
Renal Impairment
Oral:
CrCl (mL/min)
Dosage
≤30 or on dialysis
Initially, 2.5 mg once daily, adjusted
subsequently according to response.
Intravenous: Hypertension
CrCl (mL/min)
Dosage
<30 or on haemodialysis
As enalaprilat: Initially, 0.625 mg given
over 5 minutes up to 1 hour, repeat dose after 1 hour if necessary. May
give additional dose of 1.25 mg 6 hourly according
to response.
Administration
May be taken with or without food.
Reconstitution
Inj: Dilute vial with up to 50 mL of a compatible diluent (e.g. dextrose 5%, NaCl 0.9%).
Incompatibility
Incompatible with phenytoin Na in NaCl 0.9%, and amphotericin B in dextrose 5% solution.
Contraindications
History of angioedema related to previous treatment with ACE inhibitor, idiopathic or hereditary angioedema. Concomitant use with aliskiren in patient with diabetes mellitus. Coadministration with or within 36 hours of switching to or from a neprilysin inhibitor (e.g. sacubitril). Pregnancy.
Special Precautions
Patient with diabetes mellitus, volume depletion, renal artery stenosis, severe aortic stenosis; ascites due to cirrhosis or refractory ascites; ischaemic heart disease or cerebrovascular disease; collagen vascular disease; hypertrophic cardiomyopathy and outflow tract obstruction; pre-existing renal insufficiency. Black race. Renal and hepatic impairment. Children and elderly. Lactation.
This drug may cause occasional dizziness or weariness, if affected, do not drive or operate machinery.
Monitoring Parameters
Monitor blood pressure, baseline serum creatinine and K; reassess serum creatinine and K within 1-2 weeks after initiation and periodically thereafter in patient treated for heart failure.
Overdosage
Symptoms: Marked hypotension, stupor, circulatory shock, electrolyte disturbance, renal failure, hyperventilation, tachycardia, palpitations, bradycardia, dizziness, anxiety and cough. Management: Infuse normal saline solution and put patient in supine position in case of hypotension. May consider treatment with IV catecholamines. May induce emesis, perform gastric lavage or administer absorbents or sodium sulfate in recent ingestion.
Drug Interactions
May potentiate hypotensive action with diuretics, other antihypertensives, TCAs, vasodilating agents (e.g. nitrates) or anaesthetics. May increase lithium serum concentration and enhance risk of lithium toxicity. May increase risk of hypoglycaemia with oral antidiabetic agents or insulin. May increase risk of hyperkalaemia with K-sparing diuretics (e.g. spironolactone, triamterene, amiloride), K-containing supplements or salt substitutes. May increase risk of renal impairment with NSAIDs (e.g. aspirin, ibuprofen) including COX-2 inhibitors. Rarely, may cause nitritoid reactions with injectable gold (Na aurothiomalate). Potentially Fatal: Increased risk of angioedema with neprilysin inhibitors (e.g. sacubitril, racecadotril), and mammalian target of rapamycin inhibitors (e.g. sirolimus, everolimus). May increase risk of side effects (e.g. hypotension, hyperkalaemia, acute renal failure) with aliskiren in patient with diabetes.
Food Interaction
Increased hypotensive effect with alcohol.
Action
Description: Enalapril is a prodrug of enalaprilat, which inhibits conversion of angiotensin I to angiotensin II (a potent vasoconstrictor) resulting in reduced angiotensin II-induced vasoconstriction, Na retention and aldosterone secretion. Onset: Approx 1 hour. Duration: 12-24 hours. Pharmacokinetics: Absorption: Rapidly absorbed in the gastrointestinal tract. Time to peak plasma concentration: Approx 0.5-1.5 hour (enalapril); 3-4.5 hours (enalaprilat). Distribution: Plasma protein binding: Approx 50%. Metabolism: Extensively hydrolysed in the liver into active metabolite enalaprilat. Excretion: Via urine (61%; 18% as enalapril, 43% as enalaprilat); faeces (33%; 6% as enalapril, 27% as enalaprilat). Elimination half-life: 2 hours (enalapril); approx 35 hours (enalaprilat).
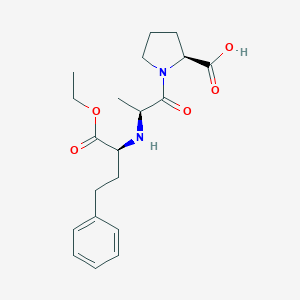
Chemical Structure
Enalapril Source: National Center for Biotechnology Information. PubChem Database. Enalapril, CID=5388962, https://pubchem.ncbi.nlm.nih.gov/compound/Enalapril (accessed on Mar. 26, 2020)
Storage
Tab: Store below 25°C. Protect from moisture. Oral solution: Store between 2-8°C. May store between 20-25°C for up to 60 days. Do not freeze and avoid excessive heat. Inj: Store at 25°C.
C09AA02 - enalapril ; Belongs to the class of ACE inhibitors. Used in the treatment of cardiovascular disease.
References
Anon. Enalapril. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 06/11/2019.Anon. Enalapril. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 06/11/2019.Buckingham R (ed). Enalapril. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 06/11/2019.Enalapril Maleate Tablet (Sandoz, Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 06/11/2019.Enalaprilat Injection (West-Ward Pharmaceuticals Corp). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 06/11/2019.Epaned Solution (Silvergate Pharmaceuticals, Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 06/11/2019.Joint Formulary Committee. Enalapril Maleate. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 06/11/2019.



 Sign Out
Sign Out