Clinical Trial Data: Clinical studies have shown that cetirizine at the recommended dosage has minor adverse effects on the CNS, including somnolence, fatigue, dizziness and headache. In some cases, paradoxical CNS stimulation has been reported.
Although cetirizine is a selective antagonist of peripheral H
1-receptors and is relatively free of anticholinergic activity, isolated cases of micturition difficulty, eye accommodation disorders and dry mouth have been reported.
Instances of abnormal hepatic function with elevated hepatic enzymes accompanied by elevated bilirubin have been reported. Mostly this resolves upon discontinuation of the treatment with cetirizine.
Double-blind controlled clinical trials comparing cetirizine to placebo or other antihistamines at the recommended dosage (10 mg daily for cetirizine), of which quantified safety data are available, included more than 3200 subjects exposed to cetirizine.
From this pooling, the following adverse events were reported for cetirizine 10 mg in the placebo-controlled trials at rates of 1.0% or greater: (see Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Although statistically more common than under placebo, somnolence was mild to moderate in the majority of cases.
Objective tests as demonstrated by other studies have demonstrated that usual daily activities are unaffected at the recommended daily dose in healthy young volunteers.
Paediatric population: Adverse events at rates of 1% or greater in children aged from 6 months to 12 years, included in placebo-controlled clinical trials are: (see Table 3.)
Click on icon to see table/diagram/image
Post Marketing Data: Adverse drug reactions (ADRs) are listed as follows by MedDRA system organ class and by frequency.
Frequencies are defined as: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data).
Blood and lymphatic disorders: Very rare: thrombocytopenia.
Immune system disorders: Rare: hypersensitivity. Very rare: anaphylactic shock.
Metabolism and nutrition disorders: Not known: increased appetite.
Psychiatric disorders: Uncommon: agitation. Rare: aggression, confusion, depression, hallucination, insomnia. Very rare: tics. Not known: suicidal ideation, nightmare.
Nervous system disorders: Uncommon: paraesthesia. Rare: convulsions. Very rare: dysgeusia, dyskinesia, dystonia, syncope, tremor. Not known: amnesia, memory impairment.
Eye disorders: Very rare: accommodation disorder, blurred vision, oculogyration.
Ear and labyrinth disorders: Not known: vertigo.
Cardiac disorders: Rare: tachycardia.
Gastrointestinal disorders: Uncommon: diarrhoea.
Hepatobiliary disorders: Rare: hepatic function abnormal (transaminases increased, blood bilirubin increased, blood alkaline phosphatase increased, gamma-glutamyl transferase increased). Not known: hepatitis.
Skin and subcutaneous tissue disorders: Uncommon: pruritus, rash. Rare: urticaria. Very rare: angioedema, fixed drug eruption. Not known: acute generalized exanthematous pustulosis (AGEP).
Musculoskeletal and connective tissue disorders: Not known: arthralgia.
Renal and urinary disorders: Very rare: dysuria, enuresis. Not known: urinary retention (see Precautions).
General disorders and administration site conditions: Uncommon: asthenia, malaise. Rare: oedema.
Investigations: Rare: weight increased.
Skin reactions occurring after discontinuation of cetirizine: After discontinuation of cetirizine, pruritus (intense itching) and/or urticaria have been reported (see Precautions).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image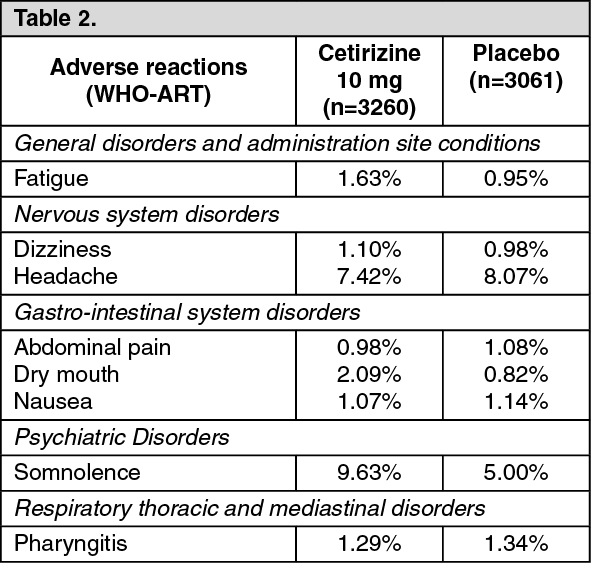 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
