


 Sign Out
Sign Out

Pharmacodynamics: Cardiac Electrophysiology: Based on evaluation of the QTc interval in patients and in a healthy volunteer study, abemaciclib did not cause large mean increases (i.e., 20 ms) in the QTc interval.
Clinical Studies: Early Breast Cancer: Early Breast Cancer: Randomised Phase 3 Study monarchE: YULAREB in combination with endocrine therapy: The efficacy and safety of YULAREB in combination with adjuvant endocrine therapy was evaluated in monarchE, a randomised, open label, two cohort, phase 3 study, in women and men with HR-positive, HER2-negative, node positive early breast cancer at high risk of recurrence. High risk of recurrence in Cohort 1 was defined by clinical and pathological features: either ≥ 4 pALN (positive axillary lymph nodes), or 1-3 pALN and at least one of the following criteria: tumor size ≥ 5 cm or histological grade 3.
A total of 5 637 patients were randomised in a 1:1 ratio to receive 2 years of YULAREB 150 mg twice daily plus physician's choice of standard endocrine therapy, or standard endocrine therapy alone. Randomization was stratified by prior chemotherapy, menopausal status, and region. Men were stratified as postmenopausal. Patients had completed definitive locoregional therapy (with or without neoadjuvant or adjuvant chemotherapy). Patients must have recovered from the acute side effects of any prior chemotherapy or radiotherapy. A washout period of 21 days after chemotherapy and 14 days after radiotherapy prior to randomization was required. Patients were allowed to receive up to 12 weeks of adjuvant endocrine therapy prior to randomisation. Adjuvant treatment with fulvestrant was not allowed as standard endocrine therapy. Patients with Eastern Cooperative Oncology Group (ECOG) Performance Status 0 or 1 were eligible. Patients with history of VTEs were excluded from the study. After the end of the study treatment period, in both treatment arms patients continued to receive adjuvant endocrine therapy for a cumulative duration of at least 5 years and up to 10 years, if medically appropriate. LHRH agonists were given when clinically indicated to pre- and perimenopausal women, and men.
Among the 5 637 randomised patients, 5 120 were enrolled in Cohort 1, representing 91% of the ITT population. In Cohort 1, patient demographics and baseline tumour characteristics were balanced between treatment arms. The median age of patients enrolled was approximately 51 years (range, 22-89 years), 15% of patients were 65 or older, 99% were women, 71% were Caucasian, 24% were Asian, and 5% Other. Forty three percent of patients were pre- or perimenopausal. Most patients received prior chemotherapy (36% neoadjuvant, 62% adjuvant), and prior radiotherapy (96%). Initial endocrine therapy received by patients included letrozole (39%), tamoxifen (31%), anastrozole (22%), or exemestane (8%).
Sixty-five percent of the patients had 4 or more positive lymph nodes, 41% had Grade 3 tumour, and 24% had pathological tumour size ≥5 cm at surgery.
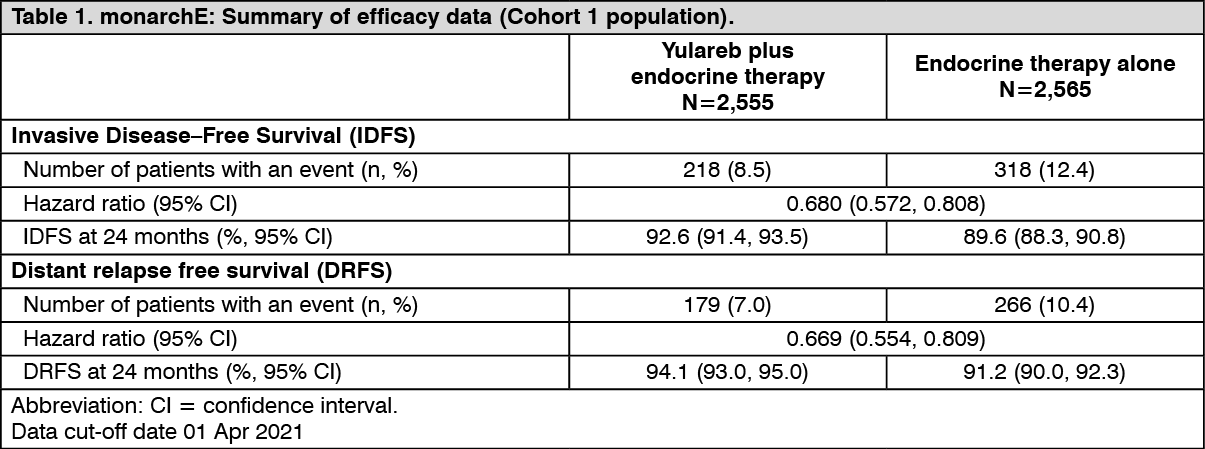
The primary endpoint was invasive disease-free survival (IDFS) in ITT population defined as the time from randomization to the first occurrence of ipsilateral invasive breast tumour recurrence, regional invasive breast cancer recurrence, distant recurrence, contralateral invasive breast cancer, second primary non-breast invasive cancer, or death attributable to any cause. Key secondary endpoint was distant relapse free survival (DRFS) in ITT population defined as time from randomization to the first occurrence of distant recurrence, or death attributable to any cause.
The primary objective of the study was met at the pre-planned interim analysis (16 Mar 2020 cut-off). A statistically significant improvement in IDFS was observed in patients who received YULAREB plus endocrine therapy versus endocrine therapy alone in the ITT population. The approval was granted for the large subpopulation, Cohort 1.
In a further analysis (01 April 2021 cut-off), 91% of the patients in Cohort 1 were off the 2 year study treatment period and the median duration of follow-up was 27.7 months.
Efficacy results in Cohort 1 are summarised in Table 1 and Figure 1. (See Table 1 and Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image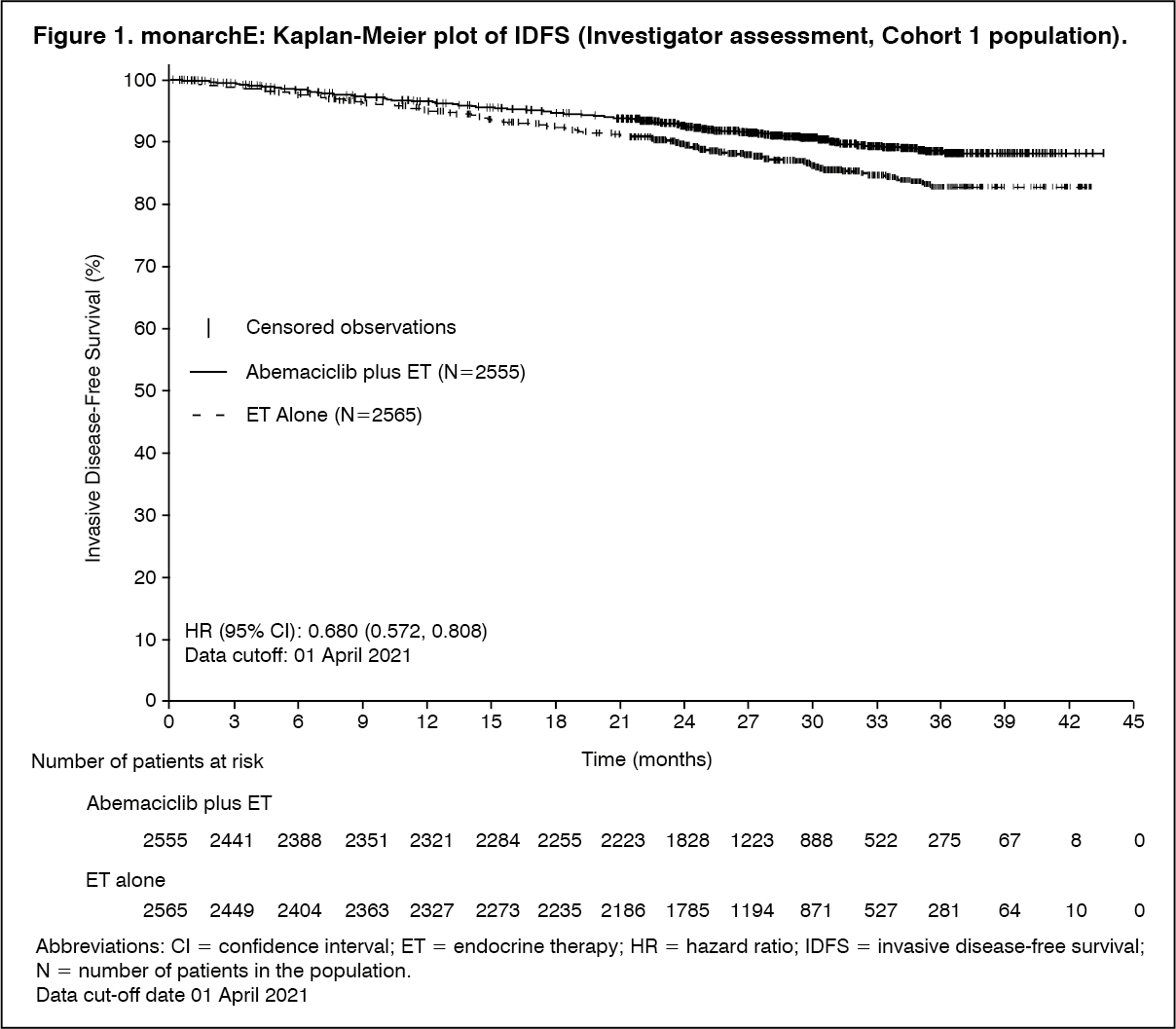 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBenefit was observed across patient subgroups defined by geographic region, menopausal status and prior chemotherapy within Cohort 1.
Advanced or Metastatic Breast Cancer: YULAREB in Combination with an Aromatase Inhibitor (Anastrozole or Letrozole) (MONARCH 3): Postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer with no prior systemic therapy in this disease setting: MONARCH 3 (NCT02246621) was a randomized (2:1), double-blinded, placebo-controlled, multicenter study in postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer in combination with a nonsteroidal aromatase inhibitor as initial endocrine-based therapy, including patients not previously treated with systemic therapy for breast cancer.
Randomization was stratified by disease site (visceral, bone only, or other) and by prior (neo)adjuvant endocrine therapy (aromatase inhibitor versus other versus no prior endocrine therapy). A total of 493 patients were randomized to receive 150 mg YULAREB or placebo orally twice daily, plus physician's choice of letrozole (80% of patients) or anastrozole (20% of patients). Patient median age was 63 years (range, 32-88 years) and the majority were White (58%) or Asian (30%). A total of 51% had received prior systemic therapy and 39% of patients had received chemotherapy, 53% had visceral disease, and 22% had bone-only disease.
Efficacy results are summarized in Table 2 and Figure 2. PFS was evaluated according to RECIST version 1.1 and PFS assessment based on a blinded independent radiologic review was consistent with the investigator assessment. Consistent results were observed across patient stratification subgroups of disease site and prior (neo)adjuvant endocrine therapy. At the time of the PFS analysis, 19% of patients had died, and overall survival data were immature. (See Table 2 and Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageYULAREB in Combination with Fulvestrant (MONARCH 2): Patients with HR-positive, HER2-negative advanced or metastatic breast cancer with disease progression on or after prior adjuvant or metastatic endocrine therapy: MONARCH 2 (NCT02107703) was a randomized, placebo-controlled, multicenter study in women with HR-positive, HER2-negative metastatic breast cancer in combination with fulvestrant in patients with disease progression following endocrine therapy who had not received chemotherapy in the metastatic setting. Randomization was stratified by disease site (visceral, bone only, or other) and by sensitivity to prior endocrine therapy (primary or secondary resistance). Primary endocrine therapy resistance was defined as relapse while on the first 2 years of adjuvant endocrine therapy or progressive disease within the first 6 months of first line endocrine therapy for metastatic breast cancer. A total of 669 patients were randomized to receive YULAREB or placebo orally twice daily plus intramuscular injection of 500 mg fulvestrant on days 1 and 15 of cycle 1 and then on day 1 of cycle 2 and beyond (28-day cycles). Pre/perimenopausal women were enrolled in the study and received the gonadotropin-releasing hormone agonist goserelin for at least 4 weeks prior to and for the duration of MONARCH 2. Patients remained on continuous treatment until development of progressive disease or unmanageable toxicity.
Patient median age was 60 years (range, 32-91 years), and 37% of patients were older than 65. The majority were White (56%), and 99% of patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Twenty percent (20%) of patients had de novo metastatic disease, 27% had bone-only disease, and 56% had visceral disease. Twenty-five percent (25%) of patients had primary endocrine therapy resistance. Seventeen percent (17%) of patients were pre- or perimenopausal.
The efficacy results from the MONARCH 2 study are summarized in Table 3, Figure 3, and Figure 4. PFS assessment based on a blinded independent radiologic review was consistent with the investigator assessment. Consistent results were observed across patient stratification subgroups of disease site and endocrine therapy resistance for PFS and OS. (See Table 3, Figures 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image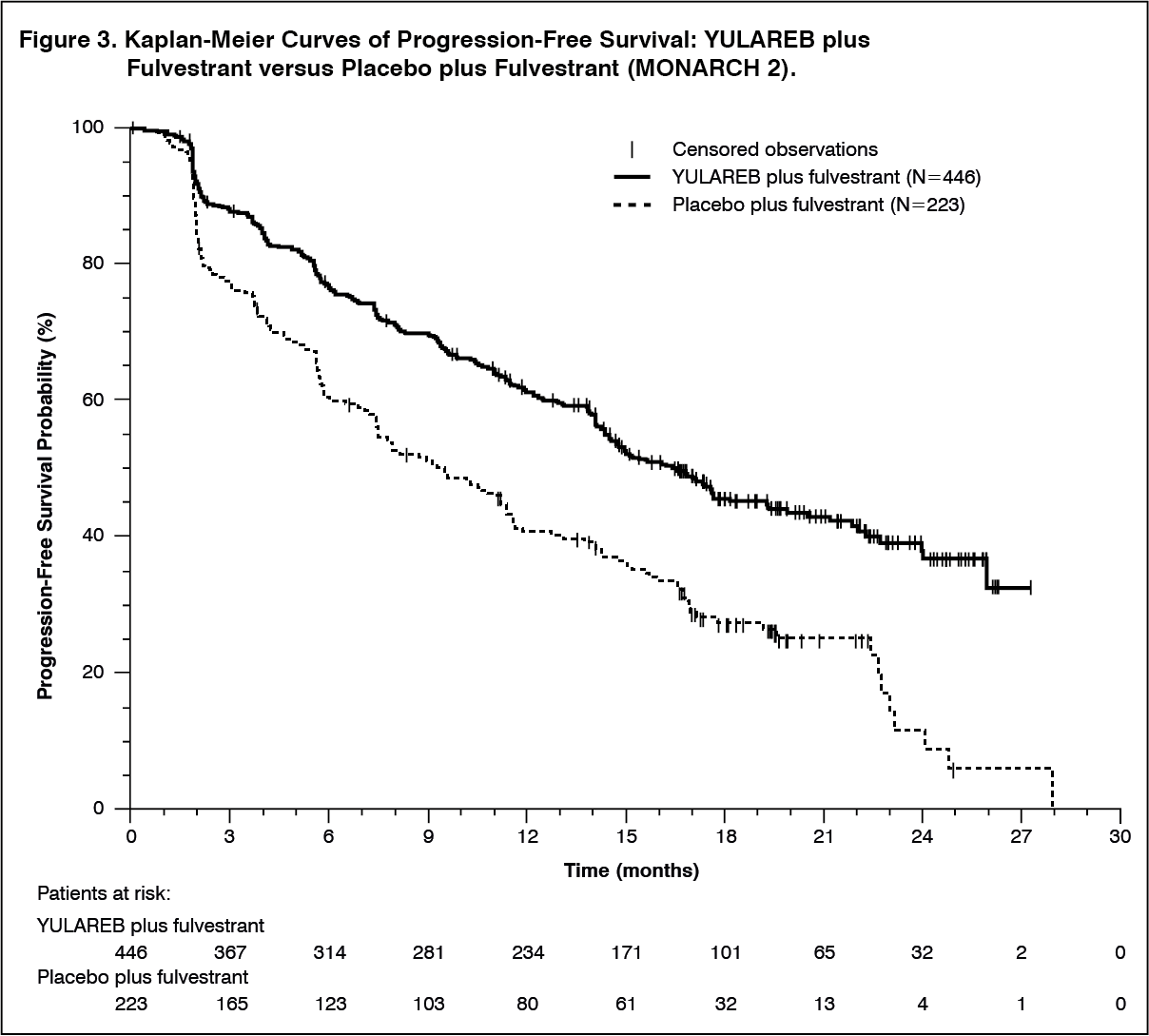 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image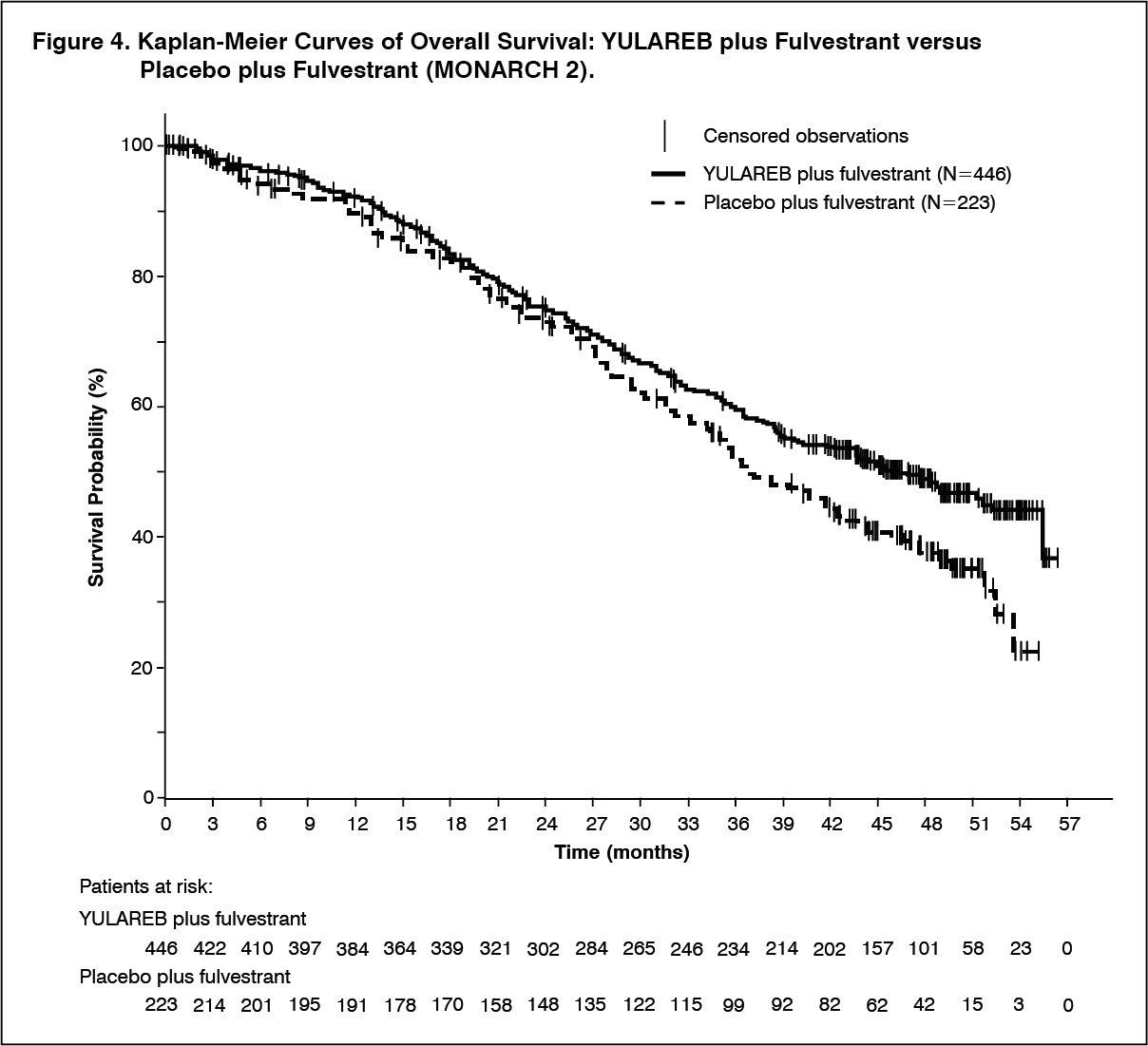 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: The pharmacokinetics of abemaciclib were characterized in patients with solid tumors, including breast cancer, and in healthy subjects.
Following single and repeated twice daily dosing of 50 mg (0.3 times the approved recommended 150 mg dosage), the increase in plasma exposure (AUC) and Cmax was approximately dose proportional. Steady state was achieved within 5 days following repeated twice daily dosing, and the estimated geometric mean accumulation ratio was 2.3 (50% CV) and 3.2 (59% CV) based on Cmax and AUC, respectively.
Absorption: The absolute bioavailability of abemaciclib after a single oral dose of 200 mg is 45% (19% CV). The median Tmax of abemaciclib is 8.0 hours (range: 4.1-24.0 hours).
Effect of Food: A high-fat, high-calorie meal (approximately 800 to 1000 calories with 150 calories from protein, 250 calories from carbohydrate, and 500 to 600 calories from fat) administered to healthy subjects increased the AUC of abemaciclib plus its active metabolites by 9% and increased Cmax by 26%.
Distribution: In vitro, abemaciclib was bound to human plasma proteins, serum albumin, and alpha-1-acid glycoprotein in a concentration independent manner from 152 ng/mL to 5066 ng/mL. In a clinical study, the mean (standard deviation, SD) bound fraction was 96.3% (1.1) for abemaciclib, 93.4% (1.3) for M2, 96.8% (0.8) for M18, and 97.8% (0.6) for M20. The geometric mean systemic volume of distribution is approximately 690.3 L (49% CV).
In patients with advanced cancer, including breast cancer, concentrations of abemaciclib and its active metabolites M2 and M20 in cerebrospinal fluid are comparable to unbound plasma concentrations.
Elimination: The geometric mean hepatic clearance (CL) of abemaciclib in patients was 26.0 L/h (51% CV), and the mean plasma elimination half-life for abemaciclib in patients was 18.3 hours (72% CV).
Metabolism: Hepatic metabolism is the main route of clearance for abemaciclib. Abemaciclib is metabolized to several metabolites primarily by cytochrome P450 (CYP) 3A4, with formation of N-desethylabemaciclib (M2) representing the major metabolism pathway. Additional metabolites include hydroxyabemaciclib (M20), hydroxy-N-desethylabemaciclib (M18), and an oxidative metabolite (M1). M2, M18, and M20 are equipotent to abemaciclib and their AUCs accounted for 25%, 13%, and 26% of the total circulating analytes in plasma, respectively.
Excretion: After a single 150 mg oral dose of radiolabeled abemaciclib, approximately 81% of the dose was recovered in feces and approximately 3% recovered in urine. The majority of the dose eliminated in feces was metabolites.
Specific Populations: Age, Gender, and Body Weight: Based on a population pharmacokinetic analysis in patients with cancer, age (range 24-91 years), gender (134 males and 856 females), and body weight (range 36-175 kg) had no effect on the exposure of abemaciclib.
Patients with Renal Impairment: In a population pharmacokinetic analysis of 990 individuals, in which 381 individuals had mild renal impairment (60 mL/min ≤ CLcr <90 mL/min) and 126 individuals had moderate renal impairment (30 mL/min ≤ CLcr <60 mL/min), mild and moderate renal impairment had no effect on the exposure of abemaciclib [see Renal Impairment under Precautions]. The effect of severe renal impairment (CLcr <30 mL/min) on pharmacokinetics of abemaciclib is unknown.
Patients with Hepatic Impairment: Following a single 200 mg oral dose of abemaciclib, the relative potency adjusted unbound AUC0-INF of abemaciclib plus its active metabolites (M2, M18, M20) in plasma increased 1.2-fold in subjects with mild hepatic impairment (Child-Pugh A, n=9), 1.1-fold in subjects with moderate hepatic impairment (Child-Pugh B, n=10), and 2.4-fold in subjects with severe hepatic impairment (Child-Pugh C, n=6) relative to subjects with normal hepatic function (n=10) [see Hepatic Impairment under Precautions]. In subjects with severe hepatic impairment, the mean plasma elimination half-life of abemaciclib increased to 55 hours compared to 24 hours in subjects with normal hepatic function.
Drug Interaction Studies: Effects of Other Drugs on Abemaciclib: Strong CYP3A Inhibitors: Ketoconazole (a strong CYP3A inhibitor) is predicted to increase the AUC of abemaciclib by up to 16-fold.
Coadministration of 500 mg twice daily doses of clarithromycin (a strong CYP3A inhibitor) with a single 50 mg dose of YULAREB (0.3 times the approved recommended 150 mg dosage) increased the relative potency adjusted unbound AUC0-INF of abemaciclib plus its active metabolites (M2, M18, and M20) by 2.5-fold relative to abemaciclib alone in cancer patients.
Moderate CYP3A Inhibitors: Verapamil and diltiazem (moderate CYP3A inhibitors) are predicted to increase the relative potency adjusted unbound AUC of abemaciclib plus its active metabolites (M2, M18, and M20) by approximately 1.6-fold and 2.4-fold, respectively.
Strong CYP3A Inducers: Coadministration of 600 mg daily doses of rifampin (a strong CYP3A inducer) with a single 200 mg dose of YULAREB decreased the relative potency adjusted unbound AUC0-INF of abemaciclib plus its active metabolites (M2, M18, and M20) by approximately 70% in healthy subjects.
Moderate CYP3A Inducers: Efavirenz, bosentan, and modafinil (moderate CYP3A inducers) are predicted to decrease the relative potency adjusted unbound AUC of abemaciclib plus its active metabolites (M2, M18, and M20) by 53%, 41%, and 29%, respectively.
Loperamide: Co-administration of a single 8 mg dose of loperamide with a single 400 mg dose of abemaciclib in healthy subjects increased the relative potency adjusted unbound AUC0-INF of abemaciclib plus its active metabolites (M2 and M20) by 12%, which is not considered clinically relevant.
Endocrine Therapies: In clinical studies in patients with breast cancer, there was no clinically relevant effect of fulvestrant, anastrozole, letrozole, exemestane, or tamoxifen on abemaciclib pharmacokinetics.
Effects of Abemaciclib on Other Drugs: Loperamide: In a clinical drug interaction study in healthy subjects, coadministration of a single 8 mg dose of loperamide with a single 400 mg abemaciclib (2.7 times the approved recommended 150 mg dosage) increased loperamide AUC0-INF by 9% and Cmax by 35% relative to loperamide alone. These increases in loperamide exposure are not considered clinically relevant.
Metformin: In a clinical drug interaction study in healthy subjects, coadministration of a single 1000 mg dose of metformin, a clinically relevant substrate of renal OCT2, MATE1, and MATE2-K transporters, with a single 400 mg dose of abemaciclib (2.7 times the approved recommended 150 mg dosage) increased metformin AUC0-INF by 37% and Cmax by 22% relative to metformin alone. Abemaciclib reduced the renal clearance and renal secretion of metformin by 45% and 62%, respectively, relative to metformin alone, without any effect on glomerular filtration rate (GFR) as measured by iohexol clearance and serum cystatin C.
Endocrine Therapies: In clinical studies in patients with breast cancer, there was no clinically relevant effect of abemaciclib on the pharmacokinetics of fulvestrant, anastrozole, letrozole, exemestane, or tamoxifen.
CYP Metabolic Pathways: In a clinical drug interaction study in patients with cancer, multiple doses of abemaciclib (200 mg twice daily for 7 days) did not result in clinically meaningful changes in the pharmacokinetics of CYP1A2, CYP2C9, CYP2D6 and CYP3A4 substrates. Abemaciclib is a substrate of CYP3A4, and time-dependent changes in pharmacokinetics of abemaciclib as a result of autoinhibition of its metabolism were not observed.
In Vitro Studies: Transporter Systems: Abemaciclib and its major active metabolites inhibit the renal transporters OCT2, MATE1, and MATE2-K at concentrations achievable at the approved recommended dosage. The observed serum creatinine increase in clinical studies with abemaciclib is likely due to inhibition of tubular secretion of creatinine via OCT2, MATE1, and MATE2-K [see Clinical Studies Experience under Adverse Reactions]. Abemaciclib and its major metabolites at clinically relevant concentrations do not inhibit the hepatic uptake transporters OCT1, OATP1B1, and OATP1B3 or the renal uptake transporters OAT1 and OAT3.
Abemaciclib is a substrate of P-gp and BCRP. Abemaciclib and its major active metabolites, M2 and M20, are not substrates of hepatic uptake transporters OCT1, organic anion transporting polypeptide 1B1 (OATP1B1), or OATP1B3.
Abemaciclib inhibits P-gp and BCRP. The clinical consequences of this finding on sensitive P-gp and BCRP substrates are unknown.
P-gp and BCRP Inhibitors: In vitro, abemaciclib is a substrate of P-gp and BCRP. The effect of P-gp or BCRP inhibitors on the pharmacokinetics of abemaciclib has not been studied.
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Abemaciclib was assessed for carcinogenicity in a 2-year rat study. Abemaciclib was not carcinogenic in male and female rats at oral doses up to 3 mg/kg/day (approximately 1 time the exposure at the maximum recommended human dose based on AUC).
Abemaciclib and its active human metabolites M2 and M20 were not mutagenic in a bacterial reverse mutation (Ames) assay or clastogenic in an in vitro chromosomal aberration assay in Chinese hamster ovary cells or human peripheral blood lymphocytes. Abemaciclib, M2, and M20 were not clastogenic in an in vivo rat bone marrow micronucleus assay.
Abemaciclib may impair fertility in males of reproductive potential. In repeat-dose toxicity studies up to 3-months duration, abemaciclib-related findings in the testis, epididymis, prostate, and seminal vesicle at doses ≥10 mg/kg/day in rats and ≥0.3 mg/kg/day in dogs included decreased organ weights, intratubular cellular debris, hypospermia, tubular dilatation, atrophy, and degeneration/necrosis. These doses in rats and dogs resulted in approximately 2 and 0.02 times, respectively, the exposure (AUC) in humans at the maximum recommended human dose. In a rat male fertility study, abemaciclib had no effects on mating and fertility at oral doses up to 10 mg/kg/day (approximately 2 times the exposure at the maximum recommended human dose based on AUC).
In a rat female fertility and early embryonic development study, abemaciclib did not affect mating and fertility at doses up to 20 mg/kg/day (approximately 3 times the exposure at the maximum recommended human dose based on AUC).
Animal Toxicology and/or Pharmacology: In repeat-dose toxicity studies up to 6-months duration, oral administration of abemaciclib resulted in retinal atrophy of the eyes in mice at a dose of 150 mg/kg/day (approximately 10 times the exposure at the maximum recommended human dose based on AUC) and in rats at a dose of 30 mg/kg/day (approximately 5 times the exposure at the maximum recommended human dose based on AUC). In a 2-year rat carcinogenicity study, oral administration of abemaciclib resulted in retinal atrophy in the eyes at doses ≥0.3 mg/kg/day (approximately 0.05 times the exposure at the maximum recommended human dose based on AUC).