


 Sign Out
Sign Out


Posology: The rapid metabolism of accumulated sphingomyelin (SM) by olipudase alfa generates pro-inflammatory breakdown products, which may induce infusion-associated reactions and/or transient liver enzyme elevations. A dose escalation regimen can minimise the majority of these adverse events (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Xenpozyme dose is based on the actual body weight for patient with a body mass index (BMI) ≤ 30 or an optimal body weight for patient with a BMI > 30 (see as follows for patients with a BMI > 30).
Adults: Dose escalation phase: The recommended starting dose of Xenpozyme is 0.1 mg/kg* for adults (also see missed doses subsection for additional guidance) and subsequently, the dose should be increased according to the dose escalation regimen presented in Table 7: (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMaintenance phase: The recommended maintenance dose of Xenpozyme is 3 mg/kg* every 2 weeks.
*Actual body weight will be used for patients with a BMI ≤ 30. For patients with a BMI > 30, an optimal body weight will be used as described as follows.
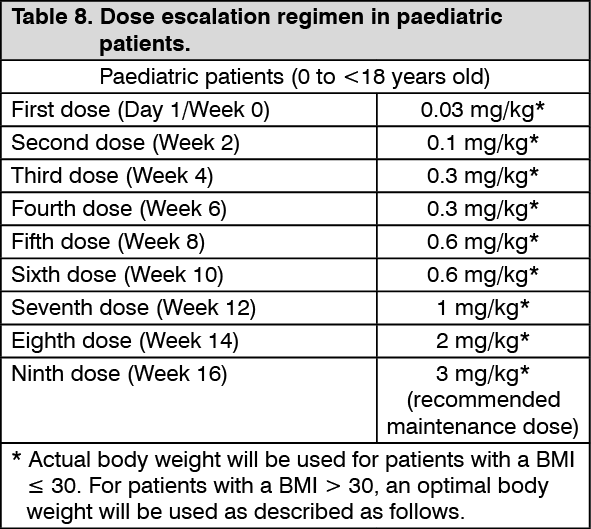
Paediatric population: Dose escalation phase: The recommended starting dose of Xenpozyme is 0.03 mg/kg* for paediatric patients, and the dose should be subsequently increased according to the dose escalation regimen presented in Table 8: (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMaintenance phase: The recommended maintenance dose of Xenpozyme is 3 mg/kg* every 2 weeks.
*Actual body weight will be used for patients with a BMI ≤ 30. For patients with a BMI > 30, an optimal body weight will be used as described as follows.
Patients with BMI > 30: In adult and paediatric patients with a body mass index (BMI) > 30, the body weight that is used to calculate the dose of Xenpozyme is estimated via the following method (for dose escalation and maintenance phases).
Body weight (kg) to be used for dose calculation = 30 x (actual height in m)2.
Example: For a patient with: BMI of 38, body weight of 110 kg, height of 1.7 m.
The dose to be administered will be calculated using a body weight of 30 x 1.72 = 86.7 kg.
Missed doses: A dose is considered missed when not administered within 3 days of the scheduled date. When a dose of Xenpozyme is missed, the next dose should be administered as described as follows as soon as possible. Thereafter, administrations should be scheduled every 2 weeks from the date of the last administration.
During the dose escalation phase: If 1 infusion is missed: the last tolerated dose should be administered, before resuming dose escalation according to the regimen in adults (Table 7) or in paediatric patients (Table 8).
If 2 consecutive infusions are missed: 1 dose level lower than the last tolerated dose (using a minimal dose of 0.3 mg/kg) should be administered, before resuming dose escalation according to Table 7 or Table 8.
If 3 or more consecutive infusions are missed: dose escalation should be resumed at 0.3 mg/kg according to Table 7 or Table 8.
At the next scheduled infusion after a missed dose, if the dose administered is 0.3 or 0.6 mg/kg, that dose should be administered twice as per Table 7 and Table 8.
During the maintenance phase: If 1 maintenance infusion is missed: the maintenance dose should be administered and the treatment schedule adjusted accordingly.
If 2 consecutive maintenance infusions are missed: 1 dose below the maintenance dose (i.e. 2 mg/kg) should be administered. Then for subsequent infusions, the maintenance dose (3 mg/kg) every 2 weeks should be administered.
If 3 or more consecutive maintenance infusions are missed: dose escalation should be resumed at 0.3 mg/kg according to Table 7 or Table 8.
Monitoring of transaminase level: Transaminase (alanine aminotransferase [ALT] and aspartate aminotransferase [AST]) levels should be obtained prior to treatment initiation and monitored during any dose escalation phases (see Precautions). If the pre-infusion transaminase levels are elevated above baseline and > 2 times the upper limit of normal (ULN), the Xenpozyme dose can be adjusted (prior dose repeated or reduced) or treatment can be temporarily withheld in accordance with the degree of transaminase elevation. If a patient requires a dose adjustment or treatment interruption, treatment re-initiation should follow the dose escalation regimen described in Table 7 and Table 8 for adult and paediatric patients, respectively, and recommendations in case of missed doses (see missed doses as previously mentioned).
Special populations: Elderly patients: No dose adjustment is recommended for patients over the age of 65 (see Pharmacology: Pharmacokinetics under Actions).
Hepatic impairment: No dose adjustment is recommended in patients with hepatic impairment (see Pharmacology: Pharmacokinetics under Actions).
Renal impairment: No dose adjustment is recommended in patients with renal impairment (see Pharmacology: Pharmacokinetics under Actions).
Method of administration: Xenpozyme is for intravenous use only. Infusions should be administered in a stepwise manner preferably using an infusion pump.
For instructions on reconstitution and dilution of the medicinal product before administration, see Special precautions for disposal and other handling under Cautions for Usage.
After reconstitution and dilution, the solution is administered as an intravenous infusion. The infusion rates must be incrementally increased during the infusion only in the absence of infusion-associated reactions (see Precautions in case of infusion-associated reactions). The infusion rate and duration of infusion (+/- 5 min) for each step of infusion are detailed in Table 9 and Table 10: (See Tables 9 and 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSigns and symptoms of infusion-associated reactions (IARs), such as headache, urticaria, pyrexia, nausea and vomiting, and other signs or symptoms of hypersensitivity should be monitored during the infusion. Depending on the symptom severity, the infusion may be slowed, paused or discontinued and appropriate medical treatment initiated as needed.
In case of severe hypersensitivity and/or anaphylactic reaction, treatment with Xenpozyme should be discontinued immediately (see Precautions).
At the end of infusion (once the syringe or infusion bag is empty), the infusion line should be flushed with sodium chloride 9 mg/mL (0.9%) solution for injection using the same infusion rate as the one used for the last part of the infusion.
Home infusion during maintenance phase: Home infusion under the supervision of a healthcare professional may be considered for patients on maintenance dose and who are tolerating their infusions well. The decision to have patients moved to home infusion should be made after evaluation and recommendation by the prescribing physician.
Appropriate medical support, including personnel trained in emergency measures, should be readily available when Xenpozyme is administered. If anaphylactic or other acute reactions occur, immediately discontinue the Xenpozyme infusion, initiate appropriate medical treatment and seek the attention of a physician. If severe hypersensitivity reactions occur, subsequent infusions should only occur in a setting where resuscitation measures are available. Dose and infusion rates should remain constant while at home, and should not be changed without supervision of the prescribing physician. In case of missed doses or delayed infusion, the prescribing physician should be contacted.