The information highlighted (if any) are the most recent updates for this brand.
VIAGRA 50 mg: Each tablet contains sildenafil citrate equivalent to 50 mg sildenafil.
VIAGRA 100 mg: Each tablet contains sildenafil citrate equivalent to 100 mg sildenafil.
For excipients, see as follows.
Excipients/Inactive Ingredients: In addition to the active ingredient, sildenafil citrate, each tablet contains the following inactive ingredients: microcrystalline cellulose, calcium hydrogen phosphate (anhydrous), croscarmellose sodium, magnesium stearate, hydroxypropyl methylcellulose (hypromellose), titanium dioxide (E171), lactose, triacetin, and FD & C Blue #2 aluminum lake (indigo carmine aluminium lake [E132]).
Pharmacology: Pharmacodynamics: Sildenafil, an oral therapy for erectile dysfunction, is the citrate salt of sildenafil, a selective inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type 5 (PDE5).
Mechanism of Action: The physiologic mechanism of erection of the penis involves release of nitric oxide (NO) in the corpus cavernosum during sexual stimulation.
NO then activates the enzyme guanylate cyclase, which results in increased levels of cyclic guanosine monophosphate (cGMP), producing smooth muscle relaxation in the corpus cavernosum and allowing inflow of blood.
Sildenafil has no direct relaxant effect on isolated human corpus cavernosum, but enhances the effect of NO by inhibiting of phosphodiesterase type 5 (PDE5), which is responsible for degradation of cGMP in the corpus cavernosum.
When sexual stimulation causes local release of NO, inhibition of PDE5 by sildenafil causes increased levels of cGMP in the corpus cavernosum, resulting in smooth muscle relaxation and inflow of blood to the corpus cavernosum.
Sildenafil at recommended doses has no effect in the absence of sexual stimulation.
Studies in vitro have shown that sildenafil is selective for PDE5.
Its effect is more potent on PDE5 than on other known phosphodiesterases (10-fold for PDE6, >80-fold for PDE1, >700-fold for PDE2, PDE3, and PDE4, PDE7 - PDE11).
The approximately 4,000-fold selectivity for PDE5 versus PDE3 is important because PDE3 is involved in the control of cardiac contractility.
Clinical studies: Cardiac: Single oral doses of sildenafil up to 100 mg produced no clinically relevant changes in the ECGs of normal male volunteers.
The mean maximum decreases in supine systolic blood pressure following 100 mg oral dosing was 8.3 mmHg. The corresponding change in supine diastolic blood pressure was 5.3 mmHg.
Larger but similarly transient effects on blood pressure were recorded among patients receiving concomitant nitrates (see Contraindications and Interactions).
In a study of the hemodynamic effects of a single oral 100 mg dose of sildenafil in 14 patients with severe coronary artery disease (CAD) (>70% stenosis of at least one coronary artery), the mean resting systolic and diastolic blood pressures decreased by 7% and 6%, respectively compared to baseline. Mean pulmonary systolic blood pressure decreased by 9%. Sildenafil showed no effect on cardiac output, and did not impair blood flow through the stenosed coronary arteries, and resulted in improvement (approximately 13%) in adenosine-induced coronary flow reserve (in both stenosed and reference arteries).
In a double-blind, placebo-controlled trial, 144 patients with erectile dysfunction and stable angina, who were taking their regular antianginal medications (except nitrates) were exercised until limiting angina occurred. The duration of treadmill exercise was statistically significantly longer (19.9 seconds; 95% confidence interval: 0.9-38.9 seconds) in the evaluable patients who had taken a single dose of sildenafil 100 mg compared to patients who had taken a single dose of placebo. The mean exercise times (adjusted for baseline) to the onset of limiting angina were 423.6 and 403.7 seconds for sildenafil and placebo, respectively.
A randomized, double-blind, placebo-controlled, flexible-dose study (sildenafil up to 100 mg) in males (N=568) with erectile dysfunction and arterial hypertension taking two or more antihypertensive agents was conducted. Sildenafil improved the erections in 71% of men compared to 18% in the placebo group, and 62% of attempts at sexual intercourse were successful with sildenafil compared to 26% on placebo. The incidence of adverse events was consistent with observations in other patient populations, as well as in the subjects taking three or more antihypertensive agents.
Visual: Mild and transient differences in colour discrimination (blue/green) were detected in some subjects using the Farnsworth-Munsell 100 hue test at 60 minutes following a 100 mg dose, with no effects evident after 120 minutes post-dose. The postulated mechanism for this change in colour discrimination is related to inhibition of PDE6, which is involved in the phototransduction cascade of the retina. In vitro studies show that sildenafil is 10-fold less potent against PDE6 than PDE5. Sildenafil has no effect on visual acuity, contrast sensitivity, electroretinograms, intraocular pressure, or pupillometry.
In a placebo-controlled, crossover study of patients with documented early age-related macular degeneration (n=9), sildenafil (single dose, 100 mg) was well-tolerated and demonstrated no clinically significant changes in the visual tests conducted (visual acuity, Amsler grid, color discrimination, simulated traffic light, Humphrey perimeter and photostress).
Efficacy: The efficacy and safety of sildenafil was evaluated in 21 randomized, double-blind, placebo-controlled trials of up to 6 months duration. Sildenafil was administered to more than 3000 patients aged 19-87, with ED of various etiologies (organic, psychogenic, mixed). The efficacy was evaluated by global assessment question, diary of erections, the International Index of Erectile Function (IIEF, a validated sexual function questionnaire) and a partner questionnaire.
Sildenafil efficacy, determined as the ability to achieve and maintain an erection sufficient for sexual intercourse, was demonstrated in all 21 studies and was maintained in long-term extension studies (one year). In fixed-dose studies, the proportions of patients reporting that treatment improved their erections were 62% (25 mg), 74% (50 mg) and 82% (100 mg) compared to 25% on placebo. In addition to improvements in erectile dysfunction, analysis of the IIEF showed that sildenafil treatment also improved the domains of orgasm, satisfaction with intercourse and overall satisfaction.
Across all trials, the proportions of patients reporting improvement on sildenafil were 59% of diabetic patients, 43% of radical prostatectomy patients and 83% of patients with spinal cord injury (versus 16%, 15% and 12% on placebo respectively).
Pharmacokinetics: Sildenafil pharmacokinetics are dose-proportional over the recommended dose range.
It is eliminated predominantly by hepatic metabolism (mainly cytochrome P450 3A4) and is converted to an active metabolite with properties similar to the parent, sildenafil.
Absorption: Sildenafil is rapidly absorbed after oral administration, with mean absolute bioavailability of 41% (range 25%-63%).
Sildenafil inhibits the human PDE5 enzyme in vitro by 50% at a concentration of 3.5 nM. In man, the mean maximum free plasma concentration of sildenafil following a single oral dose of 100 mg is approximately 18 ng/mL, or 38 nM.
Maximum observed plasma concentrations are reached within 30 to 120 minutes (median 60 minutes) of oral dosing in the fasted state.
When sildenafil film-coated tablets are taken with a high fat meal, the rate of absorption of sildenafil is reduced, with a mean delay in Tmax of 60 minutes and a mean reduction in Cmax of 29%, however, the extent of absorption was not significantly affected (AUC decreased by 11%).
Distribution: The mean steady-state volume of distribution (Vss) for sildenafil is 105 L, indicating distribution into the tissues.
Sildenafil and its major circulating N-desmethyl metabolite are both approximately 96% bound to plasma proteins.
Protein binding is independent of total drug concentrations.
Based upon measurements of sildenafil in semen of healthy volunteers 90 minutes after dosing, less than 0.0002% (average 188 ng) of the administered dose may appear in the semen of patients.
Metabolism: Sildenafil is cleared predominantly by the CYP3A4 (major route) and CYP2C9 (minor route) hepatic microsomal isoenzymes.
The major circulating metabolite results from N-desmethylation of sildenafil, and is itself further metabolized.
This metabolite has a PDE selectivity profile similar to sildenafil and an in vitro potency for PDE5 approximately 50% of the parent drug.
In healthy volunteers, plasma concentrations of this metabolite are approximately 40% of those seen for sildenafil.
The N-desmethyl metabolite is further metabolized, with a terminal half-life of approximately 4 hours.
Elimination: The total body clearance of sildenafil is 41 L/h with a resultant terminal phase half-life of 3-5 hours. After either oral or intravenous administration, sildenafil is excreted as metabolites predominantly in the feces (approximately 80% of administered oral dose) and to a lesser extent in the urine (approximately 13% of the administered oral dose).
Pharmacokinetics in special patient groups: Elderly: Healthy elderly volunteers (65 years or over) had a reduced clearance of sildenafil, resulting in approximately 90% higher plasma concentrations of sildenafil and the active N-desmethyl metabolite compared to those seen in healthy younger volunteers (18-45 years). Due to age-differences in plasma protein binding, the corresponding increase in free sildenafil plasma concentration was approximately 40%.
Renal Insufficiency: In volunteers with mild (creatinine clearance = 50-80 mL/min) and moderate (creatinine clearance = 30-49 mL/min) renal impairment, the pharmacokinetics of a single oral dose of sildenafil (50 mg) were not altered.
In volunteers with severe (creatinine clearance = <30 mL/min) renal impairment, sildenafil clearance was reduced, resulting in approximately doubling of AUC (100%) and Cmax (88%) compared to age-matched volunteers with no renal impairment (see Dosage & Administration).
In addition, N-desmethyl metabolite AUC and Cmax values were significantly increased by 200% and 79% respectively in subjects with severe renal impairment compared to subjects with normal renal function.
Hepatic Insufficiency: In volunteers with hepatic cirrhosis (Child-Pugh A and B), sildenafil clearance was reduced, resulting in increases in AUC (85%) and Cmax (47%) compared to age-matched volunteers with no hepatic impairment (see Dosage & Administration). The pharmacokinetics of sildenafil in patients with severely impaired hepatic function (Child-Pugh class C) have not been studied.
Toxicology: Preclinical safety data: No evidence of drug related carcinogenicity was revealed in a 24-month study in rats at doses up to 42 times the Maximum Recommended Human Dose (MRHD) on a mg/kg basis and approximately five times the MRHD on a mg/m2 bases) and in an 18-21 month study in mice at doses up to 21 times the MRHD on a mg/kg basis (approximately two times the MRHD on a mg/m2 basis).
Bacterial and in vivo mutagenicity tests were negative.
There was no effect on sperm motility or morphology after single 100 mg oral doses of sildenafil in healthy volunteers.
Sildenafil is indicated for the treatment of erectile dysfunction, which is the inability to achieve or maintain a penile erection sufficient for satisfactory sexual performance.
In order for sildenafil to be effective, sexual stimulation is required.
Sildenafil tablets are for oral administration.
Use in adults: For most patients, the recommended dose is 50 mg taken, as needed, approximately 1 hour before sexual activity. Based on effectiveness and toleration, the dose may be increased to a maximum recommended dose of 100 mg or decreased to 25 mg. The maximum recommended daily dose is 100 mg. The maximum recommended dosing frequency is once per day.
Use in patients with impaired renal function: Dosage adjustments are not required in patients with mild to moderate renal impairment (creatinine clearance = 30 - 80 mL/min).
Since sildenafil clearance is reduced in patients with severe renal impairment (creatinine clearance <30 mL/min), a 25 mg dose should be considered.
Use in patients with impaired hepatic function: Since sildenafil clearance is reduced in patients with hepatic impairment (e.g., cirrhosis), a 25 mg dose should be considered.
Use in patients using other medications: Given the extent of the interaction with patients receiving concomitant therapy with ritonavir (see Interactions), it is recommended not to exceed a maximum single dose of 25 mg of sildenafil in a 48-hour period.
A starting dose of 25 mg should be considered in patients receiving concomitant treatment with the CYP3A4 inhibitors (e.g., erythromycin, saquinavir, ketoconazole, itraconazole) see Interactions.
In order to minimize the potential for developing postural hypotension, patients should be stable on alpha-blocker therapy prior to initiating sildenafil treatment. In addition, initiation of sildenafil at lower doses should be considered (see Precautions and Interactions).
Use in children: Sildenafil is not indicated for use in children (<18 years old).
Use in elderly men: Dosage adjustments are not required in elderly patients.
In studies with healthy volunteers of single doses up to 800 mg, adverse events were similar to those seen at lower doses but incidence rates and severities were increased.
In cases of overdose, standard supportive measures should be adopted as required.
Renal dialysis is not expected to accelerate clearance as sildenafil is highly bound to plasma proteins and it is not eliminated in the urine.
Use of sildenafil is contraindicated in patients with a known hypersensitivity to any component of the tablet.
Sildenafil was shown to potentiate the hypotensive effects of acute and chronic nitrates, and its administration to patients who are concurrently using nitric oxide donors, organic nitrates or organic nitrites in any form either regularly or intermittently is therefore contraindicated (see Interactions).
The co-administration of PDE5 inhibitors, including sildenafil, with guanylate cyclase stimulators, such as riociguat, is contraindicated as it may potentially lead to symptomatic hypotension.
Patients should not be prescribed VIAGRA if they are taking Nitrates (see CONTRAINDICATIONS).
VIAGRA is contraindicated in men for whom sexual intercourse is inadvisable due to cardiovascular risk factors (see CONTRAINDICATIONS and PRECAUTIONS).
A thorough medical history and physical examination should be undertaken to diagnose erectile dysfunction, determine potential underlying causes, and identify appropriate treatment.
There is a degree of cardiac risk associated with sexual activity; therefore, physicians may wish to consider the cardiovascular status of their patients prior to initiating any treatment for erectile dysfunction.
Agents for the treatment of erectile dysfunction should not be used in men for whom sexual activity is inadvisable.
Serious cardiovascular events, including myocardial infarction, sudden cardiac death, ventricular arrhythmia, cerebrovascular hemorrhage and transient ischemic attack have been reported post-marketing in temporal association with the use of sildenafil for erectile dysfunction. Most, but not all, of these patients had pre-existing cardiovascular risk factors. Many of these events were reported to occur during or shortly after sexual activity, and a few were reported to occur shortly after the use of sildenafil without sexual activity. Others were reported to have occurred hours to days after the use of sildenafil and sexual activity. It is not possible to determine whether these events are related directly to sildenafil, to sexual activity, to the patient's underlying cardiovascular disease, to a combination of these factors, or to other factors.
In clinical trials, sildenafil has been shown to have systemic vasodilatory properties that result in transient decreases in blood pressure (see Pharmacology: Pharmacodynamics under Actions). This is of little or no consequence in most patients. However, prior to prescribing sildenafil, physicians should carefully consider whether their patients with certain underlying conditions could be adversely affected by such vasodilatory effects, especially in combination with sexual activity. Patients with increased susceptibility to vasodilators include those with left ventricular outflow obstruction (e.g., aortic stenosis, hypertrophic obstructive cardiomyopathy), or those with the rare syndrome of multiple system atrophy manifesting as severely impaired autonomic control of blood pressure.
Non-arteritic anterior ischemic optic neuropathy (NAION), a rare condition and a cause of decreased vision or loss of vision, has been reported rarely post-marketing with the use of all PDE5 inhibitors, including sildenafil. Most of these patients had risk factors such as low cup to disc ratio ("crowded disc"), age over 50, diabetes, hypertension, coronary artery disease, hyperlipidemia and smoking. An observational study evaluated whether recent use of PDE5 inhibitors, as a class, was associated with acute onset of NAION. The results suggest an approximate 2-fold increase in the risk of NAION within 5 half-lives of PDE5 inhibitor use. Based on published literature, the annual incidence of NAION is 2.5-11.8 cases per 100,000 males aged ≥50 per year in the general population. In case of sudden visual loss, patients should be advised to stop taking sildenafil and consult a physician immediately.
Individuals who have already experienced NAION are at increased risk of NAION recurrence. Therefore physicians should discuss this risk with these patients and whether they could be adversely affected by use of PDE5 inhibitors. PDE5 inhibitors, including sildenafil, should be used with caution in these patients and only when the anticipated benefits outweigh the risks.
Caution is advised when sildenafil is administered to patients taking an alpha-blocker, as the co-administration may lead to symptomatic hypotension in a few susceptible individuals (see Interactions). In order to minimize the potential for developing postural hypotension, patients should be hemodynamically stable on alpha-blocker therapy prior to initiating sildenafil treatment. Initiation of sildenafil at lower doses should be considered (see Dosage & Administration). In addition, physicians should advise patients what to do in the event of postural hypotensive symptoms.
A minority of patients with the inherited condition retinitis pigmentosa have genetic disorders of retinal phosphodiesterases. There is no safety information on the administration of sildenafil to patients with retinitis pigmentosa, therefore, sildenafil should be administered with caution to these patients.
In vitro studies with human platelets indicate that sildenafil potentiates the anti-aggregatory effect of sodium nitroprusside (a nitric oxide donor). There is no safety information on the administration of sildenafil to patients with bleeding disorders or active peptic ulceration, therefore sildenafil should be administered with caution to these patients.
Agents for the treatment of erectile dysfunction should be used with caution in patients with anatomical deformation of the penis (such as angulation, cavernosal fibrosis or Peyronie's disease), or in patients who have conditions which may predispose them to priapism (such as sickle cell anemia, multiple myeloma or leukemia).
Prolonged erections and priapism have been reported with sildenafil in post-marketing experience. In the event of an erection that persists longer than 4 hours, the patient should seek immediate medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency could result.
The safety and efficacy of combinations of sildenafil with other PDE5 inhibitors, or other pulmonary arterial hypertension (PAH) treatments containing sildenafil (REVATIO), or other treatments for erectile dysfunction have not been studied, and the use of such combinations is not recommended.
Sudden decrease or loss of hearing has been reported in a small number of post-marketing and clinical trials cases with the use of all PDE5 inhibitors, including sildenafil. Most of these patients had risk factors for sudden decrease or loss of hearing. No causal relationship has been made between the use of PDE5 inhibitors and sudden decrease or loss of hearing. In case of sudden decrease or loss of hearing patients should be advised to stop taking sildenafil and consult a physician promptly.
Effects on ability to drive and use machines: As dizziness and altered vision were reported in clinical trials with sildenafil, patients should be aware of how they react to sildenafil, before driving or operating machinery. The effect of sildenafil on the ability to drive and use machinery has not been studied.
Sildenafil is not indicated for use in women.
No teratogenic effects, impairment of fertility or adverse effects on peri-/post-natal development were found in reproduction studies in rats and rabbits following oral administration of sildenafil.
There are no adequate and well-controlled studies in pregnant or lactating women.
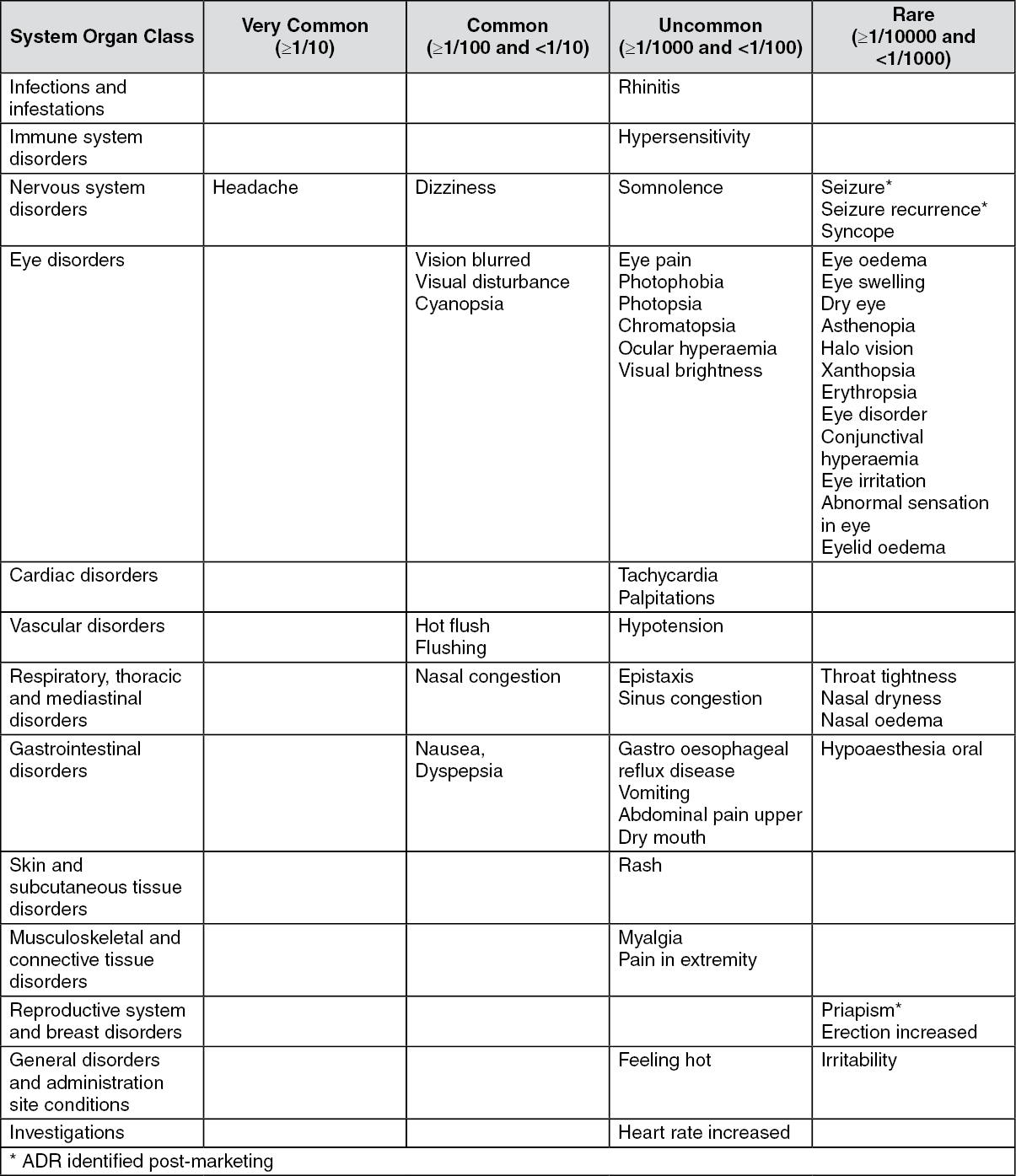
The adverse events were generally transient and mild to moderate in nature.
In fixed-dose studies, the incidence of some adverse events increased with dose.
The nature of the adverse events in flexible-dose studies, which more closely reflect the recommended dosage regimen, was similar to that for fixed-dose studies.
The most commonly reported adverse reactions were headache and flushing.
Adverse reactions reported in clinical trials and post-marketing surveillance are presented in Table as follows: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
At doses above the recommended dose range, adverse events were similar to those detailed previously but generally were reported more frequently.
In an analysis of double-blind placebo-controlled clinical trials encompassing over 700 person-years of observation on placebo and over 1300 person-years on sildenafil, there were no differences in the incidence rate of myocardial infarction (MI) or in the rate of cardiovascular mortality for patients receiving sildenafil compared to those receiving placebo. The rates of MI were 1.1 per 100 person-years for men receiving sildenafil and for those receiving placebo. The rates of cardiovascular mortality were 0.3 per 100 person-years for men receiving sildenafil and those receiving placebo.
Effects of other medicinal products on sildenafil: In vitro studies: Sildenafil metabolism is principally mediated by the cytochrome P450 (CYP) isoforms 3A4 (major route) and 2C9 (minor route). Therefore, inhibitors of these isoenzymes may reduce sildenafil clearance and inducers of these isoenzymes may increase sildenafil clearance.
In vivo studies: Population pharmacokinetic analysis of clinical trial data indicated a reduction in sildenafil clearance when co-administered with CYP3A4 inhibitors (such as ketoconazole, erythromycin, cimetidine).
Cimetidine (800 mg), a cytochrome P450 inhibitor and a non-specific CYP3A4 inhibitor, caused a 56% increase in plasma sildenafil concentrations when co-administered with sildenafil (50 mg) to healthy volunteers.
When a single 100 mg dose of sildenafil was administered with erythromycin, a moderate CYP3A4 inhibitor, at steady-state (500 mg twice daily for 5 days), there was a 182% increase in sildenafil systemic exposure (AUC). In addition, co-administration of the HIV protease inhibitor saquinavir, also a CYP3A4 inhibitor, at steady-state (1200 mg three times daily) with sildenafil (100 mg single dose) resulted in a 140% increase in sildenafil Cmax and a 210% increase in sildenafil AUC. Sildenafil had no effect on saquinavir pharmacokinetics (see Dosage & Administration). Stronger CYP3A4 inhibitors such as ketoconazole and itraconazole would be expected to have greater effects.
Co-administration with the HIV protease inhibitor ritonavir, which is a highly potent P450 inhibitor, at steady-state (500 mg twice daily) with sildenafil (100 mg single dose) resulted in a 300% (4-fold) increase in sildenafil Cmax and a 1000% (11-fold) increase in sildenafil plasma AUC. At 24 hours, the plasma levels of sildenafil were still approximately 200 ng/mL, compared to approximately 5 ng/mL when sildenafil was dosed alone. This is consistent with ritonavir's marked effects on a broad range of P450 substrates. Sildenafil had no effect on ritonavir pharmacokinetics see Dosage & Administration.
When the dose of sildenafil for subjects receiving potent CYP3A4 inhibitors was administered as recommended, the maximum free plasma sildenafil concentration did not exceed 200 nM for any individual and was consistently well tolerated.
Single doses of antacid (magnesium hydroxide/aluminium hydroxide) did not affect the bioavailability of sildenafil.
In a study of healthy male volunteers, co-administration of the endothelin antagonist, bosentan, (an inducer of CYP3A4 [moderate], CYP2C9 and possibly of CYP2C19) at steady-state (125 mg twice a day) with sildenafil at steady-state (80 mg three times a day) resulted in 62.6% and 55.4% decrease in sildenafil AUC and Cmax, respectively. Sildenafil increased bosentan AUC and Cmax by 49.8% and 42%, respectively. Concomitant administration of strong CYP3A4 inducers, such as rifampin, is expected to cause greater decreases in plasma concentrations of sildenafil.
Pharmacokinetic data from patients in clinical trials showed no effect on sildenafil pharmacokinetics of CYP2C9 inhibitors (such as tolbutamide, warfarin), CYP2D6 inhibitors (such as selective serotonin reuptake inhibitors, tricyclic antidepressants), thiazide and related diuretics, angiotensin converting enzyme (ACE) inhibitors, and calcium channel blockers.
In healthy male volunteers, there was no evidence of an effect of azithromycin (500 mg daily for 3 days) on the AUC, Cmax, Tmax, elimination rate constant, or subsequent half-life of sildenafil or its major circulating metabolite.
Effects of sildenafil on other medicinal products: In vitro studies: Sildenafil is a weak inhibitor of the cytochrome P450 isoforms 1A2, 2C9, 2C19, 2D6, 2E1 and 3A4 (IC50 > 150 μM).
Given sildenafil peak plasma concentrations of approximately 1 μM after recommended doses, it is unlikely that sildenafil will alter the clearance of substrates of these isoenzymes.
In vivo studies: Sildenafil was shown to potentiate the hypotensive effect of acute and chronic nitrates. Therefore, use of nitric oxide donors, organic nitrates, or organic nitrites in any form either regularly or intermittently with sildenafil is contraindicated (see Contraindications).
In three specific drug-drug interaction studies, the alpha-blocker doxazosin (4 mg and 8 mg) and sildenafil (25 mg, 50 mg, or 100 mg) were administered simultaneously to patients with benign prostatic hyperplasia (BPH) stabilized on doxazosin therapy. In these study populations, mean additional reductions of supine blood pressure of 7/7 mmHg, 9/5 mmHg, and 8/4 mmHg, and mean additional reductions of standing blood pressure of 6/6 mmHg, 11/4 mmHg, and 4/5 mmHg, respectively, were observed. When sildenafil and doxazosin were administered simultaneously to patients stabilized on doxazosin therapy, there were infrequent reports of patients who experienced symptomatic postural hypotension. These reports included dizziness and light-headedness, but not syncope. Concomitant administration of sildenafil to patients taking alpha-blocker therapy may lead to symptomatic hypotension in a few susceptible individuals (see Dosage & Administration and Precautions).
No significant interactions were shown when sildenafil (50 mg) was co-administered with tolbutamide (250 mg) or warfarin (40 mg), both of which are metabolized by CYP2C9.
Sildenafil (100 mg) did not affect the steady-state pharmacokinetics of the HIV protease inhibitors, saquinavir and ritonavir, both of which are CYP3A4 substrates (see previously mentioned, Effects of other medicinal products on sildenafil).
Sildenafil at steady-state (80 mg three times a day) resulted in a 49.8% increase in bosentan AUC and a 42% increase in bosentan Cmax (125 mg twice a day) (see previously mentioned, Effects of other medicinal products on sildenafil).
Sildenafil (50 mg) did not potentiate the increase in bleeding time caused by aspirin (150 mg).
Sildenafil (50 mg) did not potentiate the hypotensive effect of alcohol in healthy volunteers with mean maximum blood alcohol levels of 0.08% (80 mg/dL).
No interaction was seen when sildenafil (100 mg) was co-administered with amlodipine in hypertensive patients. The mean additional reduction on supine systolic blood pressure was 8 mmHg systolic and 7 mmHg diastolic.
Analysis of the safety database showed no difference in the side effect profile in patients taking sildenafil with and without antihypertensive medication.
Special precautions for disposal: No special instructions.
Incompatibilities: Not applicable.
Do not store above 30°C. Keep tablets in the original package, protected from moisture.
G04BE03 - sildenafil ; Belongs to the class of drugs used in erectile dysfunction.
Viagra FC tab 100 mg
1's;4's
Viagra FC tab 50 mg
1's;4's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
