Trevive Tablets 100 mg: Each film-coated tablet contains imatinib mesylate equivalent to imatinib 100 mg.
Trevive Tablets 400 mg: Each film-coated tablet contains imatinib mesylate equivalent to imatinib 400 mg.
Pharmacotherapeutic group: protein-tyrosine kinase inhibitor. ATC code: L01XE01.
Pharmacology: Pharmacodynamics: Mechanism of action: Imatinib is a small molecule protein-tyrosine kinase inhibitor that potently inhibits the activity of the Bcr-Abl tyrosine kinase (TK), as well as several receptor TKs: Kit, the receptor for stem cell factor (SCF) coded for by the c-Kit proto-oncogene, the discoidin domain receptors (DDR1 and DDR2), the colony stimulating factor receptor (CSF-1R) and the platelet-derived growth factor receptors alpha and beta (PDGFR-alpha and PDGFR-beta). Imatinib can also inhibit cellular events mediated by activation of these receptor kinases.
Pharmacodynamics effects: Imatinib is a protein-tyrosine kinase inhibitor which potently inhibits the Bcr-Abl tyrosine kinase at the in vitro, cellular and in vivo levels. The compound selectively inhibits proliferation and induces apoptosis in Bcr-Abl positive cell lines as well as fresh leukaemic cells from Philadelphia chromosome positive CML and acute lymphoblastic leukaemia (ALL) patients. In colony transformation assays using ex vivo peripheral blood and bone marrow samples, Imatinib shows selective inhibition of BCR-ABL positive colonies from CML patients.
In vivo the compound shows anti-tumour activity as a single agent in animal models using BcrAbl positive tumour cells.
Imatinib is also an inhibitor of the receptor tyrosine kinases for platelet-derived growth factor (PDGF) and stem cell factor (SCF), c-Kit, and inhibits PDGF- and SCF-mediated cellular events.
In vitro, imatinib inhibits proliferation and induces apoptosis in gastrointestinal stromal tumour (GIST) cells, which express an activating kit mutation. Constitutive activation of the PDGF or the ABL protein tyrosine kinases as a consequence of fusion to diverse partner proteins or constitutive production of PDGF have been implicated in the pathogenesis of MDS/MPD, HES/CEL and DFSP. In addition, constitutive activation of c-KIT or the PDGFR has been implicated in the pathogenesis of ASM. Imatinib inhibits signalling and proliferation of cells driven by dysregulated PDGFR and Abl kinase activity.
Pharmacokinetics: Pharmacokinetics of Imatinib Tablets: The pharmacokinetics of Imatinib Tablets have been evaluated over a dosage range of 25 to 1,000 mg. Plasma pharmacokinetic profiles were analysed on day 1 and on either day 7 or day 28, by which time plasma concentrations had reached steady state.
Absorption: Mean absolute bioavailability for imatinib is 98% .There was high between-patient variability in plasma imatinib AUC levels after an oral dose. When given with a high-fat meal, the rate of absorption of imatinib was minimally reduced with a small reduction in AUC (7.4%) compared to fasting conditions. The effect of prior gastrointestinal surgery on drug absorption has not been investigated.
Distribution: Binding to plasma proteins was approximately 95% on the basis of in vitro experiments, mostly to albumin and alpha-acid-glycoprotein, with little binding to lipoprotein.
Biotransformation: The main circulating metabolite in humans is the N-demethylated piperazine derivative, which shows similar in vitro potency to the parent. The plasma AUC for this metabolite was found to be only 16% of the AUC for imatinib.
The plasma protein binding of the N-demethylated metabolite is similar to that of the parent compound.
Imatinib and the N-demethyl metabolite together accounted for about 65% of the circulating radioactivity (AUC(0-48h)). The remaining circulating radioactivity consisted of a number of minor metabolites.
The in vitro results showed that CYP3A4 was the major human P450 enzyme catalysing the biotransformation of imatinib. Of a panel of potential comedications (acetaminophen, aciclovir, allopurinol, amphotericin, cytarabine, erythromycin, fluconazole, hydroxyurea, norfloxacin, penicillin V) only erythromycin and fluconazole showed inhibition of imatinib metabolism which could have clinical relevance.
Imatinib was shown in vitro to be a competitive inhibitor of marker substrates for CYP2C9, CYP2D6 and CYP3A4/5. Inhibition of CYP2D6 and/or CYP3A4/5-mediated metabolism of coadministered drugs is possible. No interaction is expected upon co-administration of either 5 fluorouracil or paclitaxel and imatinib.
Elimination: After an oral 14C-labelled dose of imatinib, approximately 81% of the dose was recovered within 7 days in faeces (86% of dose) and urine (13% of dose). Unchanged imatinib accounted for 25% of the dose (5% urine, 20% faeces), the remainder being metabolites.
Plasma pharmacokinetics: Following oral administration in healthy volunteers, the t½ was approximately 18h, suggesting that once-daily dosing is appropriate. The increase in mean AUC with increasing dose was linear and dose proportional in the range of 25-1,000 mg imatinib after oral administration. There was no change in the kinetics of imatinib on repeated dosing, and accumulation was 1.5-2.5-fold at steady state when dosed once daily.
Pharmacokinetics in GIST patients: In patients with GIST steady-state exposure was 1.5-fold higher than that observed for CML patients for the same dosage (400 mg daily). Based on preliminary population pharmacokinetic analysis in GIST patients, there were three variables (albumin, WBC and bilirubin) found to have a statistically significant relationship with imatinib pharmacokinetics. Decreased values of albumin caused a reduced clearance (CL/f); and higher levels of WBC led to a reduction of CL/f. However, these associations are not sufficiently pronounced to warrant dose adjustment. In this patient population, the presence of hepatic metastases could potentially lead to hepatic insufficiency and reduced metabolism.
Population pharmacokinetics: In CML patients, there was small effect of age on the volume of distribution which is clinically insignificant. The effect of bodyweight on the clearance of imatinib is not considered sufficient to warrant dose adjustment based on kg bodyweight. There is no effect of gender on the kinetics of imatinib.
Pharmacokinetics in children: As in adult patients, imatinib was rapidly absorbed after oral administration in paediatric patients. Dosing in children at 260 and 340 mg/m2 achieved the same exposure, respectively, as doses of 400 mg and 600 mg in adult patients. A 1.7-fold drug accumulation was observed after repeated once-daily dosing.
Based on pooled population pharmacokinetic analysis in paediatric patients with haematological disorders (CML, Ph+ALL, or other haematological disorders treated with imatinib), clearance of imatinib increases with increasing body surface area (BSA). After correcting for the BSA effect, other demographics such as age, body weight and body mass index did not have clinically significant effects on the exposure of imatinib. The analysis confirmed that exposure of imatinib in paediatric patients receiving 260 mg/m2 once daily (not exceeding 400 mg once daily) or 340 mg/m2 once daily (not exceeding 600 mg once daily) were similar to those in adult patients who received imatinib 400 mg or 600 mg once daily.
Organ function impairment: Imatinib and its metabolites are not excreted via the kidney to a significant extent. Patients with mild and moderate impairment of renal function appear to have a higher plasma exposure than patients with normal renal function. The increase is approximately 1.5- to 2 fold, corresponding to a 1.5-fold elevation of plasma AGP, to which imatinib binds strongly. The free drug clearance of imatinib is probably similar between patients with renal impairment and those with normal renal function, since renal excretion represents only a minor elimination pathway for imatinib.
Although the results of pharmacokinetic analysis showed that there is considerable inter subject variation, the mean exposure to imatinib did not increase in patients with varying degrees of liver dysfunction as compared to patients with normal liver function.
Imatinib Tablets are indicated for the treatment of: adult and pediatric patients with newly diagnosed chronic myeloid leukaemia (CML) as well as for the treatment of adult and pediatric patients with CML in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy.
adult patients with unresectable and/or metastatic malignant gastrointestinal stromal tumours (GIST).
adjuvant treatment of adult patients following resection of GIST. Patients who have a low or very low risk of recurrence should not receive adjuvant treatment.
adult and pediatric patients with newly diagnosed Philadelphia chromosome positive acute lymphoblastic leukaemia (Ph+ ALL) integrated with chemotherapy.
adult patients with relapsed or refractory Ph+ ALL as monotherapy.
adult patients with myelodysplastic/myeloproliferative diseases(MDS/MPD) associated with platelet-derived growth factor receptor (PDGFR) gene re-arrangements.
adult patients with hypereosinophilic syndrome (HES) and/or chronic eosinophilic leukaemia (CEL) with FIP1L1-PDGFRα rearrangement.
adult patients with unresectable, recurrent and/or metastatic dematofibrasarcoma protuberans (DFSP).
adult patients with aggressive systemic mastocytosis (ASM) without the D816V c-Kit mutation or with c-Kit mutational status unknown.
The effectiveness of Imatinib mesylate tablet is based on overall haematological and cytogenetic response rates and progression-free survival in CML, on haematological and cytogenetic response rates in Ph+ ALL, MDS/MPD, on haematological response rates in HES/CEL and ASM and on objective response rates in GIST and DFSP, and on recurrence-free survival in adjuvant GIST. The experience with Imatinib tablet in patients with MDS/MPD associated with PDGFR gene rearrangements is very limited. Except in newly diagnosed chronic phase CML, there are no controlled trials demonstrating a clinical benefit or increased survival in diseases.
Therapy should be initiated by a physician experienced in the treatment of patients with haematological malignancies and malignant sarcomas, as appropriate. For doses of 400 mg and above (see dosage recommendation as follows) a 400 mg tablet (not divisible) is available.
For doses other than 400 mg and 800 mg (see dosage recommendation as follows) a 100 mg divisible tablet is available.
The prescribed dose should be administered orally with a meal and a large glass of water to minimize the risk of gastrointestinal irritations. Doses of 400 mg or 600 mg should be administered once daily, whereas a daily dose of 800 mg should be administered as 400 mg twice a day, in the morning and in the evening.
For patients unable to swallow the tablets, the tablets may be dissolved in a glass of water or apple juice. The required number of tablets should be placed in the appropriate volume of beverage (approximately 50 ml for a 100 mg tablet, and 200 ml for a 400 mg tablet) and stirred with a spoon. The suspension should be administered immediately after complete disintegration of the tablet(s). Treatment should be continued as long as the patient continues to benefit.
Monitoring of response to Imatinib therapy in Ph+ CML patients should be performed routinely and when therapy is modified, to identify suboptimal response, loss of response to therapy, poor patient compliance, or possible drug-drug interaction. Results of monitoring should guide appropriate CML management.
Posology for CML: The recommended dosage of Imatinib Tablets is 400 mg/day for adult patients in chronic phase CML and 600mg/day for patients in accelerated phase or blast crisis.
Dose increases from 400 mg to 600 mg or 800 mg in patients with chronic phase disease, or from 600 mg to a maximum of 800 mg in patients with accelerated phase or blast crisis may be considered in the absence of severe adverse drug reaction and severe non-leukaemia-related neutropenia or thrombocytopenia in the following circumstances: disease progression (at any time); failure to achieve a satisfactory haematological response after at least 3 months of treatment; failure to achieve a cytogenetic response after 12 months of treatment; or loss of a previously achieved haematological and/or cytogenetic response (see Special populations: Paediatric use as follows).
Posology for GIST: The recommended dose of Imatinib Tablets is 400 mg/day for adult patients with unresectable and/or metastatic malignant GIST. A dose increases from 400 mg to 600 mg or 800 mg for patients may be considered in the absence of adverse drug reactions if assessments demonstrate an insufficient response to therapy.
The recommended dose of Imatinib Tablets is 400 mg/day for the adjuvant treatment of adult patients following complete gross resection of GIST. The optimal treatment duration with Imatinib Tablets is not known.
Posology for Ph+ ALL: The recommended dose of Imatinib Tablets is 600 mg/day for adult patients with Ph+ ALL (see Special populations: Paediatric use as follows). Haematological experts in the management of this disease should supervise the therapy throughout all phases of care.
Posology for MDS/MPD: The recommended dose of Imatinib Tablets is 400 mg/day for adult patients with MDS/MPD.
Posology for ASM: The recommended dose of Imatinib Tablets is 400 mg/day for adult patients with ASM without the D816V c-Kit mutation or mutational status unknown or not responding satisfactorily to other therapies.
For patients with ASM associated with eosinophilia, a clonal haematological disease related to the fusion kinase FIP1L1-PDGFR-alpha, a starting dose of 100 mg/day is recommended. A dose increase from 100 mg to 400 mg for these patients may be considered in the absence of adverse drug reactions if assessments demonstrate an insufficient response to therapy.
Posology for HES/CEL: The recommended dose of Imatinib Tablets is 400 mg/day for adult patients with HES/CEL. For HES/CEL patients with demonstrated FIP1L1-PDGFR-alpha fusion kinase, a starting dose of 100 mg/day is recommended. A dose increase from 100 mg to 400 mg for these patients may be considered in the absence of adverse drug reactions if assessments demonstrate an insufficient response to therapy.
Posology for DFSP: The recommended dose of Imatinib Tablets is 800 mg/day for adult patients with DFSP.
Dose adjustment for adverse reactions: Non-haemotological adverse reactions: If a severe non-haematological adverse reaction develops with Imatinib Tablets use, treatment must be withheld until the event has resolved. Thereafter, treatment can be resumed as appropriate depending on the initial severity of the event. If elevations in bilirubin > 3 x institutional upper limit of normal (IULN) or in liver transaminases > 5 x IULN occur, Imatinib Tablets should be withheld until bilirubin levels have returned to < 1.5 x IULN and transaminase levels to <2.5 x IULN. Treatment with Imatinib Tablets may then be continued at a reduced daily dose. In adults the dose should be reduced from 400 to 300 mg or from 600 to 400 mg or from 800 mg to 600 mg, and in children from 340 to 260mg/m
2/day.
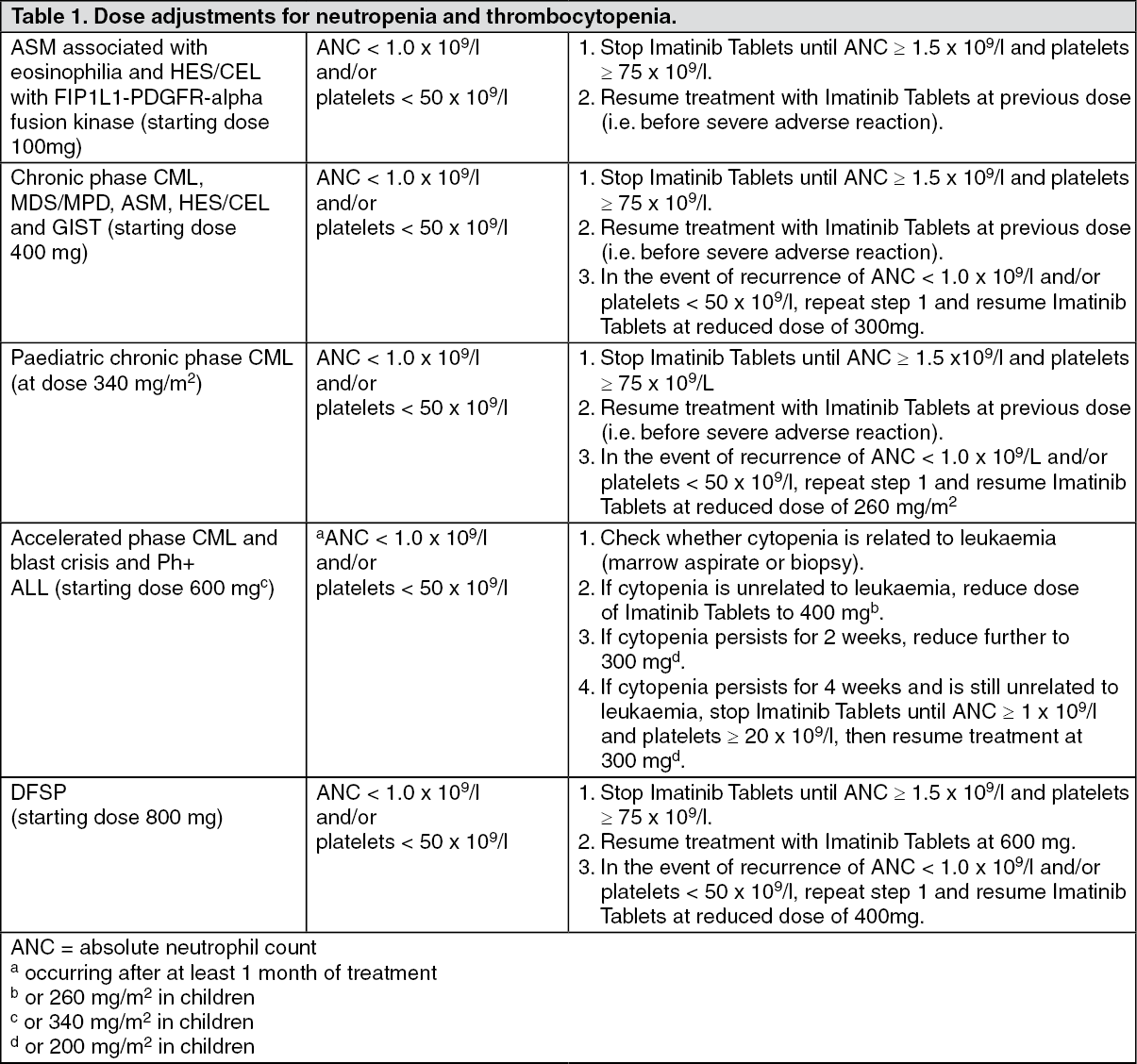
Haematological adverse reactions: Dose reduction or treatment interruption for severe neutropenia and thrombocytopenia are recommended as indicated in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Special populations: Paediatric use:
Click on icon to see table/diagram/image
Special populations: Paediatric use: There is no experience in children with CML below 2 years of age and with Ph+ ALL below 1 year of age. There is very limited to no experience with use of Imatinib Tablets in other indications.
Dosing in children should be on the basis of body surface area (mg/m
2). The dose of 340 mg/m
2 daily is recommended for children with chronic phase and advanced phase CML and Ph+ ALL (not to exceed the total dose of 600 mg daily).
Treatment can be given as a once daily dose in CML and Ph+ ALL. In CML, alternatively the daily dose may be split into two administrations - one in the morning and one in the evening.
Hepatic insufficiency: Imatinib is mainly metabolised by liver. Patients with mild, moderate or severe liver dysfunction should be given the minimum recommended dose of 400 mg daily. The dose can be reduced if not tolerated.
Renal insufficiency: Imatinib and its metabolites are not significantly excreted via the kidney. Patients with renal dysfunction or on dialysis could be given the minimum recommended dose of 400 mg daily as starting dose. However, in these patients caution is recommended. The dose can be reduced if not tolerated. If tolerated, the dose can be increased for lack of efficacy.
Route of Administration: Oral.
Experience with doses higher than the recommended therapeutic dose is limited. Isolated cases of Imatinib Tablets overdose have been reported spontaneously and in the literature. In the event of overdose the patient should be observed and appropriate symptomatic treatment given. Generally the reported outcome in these cases was "improved" or "recovered". Events that have been reported at different dose ranges are as follows: Adult population: 1200 to 1600 mg (duration varying between 1 to 10 days): Nausea, vomiting, diarrhoea, rash, erythema, oedema, swelling, fatigue, muscle spasms, thrombocytopenia, pancytopenia, abdominal pain, headache, decreased appetite.
1800 to 3200 mg (as high as 3200 mg daily for 6 days): Weakness, myalgia, increased creatine phosphokinase, increased bilirubin, gastrointestinal pain.
6400 mg (single dose): One case reported in the literature of one patient who experienced nausea, vomiting, abdominal pain, pyrexia, facial swelling, decreased neutrophil count, increased transaminases.
8 to 10 g (single dose): Vomiting and gastrointestinal pain have been reported.
Paediatric population: One 3-year-old male exposed to a single dose of 400 mg experienced vomiting, diarrhoea and anorexia and another 3-year-old male exposed to a single dose of 980 mg experienced decreased white blood cell count and diarrhoea.
In the event of overdose, the patient should be observed and appropriate supportive treatment given.
Hypersensitivity to the active substance or to any of the excipients (sodium stearyl fumarate, opadry brown).
When Imatinib Tablets is co-administered with other medicinal products, there is a potential for drug interactions. Caution should be used when taking Imatinib Tablets with rifampicin or other strong CYP3A4 inducers, azole antifungals, certain macrolides, CYP3A4 substrates with a narrow therapeutic window (e.g. cyclosporine, pimozide, tacrolimus, sirolimus, ergotamine, diergotamine, fentanyl, alfentanil, terfenadine, bortezomib, docetaxel, quinidine) or warfarin and other coumarin derivatives.
Concomitant use of imatinib and medicinal products that induce CYP3A4 (e.g. dexamethasone, phenytoin, carbamazepine, rifampicin, phenobarbital or Hypericum perforatum, also known as St. John's Wort) may significantly reduce exposure to Imatinib Tablets, potentially increasing the risk of therapeutic failure. Therefore, concomitant use of strong CYP3A4 inducers and imatinib should be avoided.
Hypothyroidism: Hypothyroidism have been reported in thyroidectomy patients undergoing levothyroxine replacement during treatment with Imatinib Tablets. Thyroid-stimulating hormone (TSH) levels should be closely monitored in such patients.
Hepatotoxicity: In patients with hepatic dysfunction (mild, moderate or severe), peripheral blood counts and liver enzymes should be carefully monitored. It should be noted that GIST patients may have hepatic metastases which could lead to hepatic impairment.
Cases of liver injury, including hepatic failure and hepatic necrosis, have been observed with Imatinib. When Imatinib is combined with high dose chemotherapy regimens, an increase in serious hepatic reactions has been detected. Hepatic function should be carefully monitored in circumstances where Imatinib is combined with chemotherapy regimens also known to be associated with hepatic dysfunction.
Fluid retention: Occurrences of severe fluid retention (pleural effusion, oedema, pulmonary oedema, ascites, and superficial oedema) have been reported in approximately 2.5% of newly diagnosed CML patients taking Imatinib Tablets. Therefore, it is highly recommended that patients be weighed regularly. An unexpected rapid weight gain should be carefully investigated and if necessary appropriate supportive care and therapeutic measures should be undertaken. An increased incidence of these events was observed in older people and those with a prior history of cardiac disease. Therefore, caution should be exercised in patients with cardiac dysfunction.
Patients with cardiac disease: Patients with cardiac disease, risk factors for cardiac failure or history of renal failure should be monitored carefully, and any patient with signs or symptoms consistent with cardiac or renal failure should be evaluated and treated. In patients with hypereosinophilic syndrome (HES) with occult infiltration of HES cells within the myocardium, isolated cases of cardiogenic shock/left ventricular dysfunction have been associated with HES cell degranulation upon the initiation of imatinib therapy. The condition was reported to be reversible with the administration of systemic steroids, circulatory support measures and temporarily withholding imatinib. As cardiac adverse events have been reported uncommonly with imatinib, a careful assessment of the benefit/risk of imatinib therapy should be considered in the HES/CEL population before treatment initiation.
Myelodysplastic/myeloproliferative diseases with PDGFR gene re-arrangements could be associated with high eosinophil levels. Evaluation by a cardiology specialist, performance of an echocardiogram and determination of serum troponin should therefore be considered in patients with HES/CEL, and in patients with MDS/MPD associated with high eosinophil levels before imatinib is administered. If either is abnormal, follow-up with a cardiology specialist and the prophylactic use of systemic steroids (1-2 mg/kg) for one to two weeks concomitantly with imatinib should be considered at the initiation of therapy.
Gastrointestinal haemorrhage: In with unresectable and/or metastatic GIST, both gastrointestinal and intra-tumoural haemorrhages were reported. No predisposing factors (e.g. tumour size, tumour location, coagulation disorders) have been identified that place patients with GIST at a higher risk of either type of haemorrhage. Since increased vascularity and propensity for bleeding is a part of the nature and clinical course of GIST, standard practices and procedures for the monitoring and management of haemorrhage in all patients should be applied.
In addition, gastric antral vascular ectasia (GAVE), a rare cause of gastrointestinal haemorrhage, has been reported in post-marketing experience in patients with CML, ALL and other diseases. When needed, discontinuation of Imatinib Tablets treatment may be considered.
Tumour lysis syndrome: Due to the possible occurrence of tumour lysis syndrome (TLS), correction of clinically significant dehydration and treatment of high uric acid levels are recommended prior to initiation of Imatinib Tablets.
Laboratory tests: Complete blood counts must be performed regularly during therapy with Imatinib Tablets. Treatment of CML patients with Imatinib Tablets has been associated with neutropenia or thrombocytopenia. However, the occurrence of these cytopenias is likely to be related to the stage of the disease being treated and they were more frequent in patients with accelerated phase CML or blast crisis as compared to patients with chronic phase CML. Treatment with Imatinib Tablets may be interrupted or the dose may be reduced, as recommended in Dosage & Administration.
Liver function (transaminases, bilirubin, alkaline phosphatase) should be monitored regularly in patients receiving Imatinib Tablets.
In patients with impaired renal function, imatinib plasma exposure seems to be higher than that in patients with normal renal function, probably due to an elevated plasma level of alpha-acid glycoprotein (AGP), an imatinib-binding protein, in these patients. Patients with renal impairment should be given the minimum starting dose. Patients with severe renal impairment should be treated with caution. The dose can be reduced if not tolerated.
Effects on ability to drive and use machines: Patients should be advised that they may experience undesirable effects such as dizziness, blurred vision or somnolence during treatment with imatinib. Therefore, caution should be recommended when driving a car or operating machinery.
Use in Children: There have been case reports of growth retardation occurring in children and pre-adolescents receiving imatinib. The long-term effects of prolonged treatment with imatinib on growth in children are unknown. Therefore, close monitoring of growth in children under imatinib treatment is recommended.
Women of child bearing potential: Women of childbearing potential must be advised to use effective contraception during treatment.
Pregnancy: There are limited data on the use of imatinib in pregnant women. Imatinib Tablets should not be used during pregnancy unless clearly necessary. If it is used during pregnancy, the patient must be informed of the potential risk to the foetus.
Breast-feeding: There is limited information on imatinib distribution on human milk. Both imatinib and its active metabolite were observed to be distributed into human milk. Considering the combined concentration of imatinib and the metabolite and the maximum daily milk intake by infants, the total exposure would be expected to be low (~10% of a therapeutic dose). However, since the effects of low-dose exposure of the infant to imatinib are unknown, women taking imatinib should not breast-feed.
Fertility: Studies on patients receiving Imatinib Tablets and its effect on fertility and gametogenesis have not been performed. Patients concerned about their fertility on Imatinib Tablets treatment should consult with their physician.
Patients with advanced stages of malignancies may have numerous confounding medical conditions that make causality of adverse reactions difficult to assess due to the variety of symptoms related to the underlying disease, its progression, and the co-administration of numerous medicinal products.
More myelosuppression seen in CML patients than in GIST, which is probably due to the underlying disease. Patients with unresectable and/or metastatic GIST, CTC grade ¾ GI bleeds, intra-tumoural bleeds or both were observed. GI tumour sites may have been the source of the GI bleeds. GI and tumoural bleeding may be serious and sometimes fatal. The most commonly reported drug-related adverse reactions in both settings were mild nausea, vomiting, diarrhoea, abdominal pain, fatigue, myalgia, muscle cramps and rash. Superficial oedemas were a common finding and were described primarily as periorbital or lower limb oedemas. However, these oedemas were rarely severe and may be managed with diuretics, other supportive measures, or by reducing the dose of Imatinib Tablets.
When imatinib was combined with high dose chemotherapy in Ph+ ALL patients, transient liver toxicity in the form of transaminase elevation and hyperbilirubinaemia were observed. Considering the limited safety database, the adverse events thus far reported in children are consistent with the known safety profile in adult patients with Ph+ ALL. The safety database for children with Ph+ ALL is very limited though no new safety concerns have been identified. Miscellaneous adverse reactions such as pleural effusion, ascites, pulmonary oedema and rapid weight gain with or without superficial oedema may be collectively described as "fluid retention". These reactions can usually be managed by withholding Imatinib Tablets temporarily and with diuretics and other appropriate supportive care measures. However, some of these reactions may be serious or life-threatening and several patients with blast crisis died with a complex clinical history of pleural effusion, congestive heart failure and renal failure. There were no special safety findings in paediatric.
Adverse reactions: Adverse reactions reported as more than an isolated case are listed as follows, by system organ class and by frequency. Frequency categories are defined using the following convention: very common, common, uncommon, rare, very rare, not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of frequency, the most frequent first. Adverse reactions and their frequencies are reported in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Compatibilities: Active substances that may increase imatinib plasma concentrations: Substances that inhibit the cytochrome P450 isoenzyme CYP3A4 activity (e.g. protease inhibitors such as indinavir, lopinavir/ritonavir, ritonavir, saquinavir, telaprevir, nelfinavir, boceprevir; azole antifungals including ketoconazole, itraconazole, posaconazole, voriconazole; certain macrolides such as erythromycin, clarithromycin and telithromycin) could decrease metabolism and increase imatinib concentrations. There was a significant increase in exposure to imatinib when it was co-administered with a single dose of ketoconazole (a CYP3A4 inhibitor). Caution should be taken when administering Imatinib Tablets with inhibitors of the CYP3A4 family.
Active substances that may decrease imatinib plasma concentrations: Substances that are inducers of CYP3A4 activity (e.g. dexamethasone, phenytoin, carbamazepine, rifampicin, phenobarbital, fosphenytoin, primidone or Hypericum perforatum, also known as St. John's Wort) may significantly reduce exposure to Imatinib Tablets, potentially increasing the risk of therapeutic failure. Concomitant use of rifampicin or other strong CYP3A4 inducers and imatinib should be avoided.
Active substances that may have their plasma concentration altered by Imatinib Tablets: Caution is recommended when administering Imatinib Tablets with CYP3A4 substrates with a narrow therapeutic window (e.g. cyclosporine, pimozide, tacrolimus, sirolimus, ergotamine, diergotamine, fentanyl, alfentanil, terfenadine, bortezomib, docetaxel and quinidine).
Imatinib Tablets may increase plasma concentration of other CYP3A4 metabolised drugs (e.g. triazolobenzodiazepines, dihydropyridine calcium channel blockers, certain HMG-CoA reductase inhibitors, i.e. statins, etc.).
Because of known increased risks of bleeding in conjunction with the use of imatinib (e.g. haemorrhage), patients who require anticoagulation should receive low-molecular-weight or standard heparin, instead of coumarin derivatives such as warfarin.
In vitro Imatinib Tablets inhibits the cytochrome P450 isoenzyme CYP2D6 activity at concentrations similar to those that affect CYP3A4 activity. Dose adjustments do not seem to be necessary when imatinib is co-administrated with CYP2D6 substrates, however caution is advised for CYP2D6 substrates with a narrow therapeutic window such as metoprolol. In patients treated with metoprolol clinical monitoring should be considered.
In vitro, Imatinib Tablets inhibits paracetamol O-glucuronidation. Caution should be exercised when using high doses of Imatinib Tablets and paracetamol concomitantly.
In thyroidectomy patients receiving levothyroxine, the plasma exposure to levothyroxine maybe decreased when Imatinib Tablets is co-administered. Caution is therefore recommended. Drug-drug interactions between imatinib and chemotherapy regimens are not well characterised. Imatinib adverse events, i.e. hepatotoxicity, myelosuppression or others may increase and it has been reported that concomitant use with L-asparaginase could be associated with increased hepatotoxicity. Therefore, the use of Imatinib Tablets in combination requires special precaution.
Store in the original package. Protect from light and moisture. Store below 30°C.
L01EA01 - imatinib ; Belongs to the class of BCR-ABL tyrosine kinase inhibitors. Used in the treatment of cancer.
Trevive FC tab 100 mg
60's
Trevive FC tab 400 mg
30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
