


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Ixekizumab is an IgG4 monoclonal antibody that binds with high affinity (< 3 pM) and specificity to interleukin 17A (both IL‑17A and IL‑17A/F). Elevated concentrations of IL‑17A have been implicated in the pathogenesis of psoriasis by promoting keratinocyte proliferation and activation, as well as in the pathogenesis of psoriatic arthritis. Neutralisation of IL‑17A by ixekizumab inhibits these actions. Ixekizumab does not bind to ligands IL‑17B, IL‑17C, IL‑17D, IL‑17E or IL‑17F.
In vitro binding assays confirmed that ixekizumab does not bind to human Fcγ receptors I, IIa, and IIIa or to complement component C1q.
Pharmacodynamic effects: Ixekizumab modulates biological responses that are induced or regulated by IL‑17A. Based on psoriatic skin biopsy data from a phase I study, there was a dose-related trend towards decreased epidermal thickness, number of proliferating keratinocytes, T cells, and dendritic cells, as well as reductions in local inflammatory markers from baseline to day 43. As a direct consequence treatment with ixekizumab reduces erythema, induration and desquamation present in plaque psoriasis lesions.
Taltz has been shown to lower (within 1 week of treatment) levels of C-reactive protein, which is a marker of inflammation.
Clinical efficacy and safety: Plaque psoriasis: The efficacy and safety of Taltz were assessed in three randomised, double-blind, placebo-controlled phase III studies in adult patients with moderate to severe plaque psoriasis who were candidates for phototherapy or systemic therapy (UNCOVER-1, UNCOVER-2, and UNCOVER-3). The efficacy and safety of Taltz were also evaluated versus etanercept (UNCOVER-2 and UNCOVER-3). Patients randomised to Taltz who were sPGA (0,1) responders (static Physicians Global Assessment) at Week 12 were re-randomised to receive placebo or Taltz for an additional 48 weeks (UNCOVER-1 and UNCOVER-2); patients randomised to placebo, etanercept or Taltz who were sPGA (0,1) non-responders received Taltz for up to 48 weeks.
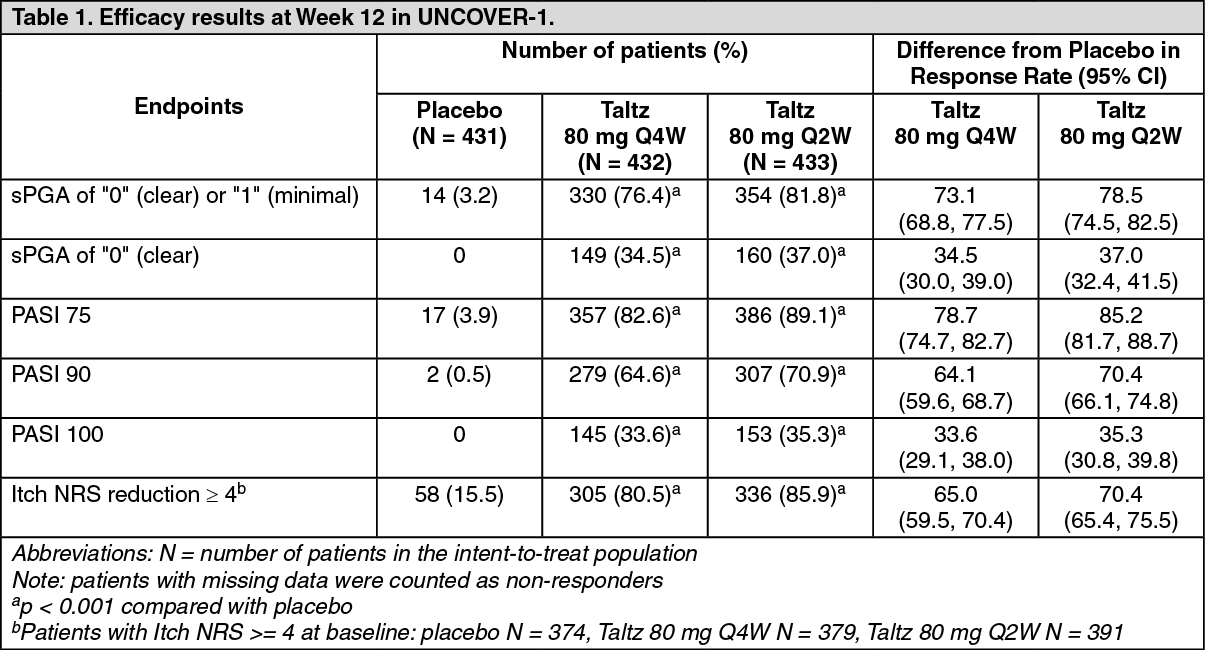
In all three studies, the co-primary endpoints were the proportion of patients who achieved a PASI 75 response (Psoriasis Area and Severity Index) and an sPGA of 0 ("clear") or 1 ("minimal") response at Week 12 versus placebo. Patients in all treatment groups had a median baseline PASI score ranging from 17.4 to 18.3; 48.3 % to 51.2 % of patients had a baseline sPGA score of severe or very severe, and mean baseline itch Numeric Rating Scale (itch NRS) ranging from 6.3 to 7.1.
Clinical response at 12 weeks: UNCOVER-1 enrolled 1,296 patients. Patients were randomised (1:1:1) to receive either placebo or Taltz (80 mg every two or four weeks [Q2W or Q4W] following a 160 mg starting dose) for 12 weeks. (See Table 1.)
 Click on icon to see table/diagram/image
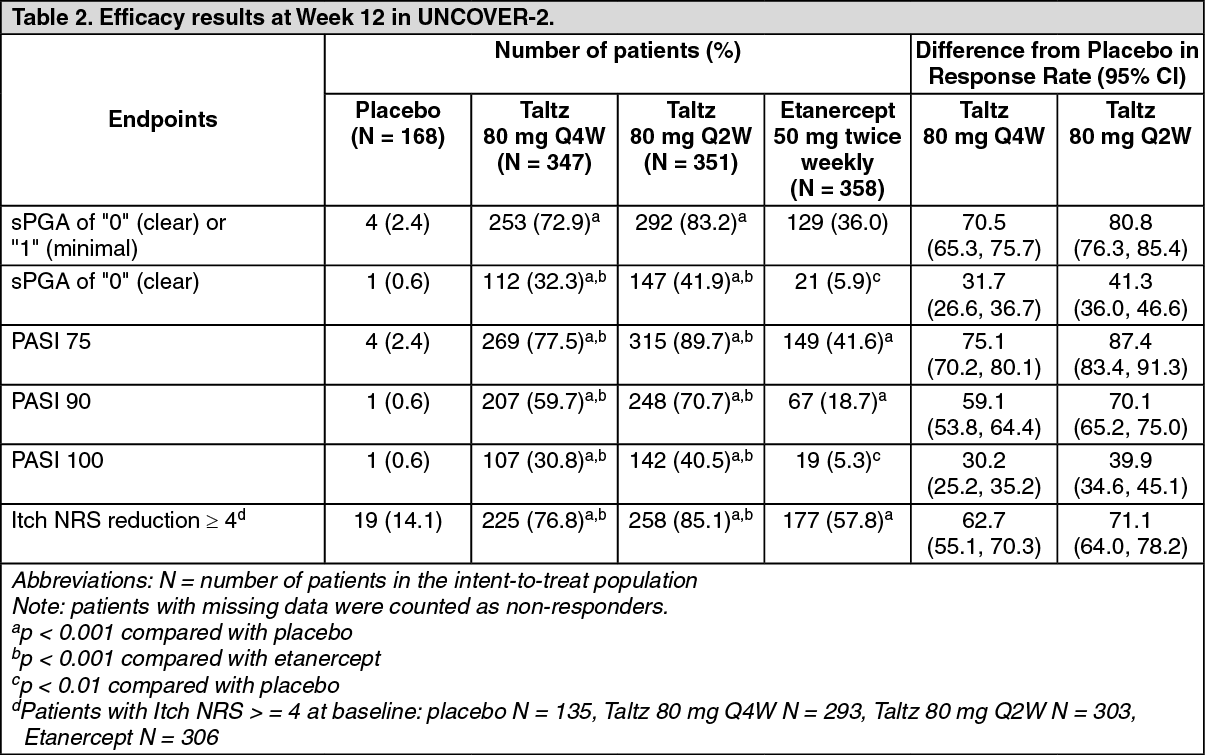
Click on icon to see table/diagram/imageUNCOVER-2 enrolled 1,224 patients. Patients were randomised (1:2:2:2) to receive either placebo, or Taltz (80 mg every two or four weeks [Q2W or Q4W] following a 160 mg starting dose) or etanercept 50 mg twice weekly for 12 weeks. (See Table 2.)
 Click on icon to see table/diagram/image
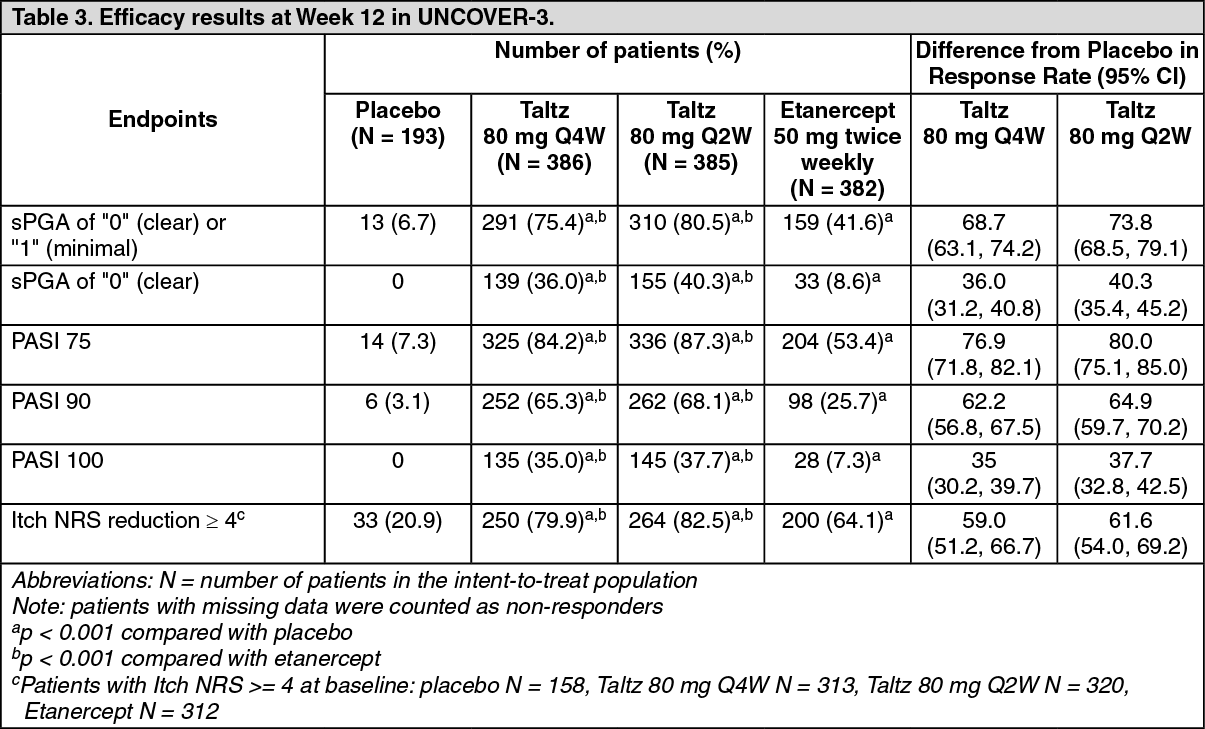
Click on icon to see table/diagram/imageUNCOVER-3 enrolled 1,346 patients. Patients were randomised (1:2:2:2) to receive either placebo, or Taltz (80 mg every two or four weeks [Q2W or Q4W] following a 160 mg starting dose) or etanercept 50 mg twice weekly for 12 weeks. (See Table 3.)
 Click on icon to see table/diagram/image
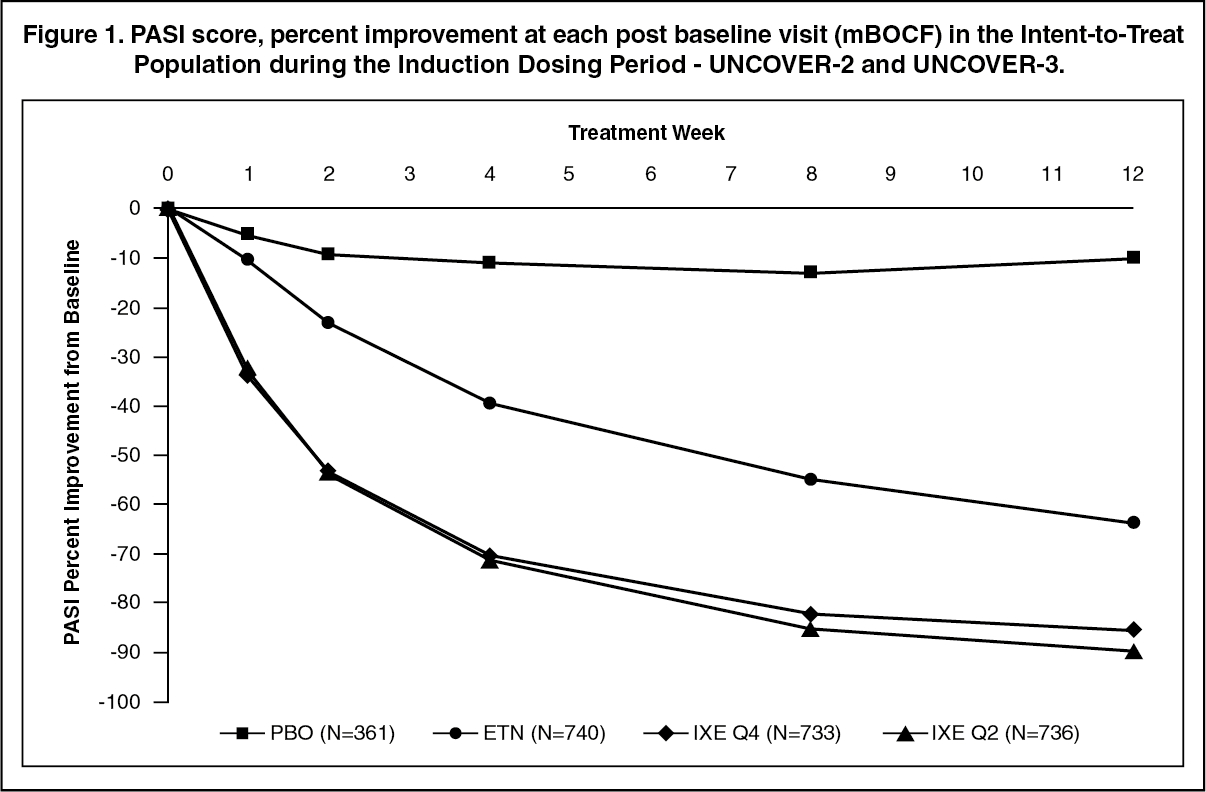
Click on icon to see table/diagram/imageTaltz was associated with a fast onset of efficacy with > 50 % reduction in mean PASI by Week 2 (Figure 1). The percentage of patients achieving PASI 75 was significantly greater for Taltz compared with placebo and etanercept as early as Week 1. Approximately 25 % of patients treated with Taltz achieved a PASI score < 5 by Week 2, more than 55 % achieved the PASI score < 5 by Week 4, and increased to 85 % by Week 12 (compared to 3 %, 14 % and 50 % for etanercept). Significant improvements in itch severity were seen at Week 1 in patients treated with Taltz. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe efficacy and safety of Taltz was demonstrated regardless of age, gender, race, body weight, PASI baseline severity, plaques location, concurrent psoriatic arthritis, and previous treatment with a biologic. Taltz was efficacious in systemic treatment-naive, biologic-naive, biologic/anti-TNF- exposed and biologic/anti-TNF-failure patients.
Efficacy in Non-Responders to Etanercept: For patients identified as an sPGA (0,1) non-responder to etanercept at Week 12 in UNCOVER-2 (N = 200) and who were switched to Taltz 80 mg Q4W after a 4 week washout period, 73 % and 83.5 % of patients were able to achieve sPGA (0,1) and PASI 75, respectively, after 12 weeks of being treated with Taltz.
In the 2 clinical studies that included an active comparator (UNCOVER-2 and UNCOVER-3), the rate of serious adverse events was 1.9 % for both etanercept and for Taltz, and the rate of discontinuation due to adverse events was 1.2 % for etanercept and 2.0 % for Taltz. The rate of infections was 21.5 % for etanercept and 26.0 % for Taltz, with the majority of the events mild to moderate in severity. The rate of serious infections was 0.4 % for etanercept and 0.5 % for Taltz.
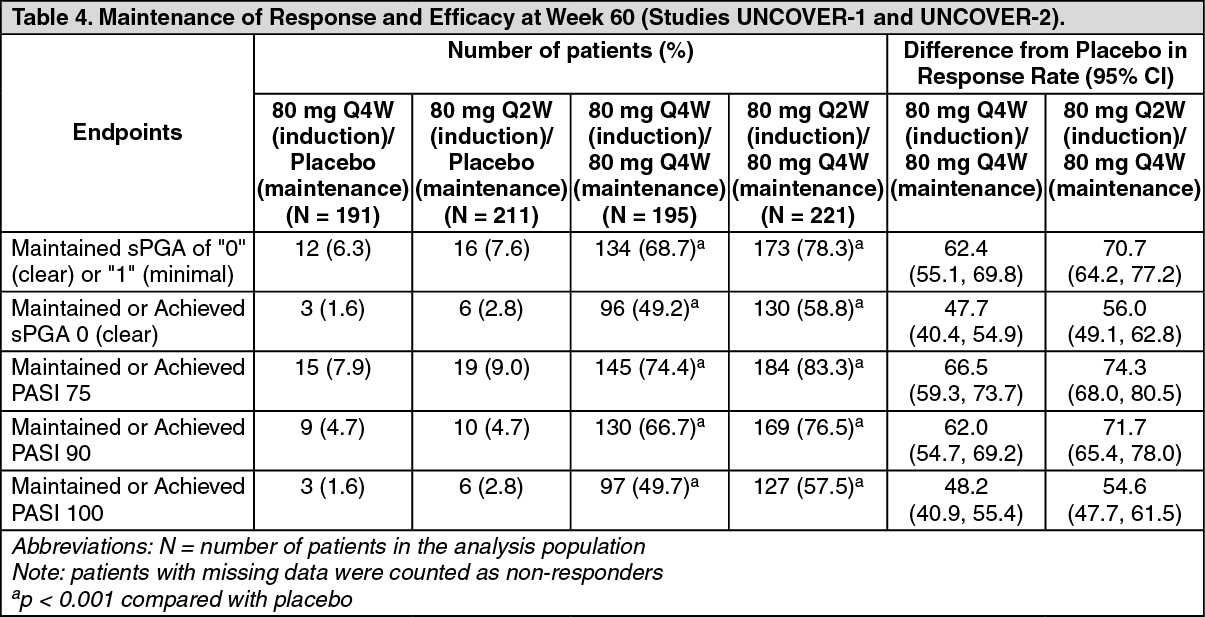
Maintenance of Response at Week 60: Patients originally randomised to Taltz and who were responders at Week 12 (i.e., sPGA score of 0,1) in UNCOVER-1 and UNCOVER-2 were re-randomised to an additional 48 weeks of one of the following treatment regimens: placebo, or Taltz (80 mg every four or twelve weeks [Q4W or Q12W]). (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTaltz was efficacious in the maintenance of response in systemic treatment-naive, biologic-naive, biologic/anti-TNF-exposed and biologic/anti-TNF-failure patients.
For sPGA (0,1) responders at Week 12 re-randomised to treatment withdrawal (i.e., placebo), the median time to relapse (sPGA ≥ 3) was 164 days in integrated UNCOVER-1 and UNCOVER-2 studies. Among these patients, 71.5 % regained at least an sPGA (0,1) response within 12 weeks of restarting treatment with Taltz 80 mg Q4W.
Significantly greater improvements at Week 12 from baseline compared to placebo and etanercept were demonstrated in nail psoriasis (as measured by the Nail Psoriasis Severity Index [NAPSI]), in scalp psoriasis (as measured by Psoriasis Scalp Severity Index [PSSI]) and in palmoplantar psoriasis (as measured by Psoriasis Palmoplantar Severity Index [PPASI]). These improvements in nail, scalp and palmoplantar psoriasis were maintained at Week 60 in patients treated with Taltz who were sPGA (0,1) responders at Week 12.
Quality of Life/Patient-Reported Outcomes: At Week 12 and across studies, Taltz was associated with statistically significant improvement in Health-related Quality of Life as assessed by mean decrease ranges from baseline in the Dermatology Life Quality Index (DLQI) (Taltz 80 mg Q2W from -10.2 to -11.1, Taltz 80 mg Q4W from -9.4 to - 10.7, etanercept from -7.7 to -8.0 and placebo -1.0 to -2.0). A significantly greater proportion of patients treated with Taltz achieved a DLQI 0 or 1. Across studies, Taltz was associated with statistically significant improvement of itching severity assessed by the Itch NRS score. A significantly greater proportion of patients treated with Taltz achieved a reduction of Itch NRS ≥ 4 points at week 12 (84.6% for Taltz Q2W, 79.2% for Taltz Q4W and 16.5% for placebo) and the benefit was sustained over time up to Week 60 in patients treated with Taltz who were sPGA (0 or 1) responders at Week 12. There was not any evidence of worsening of depression up to 60 weeks treatment with Taltz as assessed by the Quick Inventory of Depressive Symptomatology Self Report.
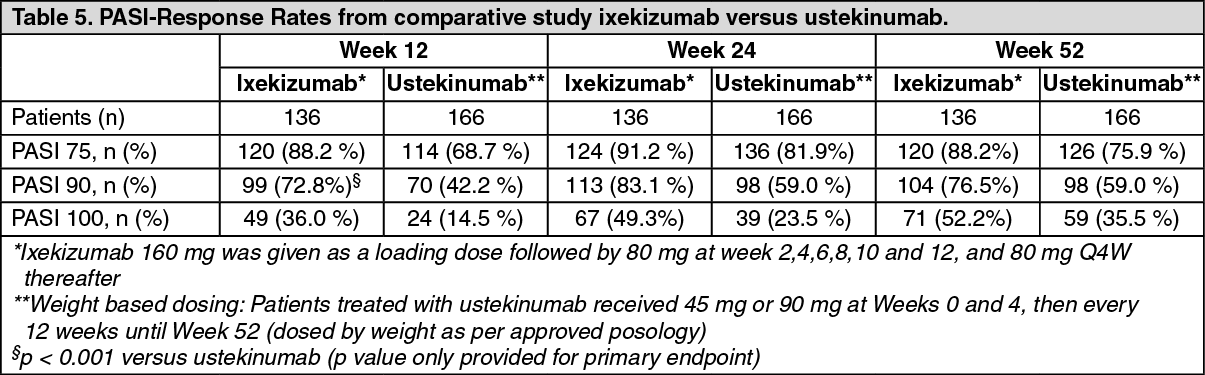
Postmarketing Phase 3b, direct comparative study: Efficacy and safety of ixekizumab was also investigated in a double-blind study compared to ustekinumab with ixekizumab being superior on the primary study objective (PASI 90 response at week 12, Table 5). Onset of response was superior on PASI 75 as early as week 2 (p < 0.001) and on PASI 90 and PASI 100 by week 4 (p < 0.001). Superiority of ixekizumab versus ustekinumab was also demonstrated in the subgroups stratified by weight. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEfficacy in Genital Psoriasis: A randomized, double-blind, placebo-controlled study (IXORA-Q) was conducted in 149 adult subjects (24% females) with moderate to severe genital psoriasis (sPGA of Genitalia score of ≥3), a minimum body surface area (BSA) involvement of 1% (60.4% had a BSA ≥ 10%) and previous failure of or intolerance to at least one topical therapy for genital psoriasis. Patients had at least moderate plaque psoriasis (defined as sPGA score of ≥ 3 and being candidates for phototherapy and/or systemic therapy) for at least 6 months.
Subjects randomized to TALTZ received an initial dose of 160 mg followed by 80 mg every 2 weeks for 12 weeks. The primary endpoint was the proportion of patients who achieved at least a "0" (clear) or "1" (minimal) response on the sPGA of Genitalia (sPGA of Genitalia 0/1). At Week 12, significantly more subjects in the TALTZ group than placebo group achieved a sPGA of Genitalia 0/1 and a sPGA 0/1 independent of baseline BSA (baseline BSA 1% - <10% resp. ≥10%: sPGA of Genitalia "0" or "1": Taltz 71%, resp. 75%; placebo: 0%, resp. 13%). A significantly greater proportion of patients treated with TALTZ achieved a reduction in the PROs of severity of genital pain, genital itch, impact of genital psoriasis on sexual activity, and Dermatology Quality of Life Index (DLQI). (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePsoriatic arthritis: The safety and efficacy of Taltz were assessed in two randomised, double-blind, placebo-controlled phase III studies in 780 patients with active psoriatic arthritis (≥3 swollen and ≥3 tender joints). Patients in these studies had a diagnosis of psoriatic arthritis (Classification Criteria for Psoriatic Arthritis [CASPAR] criteria) for a median of 5.33 years. Randomised patients also had current plaque psoriasis skin lesions (94.0%) or a documented history of plaque psoriasis, with 12.1% of patients with moderate to severe plaque psoriasis at baseline. Over 58.9% and 22.3% of the psoriatic arthritis patients had enthesitis and dactylitis at baseline, respectively. For both studies, the primary endpoint was American College of Rheumatology (ACR) 20 response at Week 24.
In Psoriatic Arthritis Study 1 (SPIRIT-P1), patients naive to biologic therapy with active psoriatic arthritis were randomised to subcutaneous injections of placebo, adalimumab 40 mg once every 2 weeks (active control reference arm), Taltz 80 mg once every 2 weeks (Q2W), or 80 mg once every 4 weeks (Q4W). Both Taltz regimens included a 160 mg starting dose. 85.3% of patients in this study had received prior treatment with ≥1 cDMARD. 53% of patients had concomitant use of MTX at a mean weekly dose of 15.8 mg. 67% of patients who had concomitant use of MTX had a dose of 15 mg or greater. Patients in all treatment groups with an inadequate response at week 16 received rescue therapy (modification to background therapy). Patients on Taltz Q2W or Q4W remained on their originally assigned dose of Taltz. Patients receiving adalimumab or placebo were re-randomised 1:1 to Taltz Q2W or Q4W at week 16 or 24 based on responder status.
Psoriatic Arthritis Study 2 (SPIRIT-P2) enrolled patients who were previously treated with an anti-TNF agent and discontinued the anti-TNF agent for either lack of efficacy or intolerance (anti-TNF-IR patients). Patients were randomised to subcutaneous injections of placebo, Taltz 80 mg once every 2 weeks (Q2W), or 80 mg once every 4 weeks (Q4W). Both Taltz regimens included a 160 mg starting dose. 56% and 35% of patients were inadequate responders to 1 anti-TNF or 2 anti-TNF, respectively. SPIRIT-P2 evaluated 363 patients, of whom 41% had concomitant use of MTX at a mean weekly dose of 16.1 mg. 73.2% of patients who had concomitant use of MTX had a dose of 15 mg or greater. Patients in all treatment groups with an inadequate response at week 16 received rescue therapy (modification to background therapy). Patients in Taltz Q2W or Q4W remained on their originally assigned dose of Taltz. Patients receiving placebo were re-randomised 1:1 to Taltz Q2W or Q4W at week 16 or 24 based on responder status
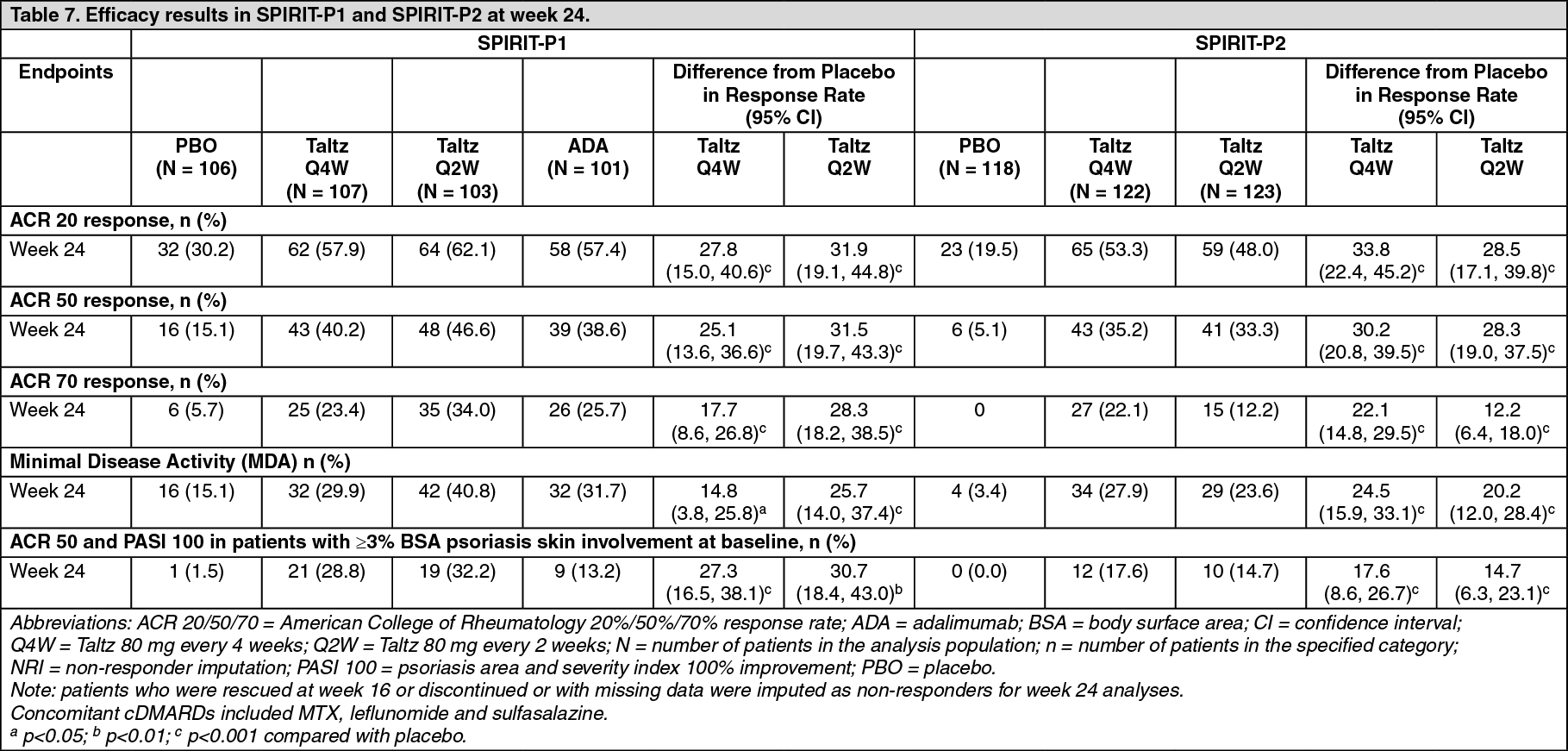
Signs and symptoms: Treatment with Taltz resulted in significant improvement in measures of disease activity compared to placebo at Week 24 (see Table 7).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn patients with pre-existing dactylitis or enthesitis, treatment with Taltz Q4W resulted in improvement in dactylitis and enthesitis at Week 24 compared to placebo (resolution: 78% vs. 24%; p<0.001, and 39% vs. 21%; p<0.01, respectively).
In patients with ≥3% BSA, the improvement in skin clearance at Week 12 as measured by 75% improvement in Psoriasis Area Severity Index (PASI 75), was 67% (94/141) for those treated with the Q4W dosing regimen, and 9% (12/134) for those treated with placebo (p<0.001). The proportion of patients achieving a PASI 75, PASI 90, and PASI 100 response at Week 24 was greater with Taltz Q4W compared to placebo (p<0.001). In patients with concomitant moderate to severe psoriasis and psoriatic arthritis, Taltz Q2W dose regimen showed significantly higher response rate for PASI75, PASI 90 and PASI 100 compared to placebo (p<0.001) and demonstrated clinically meaningful benefit over the Q4W dose regimen.
The treatment responses on Taltz were significantly greater than those on placebo as early as week 1 for ACR 20, week 4 for ACR 50 and week 8 for ACR 70 and persisted through week 24. (See Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn SPIRIT-P1 and SPIRIT-P2, similar responses for ACR 20/50/70 were seen in patients with psoriatic arthritis regardless of whether they were on concomitant cDMARDs, including MTX treatment, or not.
In SPIRIT-P1 and SPIRIT-P2, improvements were shown in all components of the ACR scores including patient assessment of pain. At Week 24 the proportion of patients achieving a modified Psoriatic Arthritis Response Criteria (PsARC) response was greater in the Taltz-treated patients compared to placebo.
In SPIRIT-P1, efficacy was maintained up to Week 52 as assessed by ACR 20/50/70, MDA, enthesitis resolution, dactylitis resolution, and PASI 75/90/100 response rates.
The efficacy and safety of Taltz was demonstrated regardless of age, gender, race, disease duration, baseline body weight, baseline psoriasis involvement, baseline CRP, baseline DAS28-CRP, concomitant corticosteroid use, and previous treatment with a biologic. Taltz was efficacious in biologic-naive, biologic-exposed and biologic-failure patients.
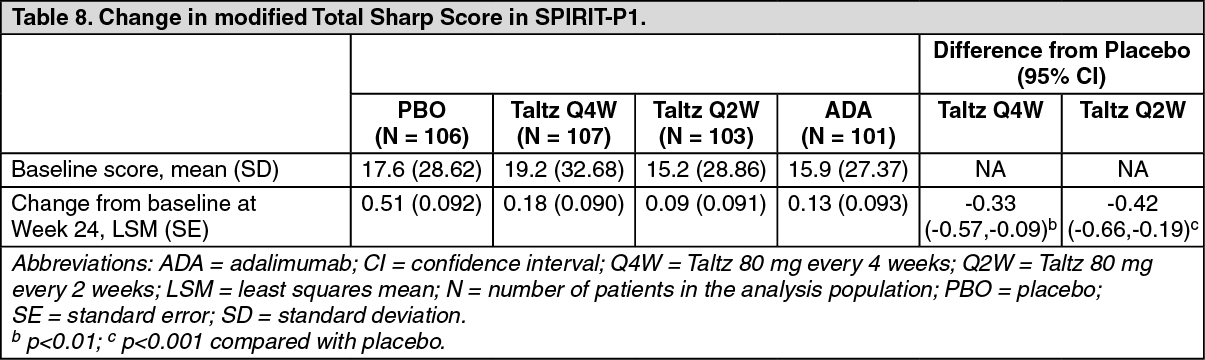
Radiographic response: In SPIRIT-P1, inhibition of progression of structural damage was assessed radiographically and expressed as the change in modified total Sharp Score (mTSS) and its components, the Erosion Score (ES) and the Joint Space Narrowing score (JSN) at Weeks 24 and 52, compared to baseline. Week 24 data are presented in Table 8. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRadiographic joint damage progression was inhibited by Taltz (Table 8) at Week 24, and the percentage of patients with no radiographic joint damage progression (defined as a change from baseline in mTSS of ≤0.5) from randomisation to Week 24 was 94.8% for Taltz Q2W (p<0.001), 89.0% for Taltz Q4W (p=0.026), 95.8% for adalimumab (p<0.001), all compared to 77.4% for placebo. At Week 52, the mean change from baseline in mTSS was 0.27 for placebo/Taltz Q4W, 0.54 for Taltz Q4W/Taltz Q4W, and 0.32 for adalimumab/Taltz Q4W. The percentage of patients with no radiographic joint damage progression from randomisation to Week 52 was 90.9% for placebo/Taltz Q4W, 85.6% for Taltz Q4W/Taltz Q4W, and 89.4% for adalimumab/Taltz Q4W.
Physical function and health-related quality of life: In both SPIRIT-P1 and SPIRIT-P2, patients treated with Taltz Q2W (p<0.001) and Q4W (p<0.001) showed significant improvement in physical function compared to patients treated with placebo as assessed by Health Assessment Questionnaire-Disability Index (HAQ-DI) at Week 24, and maintained at Week 52 in SPIRIT-P1.
Taltz-treated patients reported improvements in health-related quality of life as measured by the Physical Component Summary of the Short Form-36 Health Survey (SF-36 PCS) score (p<0.001). There were also improvements demonstrated in fatigue as assessed by Fatigue severity NRS scores (p<0.001).
Immunisations: In a study in healthy subjects, no safety concerns were identified of two inactivated vaccines (tetanus and pneumococcal), received after two doses of ixekizumab (160 mg followed by a second dose of 80 mg two weeks later). However, the data concerning immunisation were insufficient to conclude on an adequate immune response to these vaccines following administration of Taltz.
Pharmacokinetics: Absorption: Following a single subcutaneous dose of ixekizumab in patients with psoriasis, mean peak concentrations were achieved within 4 to 7 days, across a dose range of 5 to 160 mg. The mean (SD) maximum plasma concentration (Cmax) of ixekizumab, after the 160 mg starting dose, was 19.9 (8.15) μg/ml.
After the 160 mg starting dose, steady state was achieved by Week 8 with the 80 mg Q2W dosing regimen. Mean (SD) Cmax,ss, and Ctrough,ss estimates are 21.5 (9.16) μg/ml, and 5.23 (3.19) μg/ml.
After switching from the 80 mg Q2W dosing regimen to the 80 mg Q4W dosing regimen at Week 12, steady state would be achieved after approximately 10 weeks. Mean (SD) Cmax,ss, and Ctrough,ss estimates are 14.6 (6.04) μg/ml, and 1.87 (1.30) μg/ml.
The average bioavailability of ixekizumab after subcutaneous administration was 54 % to 90 % across analyses.
Distribution: From population pharmacokinetic analyses, the mean total volume of distribution at steady state was 7.11 L.
Biotransformation: Ixekizumab is a monoclonal antibody and is expected to be degraded into small peptides and amino acids via catabolic pathways in the same manner as endogenous immunoglobulins.
Elimination: In the population PK analysis, mean serum clearance was 0.0161 L/hr. Clearance is independent of dose. The mean elimination half-life, as estimated from population pharmacokinetic analysis, is 13 days in patients with plaque psoriasis.
Linearity/non-linearity: Exposure (AUC) increased proportionally over a dose range of 5 to 160 mg given as a subcutaneous injection.
Psoriatic arthritis: The pharmacokinetic properties of Taltz observed in psoriatic arthritis patients were similar to those displayed in plaque psoriasis patients. The bioavailability of Taltz in psoriatic arthritis patients was in the range of 61-84% on the basis of the population pharmacokinetic model.
Elderly: Of the 4,204 plaque psoriasis patients exposed to Taltz in clinical studies, a total of 301 were 65 years of age or older and 36 patients were 75 years of age or older. Of the 1,118 psoriatic arthritis patients exposed to Taltz in clinical studies, a total of 122 patients were 65 years of age or older and 6 patients were 75 years of age or older.
Based on population pharmacokinetic analysis with a limited number of elderly patients (n = 94 for age ≥ 65 years and n = 12 for age ≥ 75 years), clearance in elderly patients and patients less than 65 years of age was similar.
Renal or hepatic impairment: Specific clinical pharmacology studies to evaluate the effects of renal impairment and hepatic impairment on the PK of ixekizumab have not been conducted. Renal elimination of intact ixekizumab, an IgG MAb, is expected to be low and of minor importance; similarly, IgG MAbs are mainly eliminated via intracellular catabolism and hepatic impairment is not expected to influence clearance of ixekizumab.
Toxicology: Preclinical safety data: Non-clinical data from cynomolgus monkeys revealed no special hazards for humans based on repeat-dose toxicity studies, safety pharmacology evaluations, and reproductive and developmental toxicity studies.
Ixekizumab administration to cynomolgus monkeys for 39 weeks at subcutaneous doses up to 50 mg/kg weekly produced no organ toxicity or undesirable effects on immune function (e.g. T-cell dependent antibody response and NK cell activity). A weekly subcutaneous dose of 50 mg/kg to monkeys is approximately 19 times the 160 mg starting dose of Taltz and in monkeys results in exposure (AUC) that is at least 61-fold higher than the predicted mean steady-state exposure in humans administered the recommended dose regimen.
Non-clinical studies have not been conducted to evaluate the carcinogenic or mutagenic potential of ixekizumab.
No effects on reproductive organs, menstrual cycles or sperm were observed in sexually mature cynomolgus monkeys that received ixekizumab for 13 weeks at a weekly subcutaneous dose of 50 mg/kg.
In developmental toxicity studies, ixekizumab was shown to cross the placenta and was present in the blood of offspring for up to 6 months of age. A higher incidence of postnatal mortality occurred in the offspring of monkeys given ixekizumab compared to concurrent controls. This was related primarily to early delivery or maternal neglect of offspring, common findings in nonhuman primate studies, and considered clinically irrelevant.