


 Sign Out
Sign Out




Patients with a medical history of ILD, drug-induced ILD, radiation pneumonitis that required steroid treatment, or any evidence of clinically active ILD were excluded from clinical studies. Patients with clinically important abnormalities in rhythm and conduction as measured by resting electrocardiogram (ECG) (e.g. QTc interval greater than 470 msec) were excluded from these studies. Patients were evaluated for LVEF at screening and every 12 weeks thereafter.
Tabulated list of adverse reactions: Adverse reactions have been assigned to the frequency categories in Table 8 where possible based on the incidence of comparable adverse event reports in a pooled dataset from the 1479 EGFR mutation positive NSCLC patients who received TAGRISSO at a dose of 80 mg daily in the ADAURA, FLAURA, AURA3, AURAex, AURA2 and AURA1 studies.
Adverse reactions are listed according to system organ class (SOC) in MedDRA. Within each system organ class, the adverse drug reactions are ranked by frequency, with the most frequent reactions first. Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. In addition, the corresponding frequency category for each adverse reaction is based on the CIOMS III convention and is defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from available data). (See Table 8.)
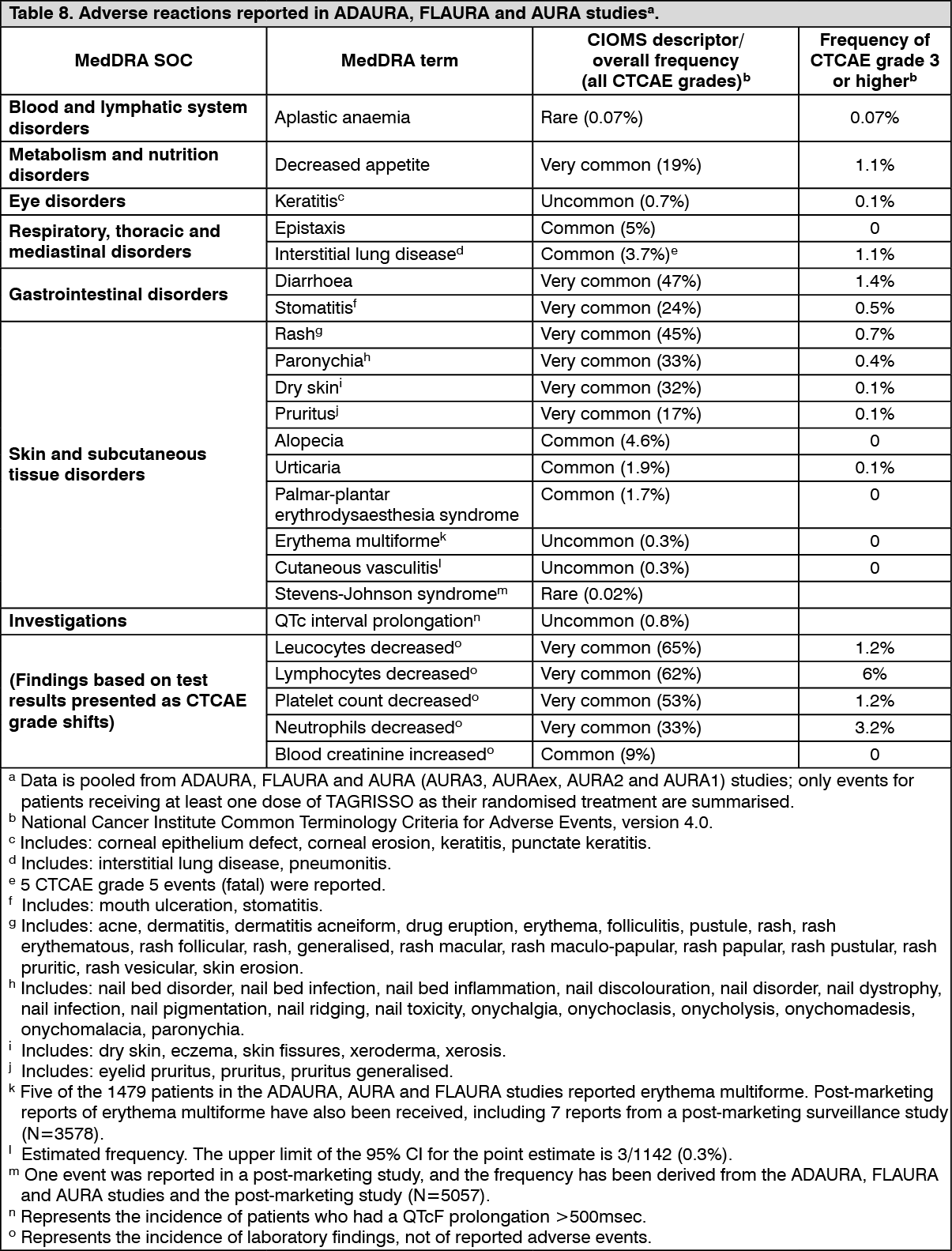 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Interstitial lung disease (ILD): In the ADAURA, FLAURA and AURA studies, the incidence of ILD was 11% in patients of Japanese ethnicity, 1.6% in patients of non-Japanese Asian ethnicity and 2.5% in non-Asian patients. The median time to onset of ILD or ILD-like adverse reactions was 84 days (see Precautions).
QTc interval prolongation: Of the 1479 patients in ADAURA, FLAURA and AURA studies treated with TAGRISSO 80 mg, 0.8% of patients (n=12) were found to have a QTc greater than 500 msec, and 3.1% of patients (n=46) had an increase from baseline QTc greater than 60 msec. A pharmacokinetic/pharmacodynamic analysis with TAGRISSO predicted a concentration-dependent increase in QTc interval prolongation. No QTc-related arrhythmias were reported in the ADAURA, FLAURA or AURA studies (see Precautions and Pharmacology: Pharmacodynamics under Actions).
Gastrointestinal effects: In the ADAURA, FLAURA and AURA studies, diarrhoea was reported in 47% of patients of which 38% were Grade 1 events, 7.9% Grade 2 and 1.4% were Grade 3; no Grade 4 or 5 events were reported. Dose reduction was required in 0.3% of patients and dose interruption in 2%. Four events (0.3%) led to discontinuation. In ADAURA, FLAURA and AURA3 the median time to onset was 22 days, 19 days and 22 days, respectively, and the median duration of the Grade 2 events was 11 days, 19 days and 6 days, respectively.
Haematological events: Early reductions in the median laboratory counts of leukocytes, lymphocytes, neutrophils and platelets have been observed in patients treated with TAGRISSO, which stabilised over time and then remained above the lower limit of normal. Adverse events of leukopenia, lymphopenia, neutropenia and thrombocytopenia have been reported, most of which were mild or moderate in severity and did not lead to dose interruptions. Rare cases of aplastic anaemia, including fatal events, have been reported in association with osimertinib treatment. Osimertinib should be discontinued in patients with confirmed aplastic anaemia (see Dosage & Administration and Precautions).
Special populations: Elderly: In ADAURA, FLAURA and AURA3 (N=1479), 43% of patients were 65 years of age and older, and 12% were 75 years of age and older. Compared with younger subjects (<65), more subjects ≥65 years old had reported adverse reactions that led to study dose modifications (interruptions or reductions) (16% versus 9%). The types of adverse events reported were similar regardless of age. Older patients reported more Grade 3 or higher adverse reactions compared to younger patients (13% versus 8%). No overall differences in efficacy were observed between these subjects and younger subjects. A consistent pattern in safety and efficacy results was observed in the analysis of AURA Phase 2 studies.
Low body weight: Patients receiving TAGRISSO 80 mg with low body weight (<50 kg) reported higher frequencies of Grade ≥3 adverse events (46% versus 31%) and QTc prolongation (12% versus 5%) than patients with higher body weight (≥50 kg).
View ADR Monitoring Form