


 Sign Out
Sign Out


Clinical Studies Experience in Adult Patients with Psoriasis, Psoriatic Arthritis, Crohn's Disease, and Ulcerative Colitis: The safety data described as follows reflect exposure to STELARA in 14 Phase 2 and Phase 3 studies in 6709 patients (4135 with psoriasis and/or psoriatic arthritis, 1749 for Crohn's disease, and 825 with ulcerative colitis), with duration of exposure to STELARA presented in Table 36. (See Table 36.)
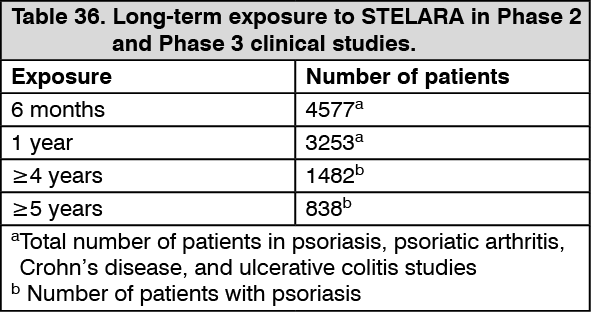 Click on icon to see table/diagram/image
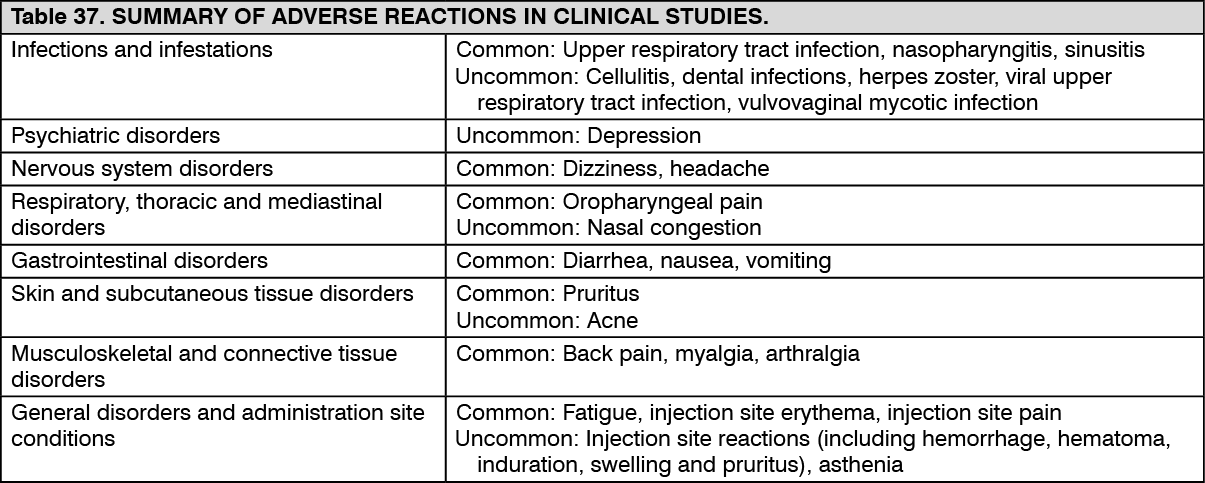
Click on icon to see table/diagram/imageThe most common adverse reactions (> 5%) in controlled periods of the clinical studies with STELARA among all indications were nasopharyngitis and headache. Most were considered to be mild and did not necessitate drug discontinuation. The overall safety profile of STELARA was similar for patients among all indications.
Table 37 provides a summary of Adverse Reactions from the clinical studies. The frequency of these adverse reactions was based on those that occurred during the initial controlled periods of the clinical studies. The adverse reactions are ranked by frequency, using the following convention: Very common (≥ 1/10); Common (frequent) (≥ 1/100, < 1/10); Uncommon (infrequent) (≥ 1/1000, < 1/100); Rare (≥ 1/10000, < 1/1000). (See Table 37.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageInfections: In the placebo-controlled studies of patients with psoriasis, psoriatic arthritis, Crohn's disease, and ulcerative colitis, the rates of infection or serious infection were similar between STELARA-treated patients and those treated with placebo. In the placebo-controlled period of the clinical studies of patients with psoriasis, patients with psoriatic arthritis, patients with Crohn's disease, and patients with ulcerative colitis, the rate of infection was 1.36 and 1.34 per patient-year of follow-up in STELARA and placebo-treated patients, respectively. Serious infections occurred at a rate of 0.03 per patient-year of follow-up in STELARA-treated patients (30 serious infections in 930 patient-years of follow-up) and 0.03 per patient-year of follow-up in placebo-treated patients (15 serious infections in 434 patient-years of follow-up).
In the controlled and non-controlled periods of psoriasis, psoriatic arthritis, Crohn's disease, and ulcerative colitis clinical studies representing 11581 patient-years of exposure in 6709 patients, the median follow-up was 1.0 years; 1.1 years for psoriatic disease studies, 0.6 year for Crohn's disease studies, and 1.0 years for ulcerative colitis studies. The rate of infection was 0.91 per patient-year of follow-up in STELARA-treated patients. The rate of serious infections was 0.02 per patient-year of follow-up in STELARA-treated patients (199 serious infections in 11581 patient-years of follow-up) and included pneumonia, anal abscess, cellulitis, diverticulitis, gastroenteritis and viral infections.
In clinical studies, patients with latent tuberculosis who were concurrently treated with isoniazid did not develop tuberculosis.
Malignancy: In the placebo-controlled period of the psoriasis, psoriatic arthritis, Crohn's disease, and ulcerative colitis clinical studies, the incidence of malignancies excluding non-melanoma skin cancer was 0.11 per 100 patient-years of follow-up for STELARA-treated patients (1 patient in 929 patient-years of follow-up) and 0.23 per 100 patient-years of follow-up for placebo-treated patients (1 patient in 434 patient-years of follow-up). The incidence of non-melanoma skin cancer was 0.43 per 100 patient-years of follow-up for STELARA-treated patients (4 patients in 929 patient-years of follow-up) compared with 0.46 per 100 patient-years of follow-up for placebo-treated patients (2 patients in 433 patient-years of follow-up).
In the controlled and non-controlled periods of psoriasis, psoriatic arthritis, Crohn's disease, and ulcerative colitis clinical studies representing 11561 patient-years of exposure in 6709 patients, the median follow up was 1.0 years; 1.1 years for psoriatic disease studies,0.6 year for Crohn's disease studies, and 1.0 years for ulcerative colitis studies. Malignancies, excluding non-melanoma skin cancers, were reported in 62 patients in 11561 patient-years of follow up (with an incidence of 0.54 per 100 patient-years of follow up for STELARA-treated patients). The incidence of non-melanoma skin cancer was 0.49 per 100 patient-years of follow up for STELARA-treated patients. The incidence of malignancies, reported in STELARA-treated patients was comparable to the incidence expected in the general population (standardized incidence ratio = 0.93 [95% confidence interval: 0.71, 1.20], adjusted for age, gender and race)1. The most frequently observed malignancies, other than non-melanoma skin cancer, were prostate, colorectal, melanoma, and breast. The ratio of patients with basal versus squamous cell skin cancers (3:1) is comparable with the ratio expected in the general population (see Precautions).
1Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER 6.6.2 Regs Research Data, Nov 2009 Sub (1973-2007) - Linked To County Attributes - Total U.S., 1969-2007 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2010, based on the November 2009 submission.
Hypersensitivity and Infusion Reactions: Subcutaneous Administration: During the controlled periods of the psoriasis and psoriatic arthritis clinical studies of STELARA, rash and urticaria have each been observed in <1% of patients.
IV Administration: In Crohn's disease and ulcerative colitis intravenous induction studies, no events of anaphylaxis or other serious infusion reactions were reported. In Crohn's disease studies, 2.4% of 466 placebo treated patients and 2.6% of 470 patients treated with the recommended dose of STELARA reported adverse events occurring during or within an hour of the infusion. In ulcerative colitis studies, 1.9% of 319 placebo patients and 0.9% of 320 patients treated with the recommended dose of STELARA reported adverse events occurring during or within an hour of the infusion.
Immunogenicity: In psoriasis and psoriatic arthritis clinical studies, up to 12.4% of patients treated with STELARA developed antibodies to ustekinumab. Patients positive for antibodies to ustekinumab tended to have lower efficacy, however, antibody positivity did not preclude a clinical response. The majority of patients who were positive for antibodies to ustekinumab had neutralizing antibodies. In Crohn's disease and ulcerative colitis clinical studies, 2.9% and 4.6% of patients, respectively, developed antibodies to ustekinumab when treated with ustekinumab for approximately one year. No apparent association between the development of antibodies to ustekinumab and the development of injection site reactions was observed.
Overdose: Single doses up to 6 mg/kg intravenously have been administered in clinical studies without dose-limiting toxicity. In case of overdosage, it is recommended that the patient be monitored for any signs or symptoms of adverse reactions or effects and appropriate symptomatic treatment be instituted immediately.
Clinical Studies Experience in Pediatric Patients with Psoriasis: The safety of STELARA has been studied in two phase 3 studies of pediatric patients with moderate to severe plaque psoriasis. The first study was in 110 patients from 12 to 17 years of age treated for up to 60 weeks (CADMUS) and the second study was in 44 patients from 6 to 11 years of age treated for up to 56 weeks (CADMUS Jr.). In general, the adverse events reported in these two studies were similar to those seen in previous studies in adults with plaque psoriasis. (see Clinical Studies Experience in Adult Patients with Psoriasis and/or Psoriatic Arthritis previously mentioned).
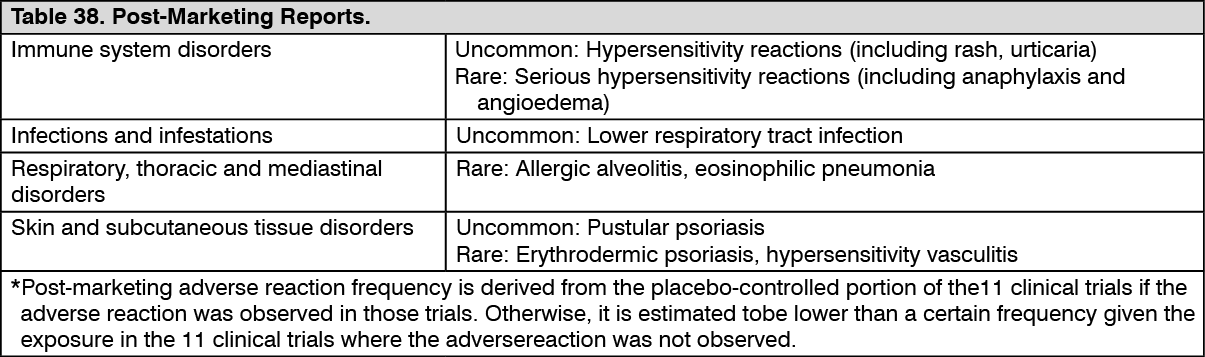
Post Marketing Experience: The adverse reactions in Table 38 are ranked by frequency* using the following convention: Very common: ≥1/10; Common: ≥1/100 and <1/10; Uncommon: ≥1/1000 and <1/100; Rare: ≥1/10000 and <1/1000; Very rare: <1/10000, including isolated reports. (See Table 38.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form