


 Sign Out
Sign Out


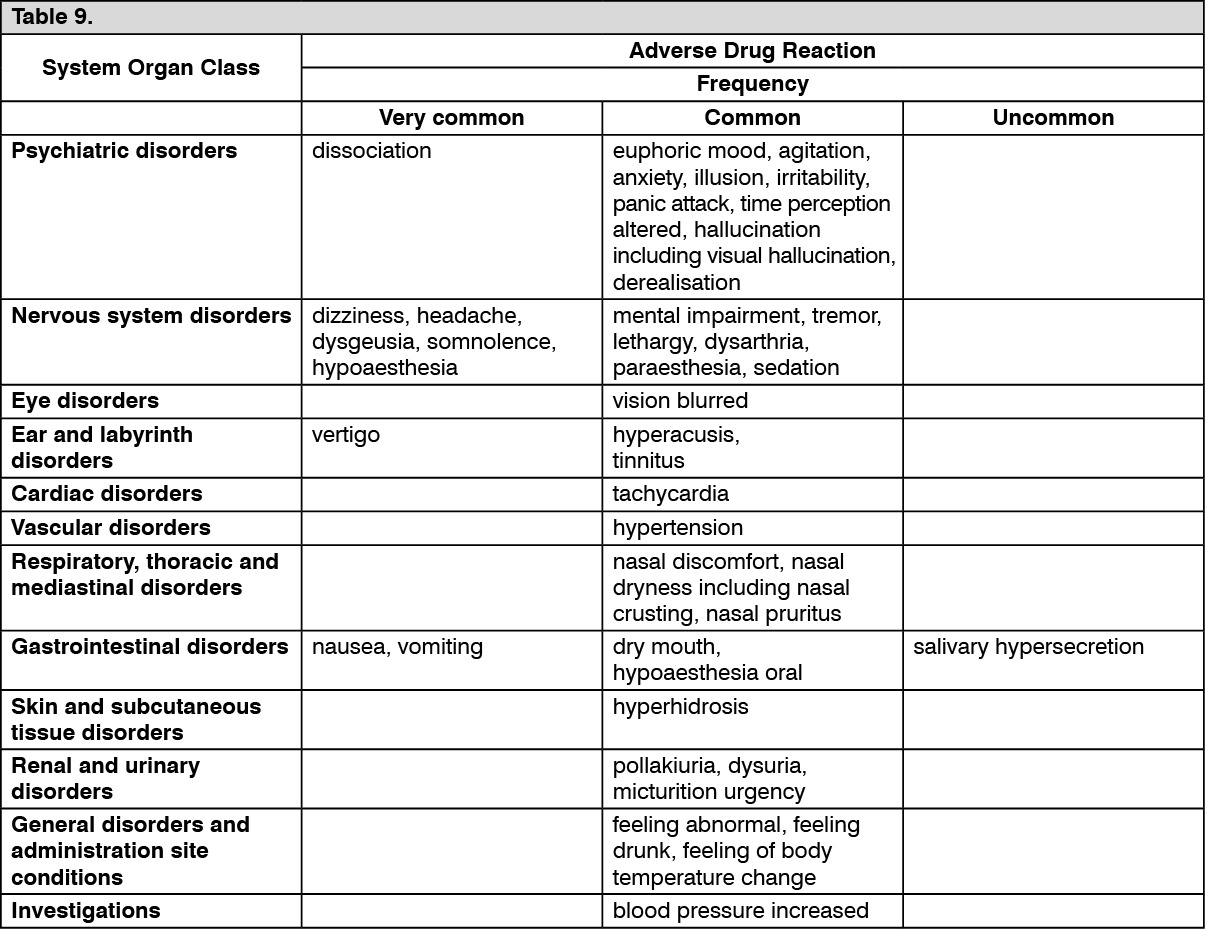
Tabulated list of adverse reactions: Adverse reactions reported with esketamine are listed in the table as follows. Within the designated system organ classes, adverse reactions are listed under headings of frequency, using the following convention: very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000); not known (cannot be estimated from the available data). (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Dissociation: Dissociation (26%) was one of the most common psychological effects of esketamine. Other related terms included derealisation (1.9%), depersonalisation (1.7%), illusions (1.5%), and distortion of time (1.2%). These adverse reactions were reported as transient and self-limited and occurred on the day of dosing. Dissociation was reported as severe in intensity at the incidence of less than 4% across studies. Dissociation symptoms typically resolved by 1.5 hours post-dose and the severity tended to reduce over time with repeated treatments.
Sedation/somnolence: Adverse reactions of sedation (9.1%) and somnolence (18.0%) were primarily mild or moderate in severity, occurred on the day of dosing and resolved spontaneously the same day. Sedative effects typically resolved by 1.5 hours post-dose. Rates of somnolence were relatively stable over time during long-term treatment. In the cases of sedation, no symptoms of respiratory distress were observed, and haemodynamic parameters (including vital signs and oxygen saturation) remained within normal ranges.
Changes in blood pressure: In clinical trials, increases in systolic and diastolic blood pressure (SBP and DBP) over time were about 7 to 9 mmHg in SBP and 4 to 6 mmHg in DBP at 40 minutes post-dose and 2 to 5 mmHg in SBP and 1 to 3 mmHg in DBP at 1.5 hours post-dose in patients receiving SPRAVATO plus oral antidepressants (see Precautions). The frequency of markedly abnormal blood pressure elevations of SBP (≥40 mmHg increase) ranged from 8% (<65 years) to 17% (≥65 years) and DBP (≥25 mmHg increase) ranged from 13% (<65 years) to 14% (≥65 years) in patients receiving esketamine plus oral antidepressant. The incidence of increased SBP (≥ 180 mmHg) was 3% and DBP (≥ 110 mmHg) was 4%.
Cognitive and memory impairment: Cognitive and memory impairment have been reported with long-term ketamine use or drug abuse. These effects did not increase over time and were reversible after discontinuing ketamine. In long-term clinical trials, the effect of esketamine nasal spray on cognitive functioning was evaluated over time and performance remained stable.
Urinary tract symptoms: Cases of interstitial cystitis have been reported with daily and long-term ketamine use at high doses. In clinical studies with esketamine, there were no cases of interstitial cystitis, however a higher rate of lower urinary tract symptoms was observed (pollakiuria, dysuria, micturition urgency, nocturia, and cystitis) in esketamine-treated patients compared with placebo-treated patients.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
Depressive symptoms in patients with major depressive disorder with acute suicidal ideation or behavior: SPRAVATO was evaluated for safety in 262 adults for the treatment of depressive symptoms in adults with major depressive disorder (MDD) with acute suicidal ideation or behavior (see Pharmacology: Pharmacodynamics under Actions) from two Phase 3 studies (Study 3 and Study 4) and one Phase 2 study. Of all SPRAVATO-treated patients in the completed Phase 3 studies, 184 (81%) received all eight doses over a 4-week treatment period.
Adverse reactions leading to discontinuation of treatment: In short-term studies in adults (pooled Study 3 and Study 4), the proportion of patients who discontinued treatment because of an adverse reaction was 6.2% for patients who received SPRAVATO plus oral AD compared to 3.6% for patients who received placebo nasal spray plus oral AD. Adverse reactions leading to SPRAVATO discontinuation in more than 1 patient were (in order of frequency): dissociation-related events (2.6%), blood pressure increased (0.9%), dizziness-related events (0.9%), nausea (0.9%), and sedation-related events (0.9%).
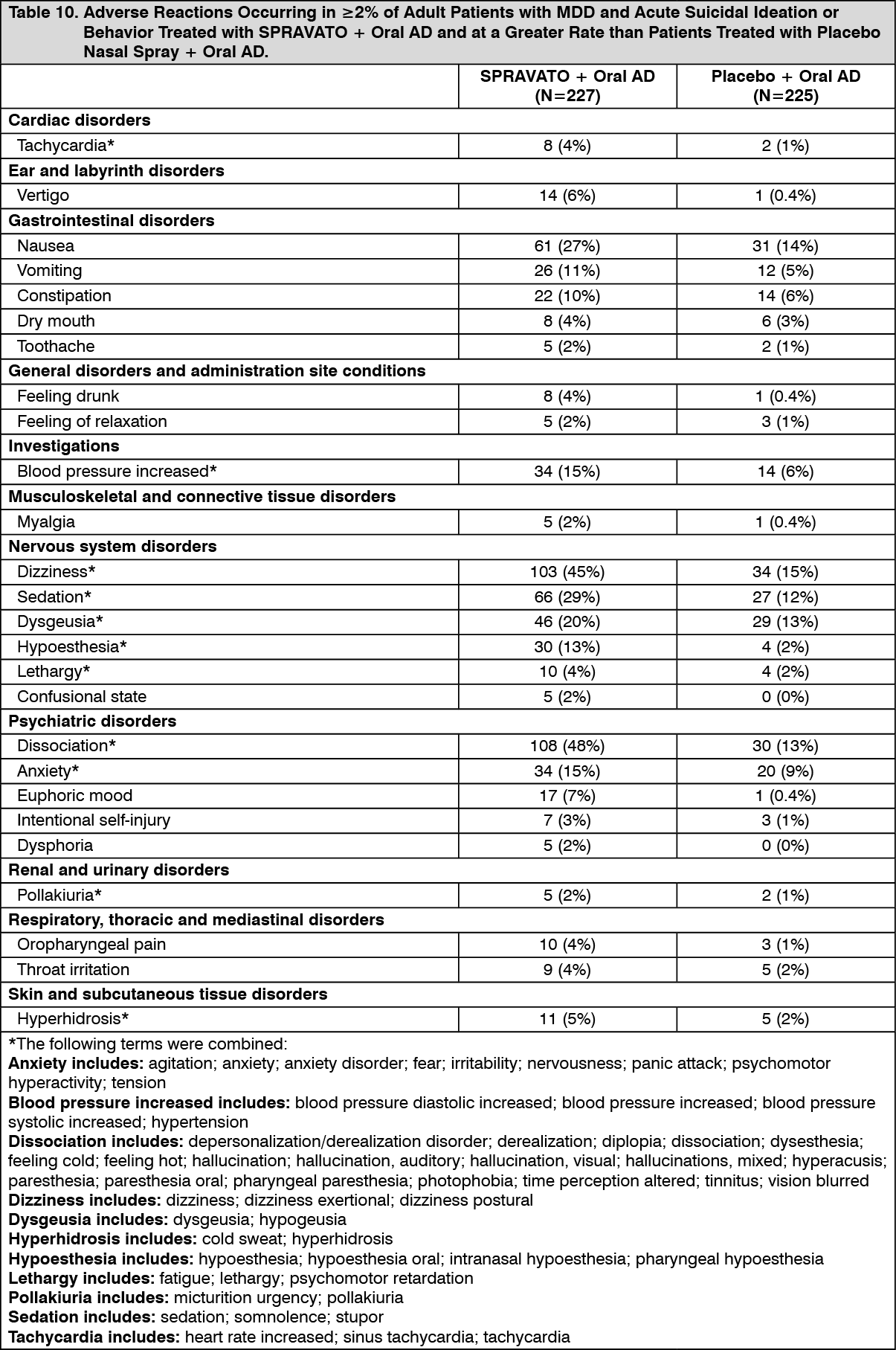
Most common adverse reactions: The most commonly observed adverse reactions in patients treated with SPRAVATO plus oral AD (incidence ≥5% and at least twice that of placebo nasal spray plus oral AD) were dissociation, dizziness, sedation, blood pressure increased, hypoesthesia, vomiting, euphoric mood, and vertigo. Table 10 shows the incidence of adverse reactions that occurred in patients treated with SPRAVATO plus oral AD and greater than patients treated with placebo nasal spray plus oral AD. (See Table 10).
 Click on icon to see table/diagram/image
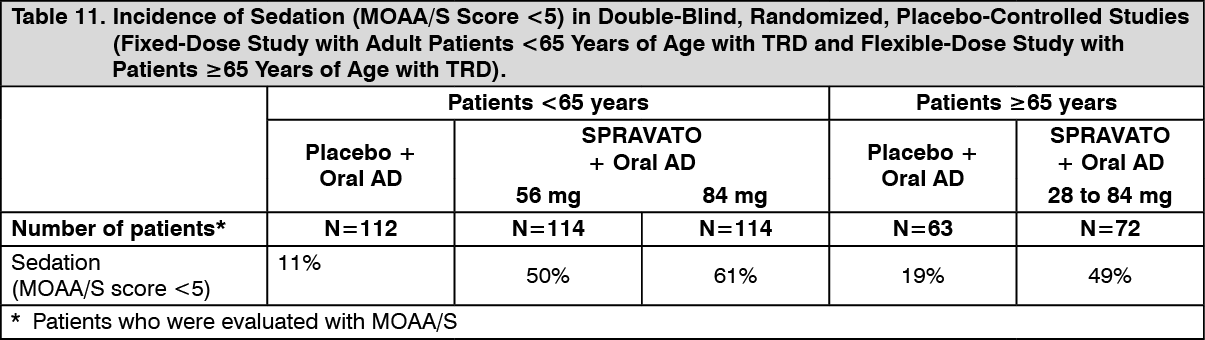
Click on icon to see table/diagram/imageSedation: Sedation was evaluated by adverse event reports and the Modified Observer's Assessment of Alertness/Sedation (MOAA/S). In the MOAA/S, 5 means "responds readily to name spoken in normal tone" and 0 means "no response after painful trapezius squeeze." Any decrease in MOAA/S from pre-dose is considered to indicate the presence of sedation, and such a decrease occurred in a higher number of patients on SPRAVATO than placebo during the short-term TRD studies. Dose-related increases in the incidence of sedation (MOAA/S score <5) were observed in a fixed-dose TRD study [see Precautions]. Table 11 presents the incidence of sedation (MOAA/S score <5) in a fixed-dose study with adult patients <65 years of age with TRD and a flexible-dose study with patients ≥65 years of age with TRD. (See Table 11).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn studies for the treatment of depressive symptoms in adults with MDD with acute suicidal ideation or behavior, there was a higher incidence of sedation (MOAA/S score <5) in patients treated with SPRAVATO plus oral AD compared to patients treated with placebo plus oral AD, similar to the TRD study results in Table 11.
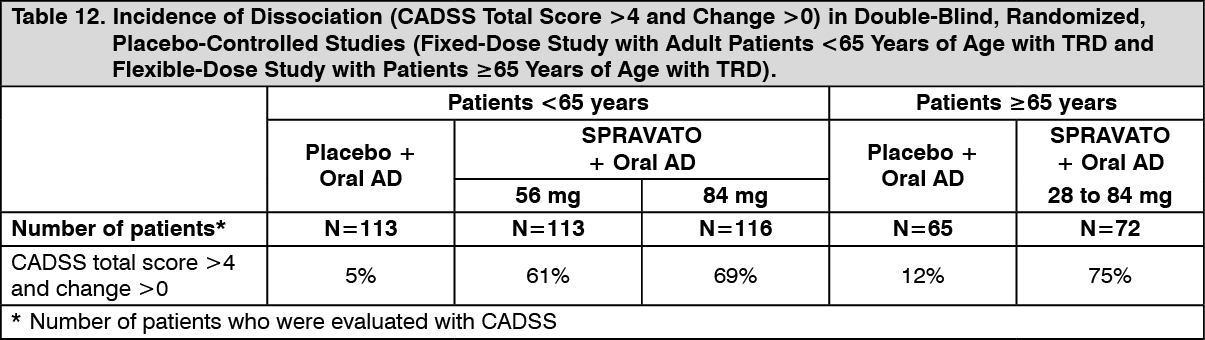
Dissociation/perceptual changes: SPRAVATO can cause dissociative symptoms (including derealization and depersonalization) and perceptual changes (including distortion of time and space, and illusions). In clinical trials, dissociation was transient and occurred on the day of dosing. Dissociation was evaluated by adverse event reports and the Clinician-Administered Dissociative States Scale (CADSS). A CADSS total score of more than 4 indicates the presence of dissociative symptoms, and such an increase to a score of 4 or more occurred in a higher number of patients on SPRAVATO compared to placebo during the short-term TRD studies. Dose-related increases in the incidence of dissociative symptoms (CADSS total score >4 and change >0) were observed in a fixed-dose TRD study [see Precautions]. Table 12 presents the incidence of dissociation (CADSS total score >4 and change >0) in a fixed-dose study with adult patients <65 years of age with TRD and a flexible-dose study with patients ≥65 years of age with TRD. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn studies for the treatment of depressive symptoms in adults with MDD with acute suicidal ideation or behavior, patients treated with SPRAVATO plus oral AD also demonstrated a higher number (84%) with dissociation (CADSS total score >4 and change >0) compared to patients treated with placebo plus oral AD (16%).
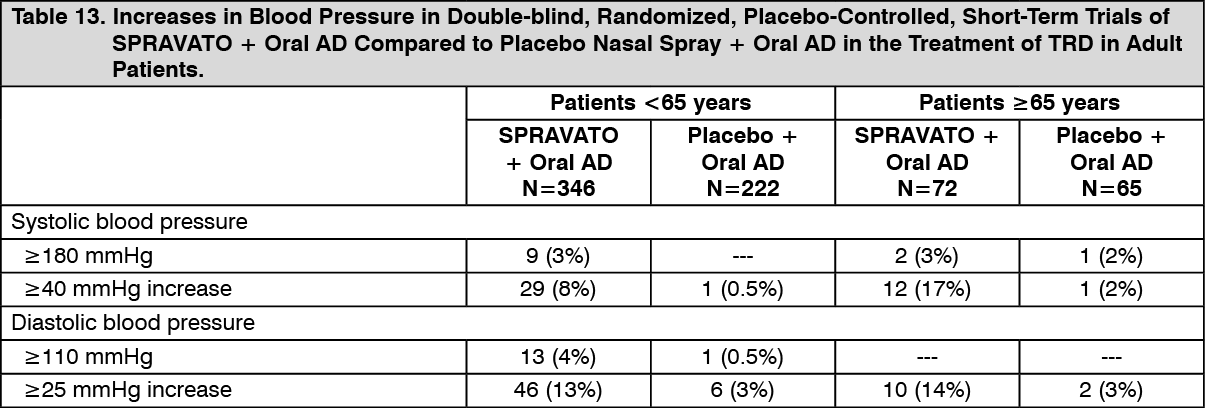
Increase in blood pressure: The mean placebo-adjusted increases in systolic and diastolic blood pressure (SBP and DBP) over time were about 7 to 9 mmHg in SBP and 4 to 6 mmHg in DBP at 40 minutes post-dose and 2 to 5 mmHg in SBP and 1 to 3 mmHg in DBP at 1.5 hours post-dose in patients with TRD receiving SPRAVATO plus oral antidepressants [see Precautions]. Table 13 presents increases in blood pressure in short-term trials with patients <65 years of age and ≥65 years of age with TRD. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn studies for the treatment of depressive symptoms in adults with MDD with acute suicidal ideation or behavior, patients treated with SPRAVATO plus oral antidepressants demonstrated similar mean placebo-adjusted increases in SBP and DBP compared to patient with TRD, as well as similar rates of increases to SBP ≥180 mmHg or ≥40 mmHg increases in SBP, and similar rates of increases to DBP ≥110 mmHg or ≥25 mmHg increases in DBP, compared to the TRD study results in Table 13.
Nausea and vomiting: SPRAVATO can cause nausea and vomiting. Most of these events occurred on the day of dosing and resolved the same day, with the median duration not exceeding 1 hour in most subjects across dosing sessions. Rates of reported nausea and vomiting decreased over time across dosing sessions from the first week of treatment in the short-term studies, as well as over time with long-term treatment. Table 14 presents the incidence and severity of nausea and vomiting in a short-term study with patients with TRD. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn studies for the treatment of depressive symptoms in adults with MDD with acute suicidal ideation or behavior, patients demonstrated similar incidence and severity of reported nausea and vomiting compared to the TRD study results described previously.
Sense of smell: Sense of smell was assessed over time; no difference was observed between patients treated with SPRAVATO plus oral AD and those treated with placebo nasal spray plus oral AD during the double-blind maintenance phase of Study 2 (see Pharmacology: Pharmacodynamics under Actions).
View ADR Monitoring Form