Throughout this section, adverse reactions are presented. Adverse reactions are adverse events that were considered to be reasonably associated with the use of itraconazole based on the comprehensive assessment of the available adverse event information. A causal relationship with itraconazole cannot be reliably established in individual cases. Further, because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Clinical trial data: Capsule: The safety of SPORANOX capsules was evaluated in 8499 patients who participated in 107 open-label and double-blind clinical trials. Of the 8499 patients treated with SPORANOX capsules, 2104 patients were treated with SPORANOX capsules during double-blind trials. All 8499 patients received at least one dose of SPORANOX capsules for the treatment of dermatomycoses or onychomycosis and provided safety data. Adverse reactions reported for ≥1% of patients treated with SPORANOX capsules in these clinical trials are shown in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Adverse reactions that occurred in <1% of patients treated with SPORANOX capsules in these clinical trials are listed in Table 6. (See Table 6.)
Click on icon to see table/diagram/image
The following is a list of additional adverse reactions associated with itraconazole that have been reported in clinical trials of SPORANOX oral solution and/or SPORANOX IV, excluding the adverse reaction term "Injection site inflammation" which is specific to the injection route of administration.
Blood and Lymphatic System Disorders: Granulocytopenia, Thrombocytopenia.
Immune System Disorders: Anaphylactoid reaction.
Metabolism and Nutrition Disorders: Hyperglycemia, Hyperkalemia, Hypokalemia, Hypomagnesemia.
Psychiatric Disorders: Confusional state.
Nervous System Disorders: Neuropathy peripheral, Dizziness, Somnolence.
Cardiac Disorders: Cardiac failure, Left ventricular failure, Tachycardia.
Vascular Disorders: Hypertension, Hypotension.
Respiratory, Thoracic and Mediastinal Disorders: Pulmonary edema, Dysphonia, Cough.
Gastrointestinal Disorders: Gastrointestinal disorder.
Hepatobiliary Disorders: Hepatic failure, Hepatitis, Jaundice.
Skin and Subcutaneous Tissue Disorders: Rash erythematous, Hyperhidrosis.
Musculoskeletal and Connective Tissue Disorders: Myalgia, Arthralgia.
Renal and Urinary Disorders: Renal impairment, Urinary incontinence.
General Disorders and Administration Site Conditions: Generalized edema, Face edema, Chest pain, Pyrexia, Pain, Fatigue, Chills.
Investigations: Alanine aminotransferase increased, Aspartate aminotransferase increased, Blood alkaline phosphatase increased, Blood lactate dehydrogenase increased, Blood urea increased, Gamma-glutamyltransferase increased, Hepatic enzyme increased, Urine analysis abnormal.
Pediatrics: The safety of SPORANOX capsules was evaluated in 165 pediatric patients aged 1 to 17 years who participated in 14 clinical trials (4 double-blind, placebo controlled trials; 9 open-label trials; and 1 trial had an open-label phase followed by a double-blind phase). These patients received at least one dose of SPORANOX capsules for the treatment of fungal infections and provided safety data.
Based on pooled safety data from these clinical trials, the commonly reported adverse reactions in pediatric patients were Headache (3.0%), Vomiting (3.0%), Abdominal pain (2.4%), Diarrhea (2.4%), Hepatic function abnormal (1.2%), Hypotension (1.2%), Nausea (1.2%), and Urticaria (1.2%). In general, the nature of adverse reactions in pediatric patients is similar to that observed in adult subjects, but the incidence is higher in the pediatric patients.
Oral solution: The safety of SPORANOX Oral Solution was evaluated in 889 patients who participated in six double-blind and four open-label clinical trials. Of the 889 patients treated with SPORANOX Oral Solution, 624 patients were treated with SPORANOX Oral Solution during the double-blind trials. All 889 patients received at least one dose of SPORANOX Oral Solution for the treatment of oropharyngeal and esophageal candidiasis and provided safety data. Adverse reactions reported for ≥1% of patients treated with SPORANOX Oral Solution in these clinical trials are shown in Table 7. (See Table 7.)
Click on icon to see table/diagram/image
Adverse reactions that occurred in <1% of patients treated with SPORANOX Oral Solution in these clinical trials are listed in Table 8. (See Table 8.)
Click on icon to see table/diagram/image
The following is a list of additional adverse reactions associated with itraconazole that have been reported in clinical trials of SPORANOX capsules and/or SPORANOX IV, excluding the adverse reaction term "Injection site inflammation" which is specific to the injection route of administration.
Infections and Infestations: Sinusitis, Upper respiratory tract infection, Rhinitis.
Blood and Lymphatic System Disorders: Granulocytopenia.
Immune System Disorders: Anaphylactoid reaction.
Metabolism and Nutrition Disorders: Hyperglycemia, Hyperkalemia, Hypomagnesemia.
Psychiatric Disorders: Confusional state.
Nervous System Disorders: Somnolence.
Cardiac Disorders: Left ventricular failure, Tachycardia.
Vascular Disorders: Hypertension, Hypotension.
Respiratory, Thoracic and Mediastinal Disorders: Pulmonary edema, Dysphonia.
Gastrointestinal Disorders: Gastrointestinal disorder, Flatulence.
Hepatobiliary Disorders: Hepatitis, Jaundice, Hepatic function abnormal.
Skin and Subcutaneous Tissue Disorders: Rash erythematous, Hyperhidrosis.
Renal and Urinary Disorders: Renal impairment, Pollakiuria, Urinary incontinence.
Reproductive System and Breast Disorders: Erectile dysfunction.
General Disorders and Administration Site Conditions: Generalized edema, Face edema, Chest pain, Pain, Fatigue, Chills.
Investigations: Alanine aminotransferase increased, Aspartate aminotransferase increased, Blood alkaline phosphatase increased, Blood lactate dehydrogenase increased, Blood urea increased, Gamma-glutamyltransferase increased, Hepatic enzyme increased, Urine analysis abnormal.
Pediatrics: The safety of SPORANOX Oral Solution was evaluated in 250 pediatric patients aged 6 months to 14 years who participated in five open-label clinical trials. These patients received at least one dose of SPORANOX Oral Solution for prophylaxis of fungal infections or for treatment of oral thrush or systemic fungal infections and provided safety data.
Based on pooled safety data from these clinical trials, the very common reported adverse reactions in pediatric patients were Vomiting (36.0%), Pyrexia (30.8%), Diarrhea (28.4%), Mucosal inflammation (23.2%), Rash (22.8%), Abdominal pain (17.2%), Nausea (15.6%), Hypertension (14.0%), and Cough (11.2%). The nature of adverse reactions in pediatric patients is similar to that observed in adult subjects, but the incidence is higher in the pediatric patients.
Post-marketing data: In addition to the adverse reactions reported during clinical studies and listed previously, the following adverse reactions have been reported during postmarketing experience (Table 9). The frequencies are provided according to the following convention: Very common ≥1/10; Common ≥1/100 and <1/10; Uncommon ≥1/1000 and <1/100; Rare ≥1/10000 and <1/1000; Very rare <1/10000, including isolated reports.
In Table 9, adverse reactions are presented by frequency category based on spontaneous reporting rates. (See Table 9.)
Click on icon to see table/diagram/image



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image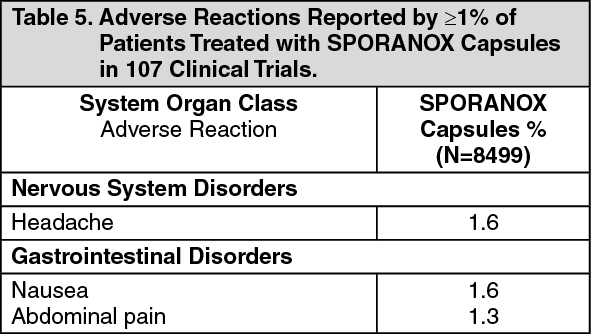 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image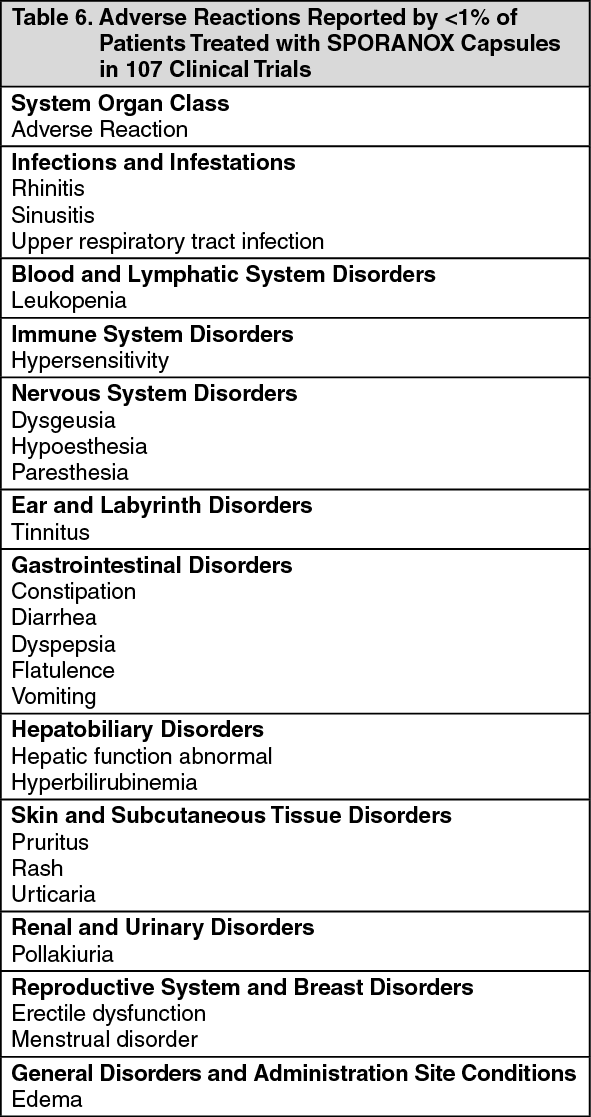 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image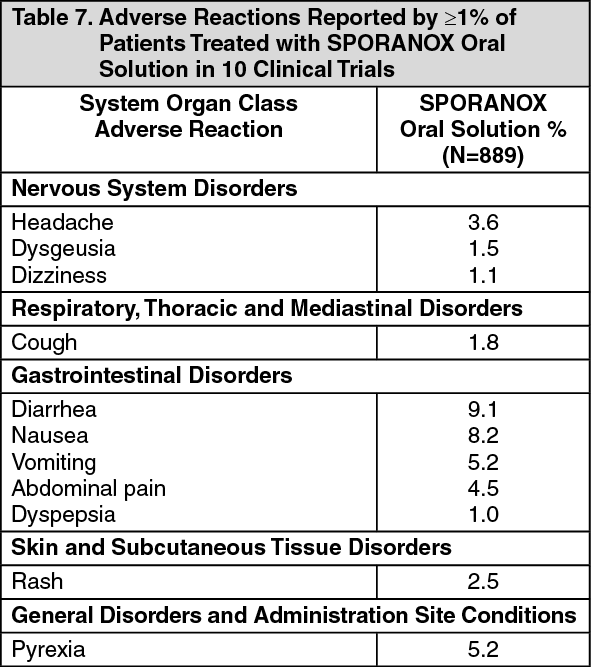 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image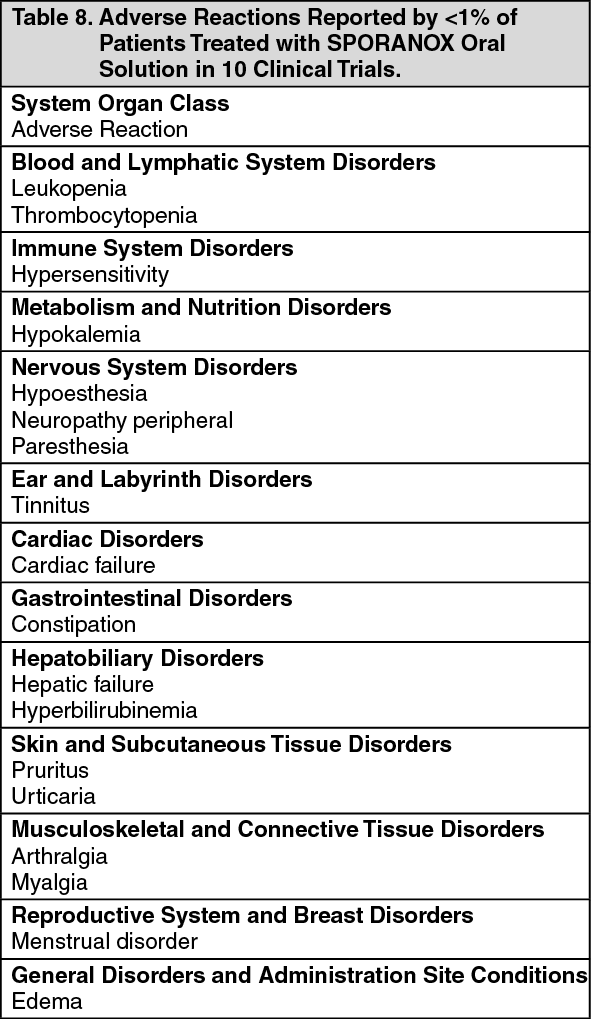 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image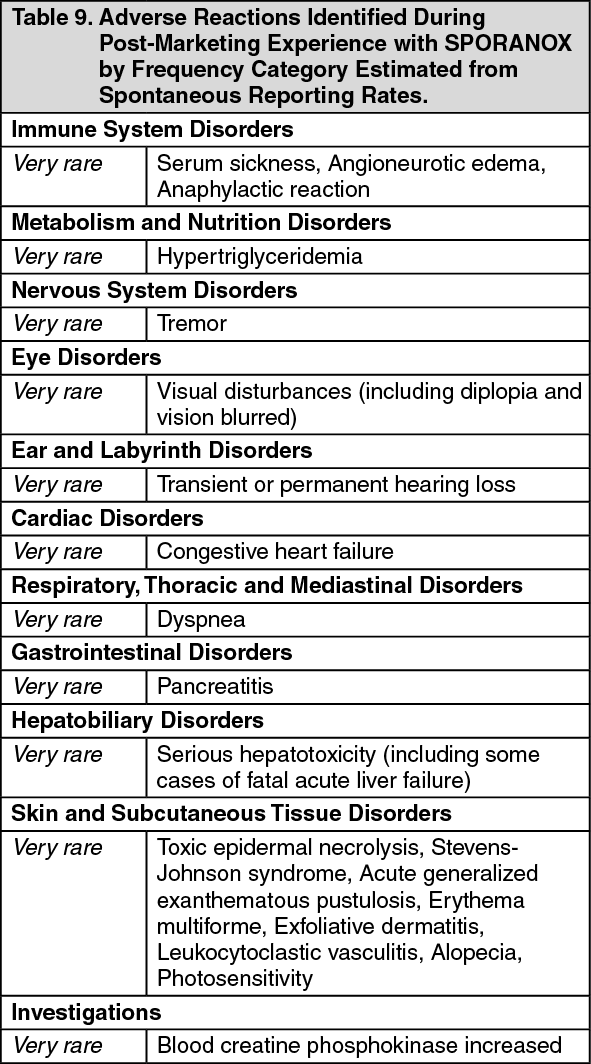 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image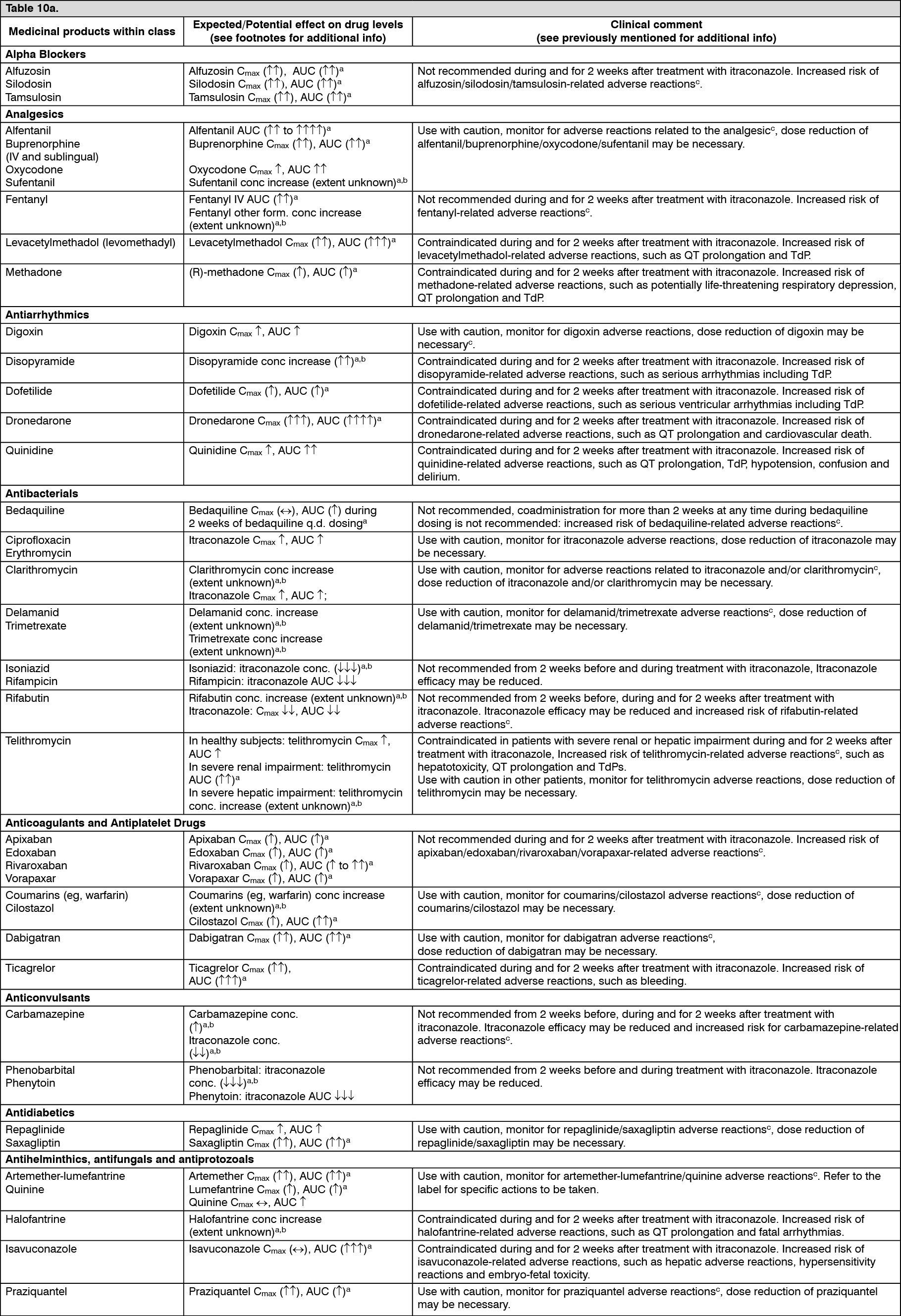 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image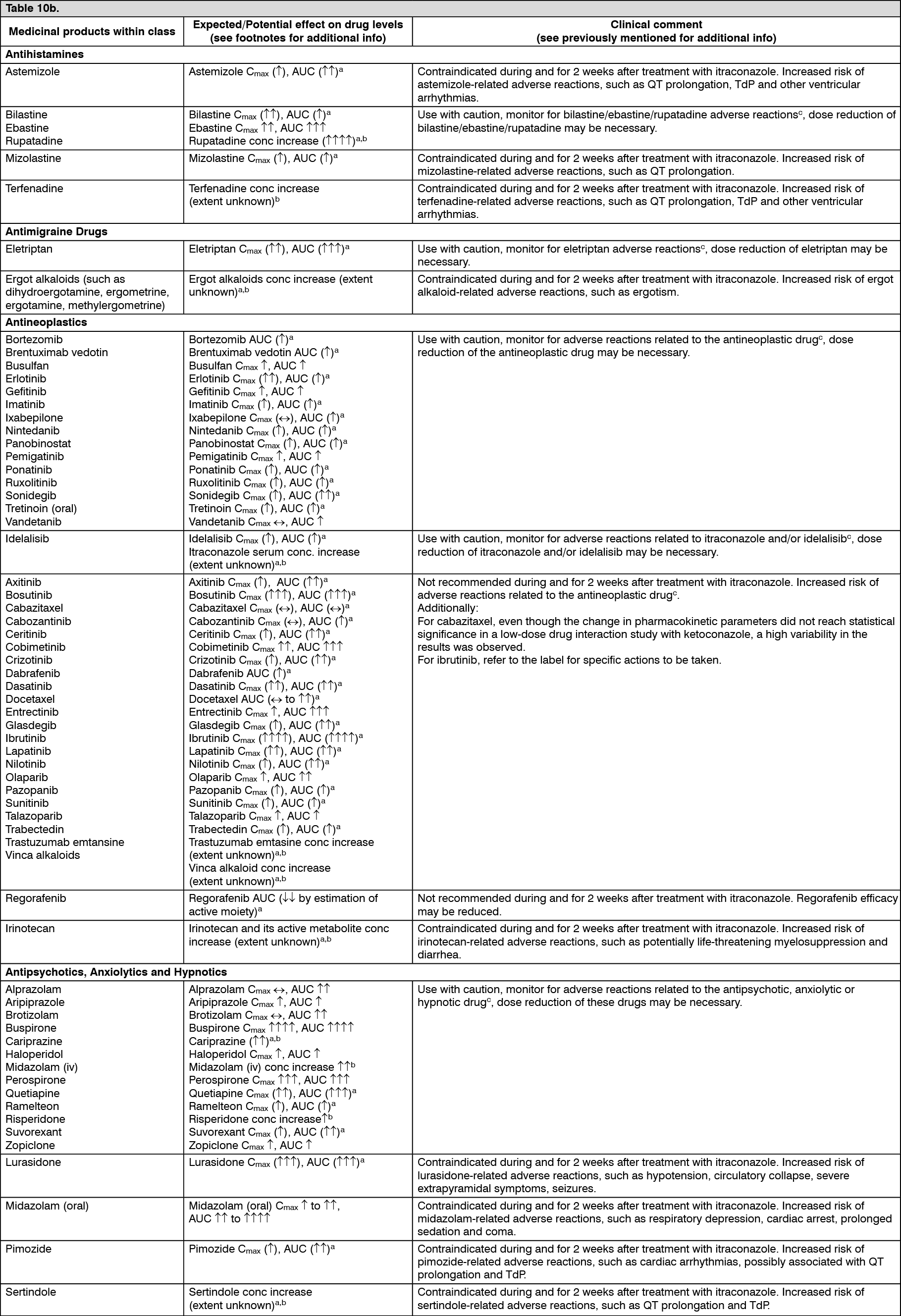 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image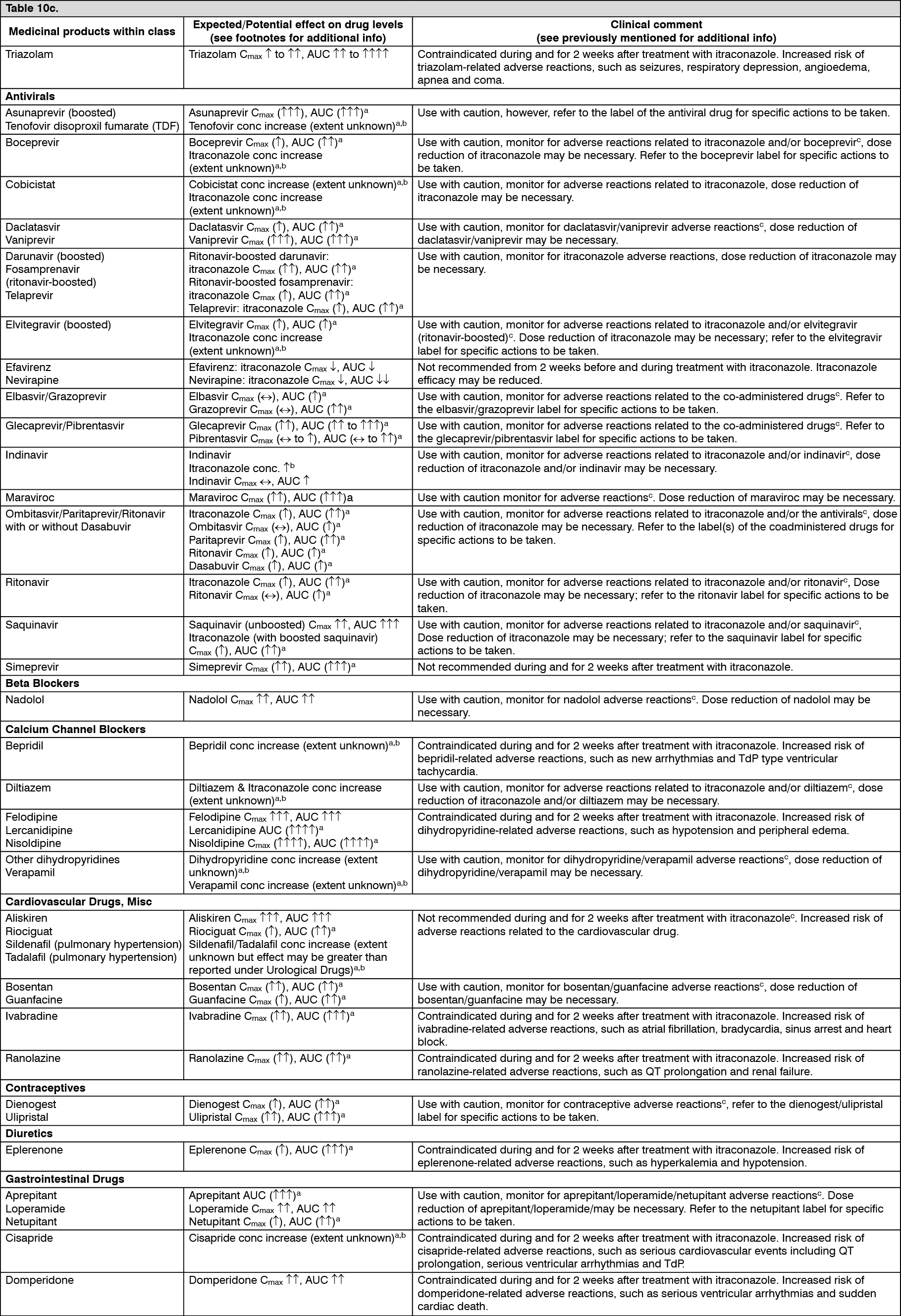 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image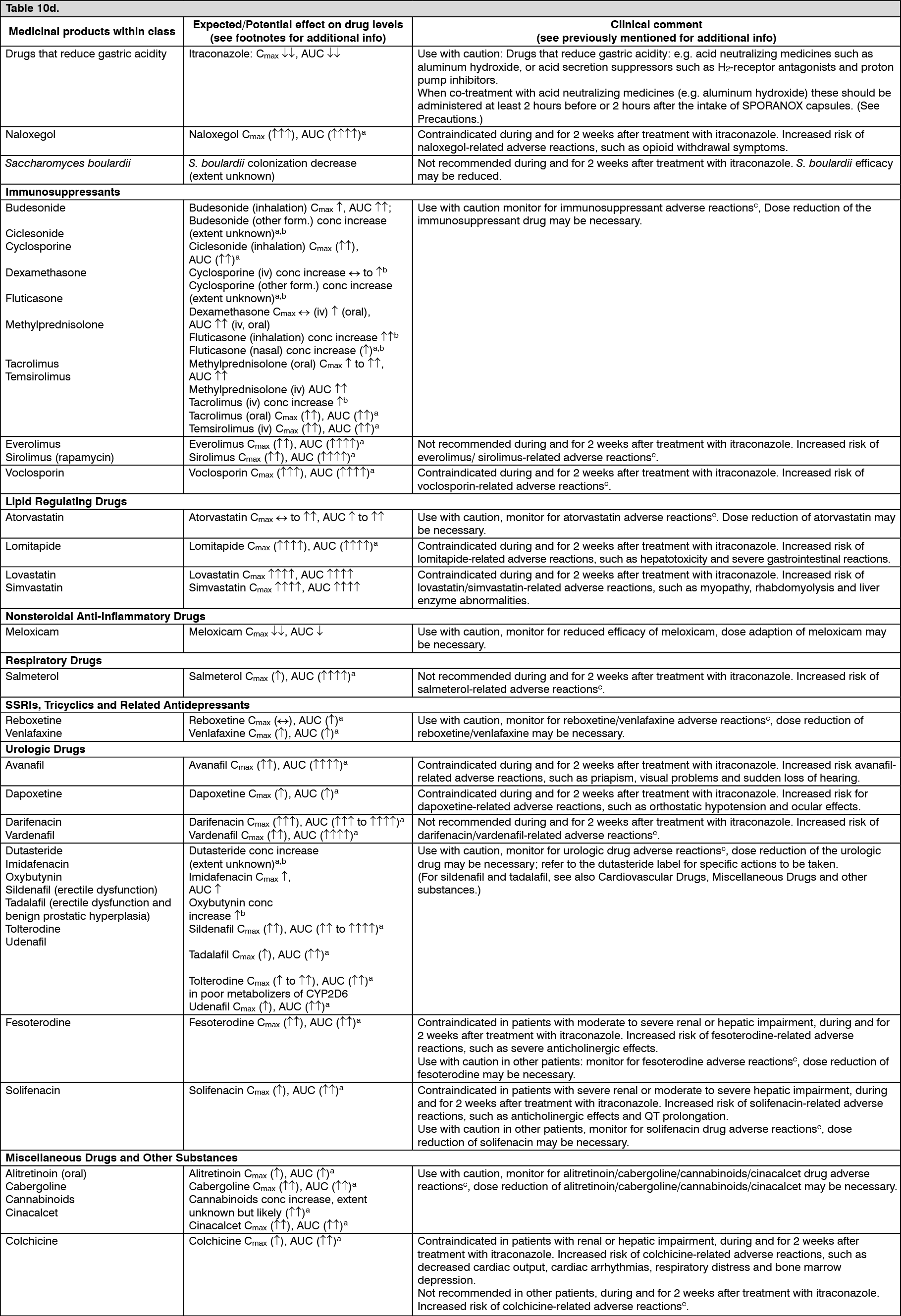 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 10 mg_mL8f5ca157-1ef7-499b-a513-a904008e6a21.GIF)

 Sign Out
Sign Out
