The information highlighted (if any) are the most recent updates for this brand.
Spedra 100 mg tablets: Each tablet contains 100 mg of avanafil.
Spedra 200 mg tablets: Each tablet contains 200 mg of avanafil.
Excipients/Inactive Ingredients: Mannitol, Fumaric acid, Hydroxypropylcellulose, Low substituted Hydroxypropylcellulose, Calcium carbonate, Magnesium stearate, Yellow iron oxide (E172).
Pharmacotherapeutic group: Urologicals; Drugs used in erectile dysfunction. ATC code: G04BE10.
Pharmacology: Pharmacodynamics: Mechanism of action: Avanafil is a highly selective and potent, reversible inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type 5. When sexual stimulation causes the local release of nitric oxide, inhibition of PDE5 by avanafil produces increased levels of cGMP in the corpus cavernosum of the penis. This results in smooth muscle relaxation and inflow of blood into the penile tissues, thereby producing an erection. Avanafil has no effect in the absence of sexual stimulation.
Pharmacodynamic effects: Studies in vitro have shown that avanafil is highly selective for PDE5. Its effect is more potent on PDE5 than on other known phosphodiesterases (> 100-fold for PDE6; > 1,000-fold for PDE4, PDE8 and PDE10; > 5,000-fold for PDE2 and PDE7; > 10,000-fold for PDE1, PDE3, PDE9, and PDE11). Avanafil is > 100-fold more potent for PDE5 than PDE6, which is found in the retina and is responsible for phototransduction. The approximately 20,000-fold selectivity for PDE5 versus PDE3, and enzyme found in heart and blood vessels, is important because PDE3 is involved in control of cardiac contractility.
In a penile plethysmography (RigiScan) study, avanafil 200 mg produced erections considered sufficient for penetration (60% rigidity by RigiScan) in some men as early as 20 minutes after dosing and overall response of these subjects to avanafil was statistically significant, compared to placebo, in the 20-40 minute time interval.
Clinical efficacy and safety: In clinical trials, avanafil was assessed for its effect on the ability of men with erectile dysfunction (ED) to achieve and maintain an erection sufficient for satisfactory sexual activity. Avanafil was evaluated in 4 randomized, double-blind, placebo-controlled, parallel group trials of up to 3 months in duration in the general population with ED, in patients with Type 1 or Type 2 diabetes and ED, and in patients with ED following bilateral nerve-sparing radical prostatectomy. The fourth study investigated the onset of action of avanafil at two doses (100 and 200 mg) in terms of per-subject proportion of sexual attempts resulting in satisfactory completion of sexual intercourse. A total of 1774 patients received avanafil, which was taken as needed at doses of 50 mg (one study), 100 mg and 200 mg (four studies), respectively. Patients were instructed to take 1 dose of study medicinal product approximately 30 minutes prior to initiation of sexual activity. In the fourth study patients were encouraged to attempt sexual intercourse approximately 15 minutes post-dosing, to assess the onset of the erectogenic effect of avanafil, taken on an as needed basis, at 100 and 200 mg dose.
In addition, a subset of patients was enrolled into an open-label extension trial with 493 patients receiving avanafil for at least 6 months and 153 patients for at least 12 months. Patients were initially assigned to avanafil 100 mg and at any point during the trial, they could request to have their dose of avanafil increased to 200 mg or decreased to 50 mg based on their individual response to treatment.
In all trials, statistically significant improvement in all primary efficacy measures were observed for all three doses of avanafil compared to placebo. These differences were maintained with long term treatment (as per studies in the general ED population, in diabetics with ED and in men with ED following bilateral nerve-sparing radical prostatectomy and in the open-label extension trial).
In the general population with ED, the mean percentage of attempts resulting in successful intercourse was approximately 47%, 58%, and 59% for the 50 mg, 100 mg, and 200 mg avanafil groups, respectively, as compared with approximately 28% for placebo.
In men with either Type 1 or Type 2 diabetes mellitus, the mean percentage of attempts resulting in successful intercourse was approximately 34% and 40% for the 100 mg and 200 mg avanafil groups, respectively, compared to approximately 21% for the placebo group.
In men with ED following bilateral nerve-sparing radical prostatectomy, the mean percentage of attempts resulting in successful intercourse was approximately 23% and 26% for the 100 mg and 200 mg avanafil groups, respectively, compared to approximately 9% for placebo.
In the Time to onset study, avanafil demonstrated statistically significant improvement in the primary efficacy variable (average per subject proportion of successful responses by time after dose administration, to the Sexual Encounter Profile 3 - SEP3) as compared with placebo, resulting in successful intercourse in 24.71% of the attempts for the 100 mg dose and 28.18% for the 200 mg dose at approximately 15 minutes after dosing compared to 13.78% for placebo.
Across all of the pivotal trials of avanafil, the percentage of successful intercourse attempts was significantly higher for all doses of avanafil compared to placebo for attempts at all post-dosing time intervals examined.
Pharmacokinetics: Avanafil is rapidly absorbed after oral administration, with a median Tmax of 30 to 45 minutes. Its pharmacokinetics are dose-proportional over the recommended dose range. It is eliminated predominantly by hepatic metabolism (mainly CYP3A4). The concomitant use of potent CYP3A4 inhibitors (e.g. ketoconazole and ritonavir) is associated with increased plasma exposure of avanafil (see Interactions). Avanafil has a terminal half-life of approximately 6-17 hours.
Absorption: Avanafil is rapidly absorbed. Maximum observed plasma concentrations are reached within 0.5 to 0.75 hours of oral dosing in the fasted state. When avanafil is taken with a high fat meal, the rate of absorption is reduced with a mean delay in Tmax of 1.25 hours and a mean reduction in Cmax of 39% (200 mg). There was no effect on the extent ofexposure (AUC). The small changes in avanafil Cmax are considered to be of minimal clinical significance.
Distribution: Avanafil is approximately 99% bound to plasma proteins. Protein binding is independent of total active substance concentrations, age, renal and hepatic function. Avanafil was not found to accumulate in plasma when dosed 200 mg twice daily over 7 days. Based upon measurements of avanafil in semen of healthy volunteers 45-90 minutes after dosing, less than 0.0002% of the administered dose may appear in the semen of patients.
Biotransformation: Avanafil is cleared predominantly by the CYP3A4 (major route) and CYP2C9 (minor route) hepatic microsomal isoenzymes. The plasma concentrations of the major circulating metabolites, M4 and M16, are approximately 23% and 29% that of the parent compound, respectively. The M4 metabolite shows a phosphodiesterase selectivity profile similar to that of avanafil and an in vitro inhibitory potency for PDE5 18% of that of avanafil. Therefore, M4 accounts for approximately 4% of total pharmacologic activity. The M16 metabolite was inactive against PDE5.
Elimination: Avanafil is extensively metabolised in humans. After oral administration, avanafil is excreted as metabolites predominantly in the faeces (approximately 63% of administered oral dose) and to a lesser extent in the urine (approximately 21% of the administered oral dose).
Other special populations: Elderly: Older patients (65 years or over) had comparable exposure to that seen in younger patients (18-45 years). However, data on subjects older than 70 years are limited.
Renal impairment: In subjects with mild (creatinine clearance ≥ 50 - < 80 mL/min) and moderate (creatinine clearance ≥ 30 - < 50 mL/min) renal impairment, the pharmacokinetics of a single 200 mg dose of avanafil were not altered. There are no data available for subjects with severe renal insufficiency or end-stage renal disease on haemodialysis.
Hepatic impairment: Subjects with mild hepatic impairment (Child-Pugh A) had comparable exposure to subjects with normal hepatic function when a single dose of 200 mg avanafil was administered.
The exposure 4 hours post-dose was lower in subjects with moderate hepatic impairment (Child-Pugh B) compared to subject with normal hepatic function after 200 mg of avanafil. The maximum concentration and exposure was similar to that observed after subjects with normal hepatic function received an efficacious avanafil 100 mg dose.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, and toxicity to reproduction.
In a rat fertility and early embryonic development trial, a decrease in fertility and sperm motility, altered estrous cycles, and an increased percentage of abnormal sperm occurred at 1000 mg/kg/day, a dose which also caused parental toxicity in the treated males and females. No effects on fertility or sperm parameters were noted at doses up to 300 mg/kg/day (in male rats 9 times human exposure based on unbound AUC at a dose of 200 mg). There were no treatment-related testicular findings in mice or rats treated with doses up to 600 or 1000 mg/kg/day for 2 years, and no testicular findings in dogs treated with avanafil for 9 months at exposures 110 times human exposure at the Maximum Recommended Human Dose (MRHD).
In pregnant rats, no evidence of teratogenicity, embryotoxicity, or fetotoxicity was observed at doses up to 300 mg/kg/day (approximately 15 times the MRHD on a mg/m2 basis in a 60 kg subject). At a maternally toxic dose of 1000 mg/kg/day (approximately 49 times the MRHD on a mg/m2 basis), decreased fetal body weight occurred with no signs of teratogenicity. In pregnant rabbits, no teratogenicity, embryotoxicity or fetotoxicity was observed at doses up to 240 mg/kg/day (approximately 23 times the MRHD on a mg/m2 basis. In the rabbit study, maternal toxicity was observed at 240 mg/kg/day.
In a rat pre- and postnatal development study, pups exhibited persistent decreases in body weight at 300 mg/kg/day and higher (approximately 15 times the MRHD on a mg/m2 basis) and delayed sexual development at 600 mg/kg/day (approximately 29 times the MRHD on a mg/m2 basis).
Treatment of erectile dysfunction in adult men.
In order for Spedra to be effective, sexual stimulation is required.
Posology: Use in adult men: The recommended dose is 100 mg taken as needed approximately 15 to 30 minutes before sexual activity (see Pharmacology: Pharmacodynamics under Actions). Based on individual efficacy and tolerability, the dose may be increased to a maximum dose of 200 mg or decreased to 50 mg. The maximum recommended dosing frequency is once per day. Sexual stimulation is required for a response to treatment.
Special populations: Elderly (≥ 65 years old): Dose adjustments are not required in elder patients. Limited data are available in elder patients aged 70 years or above.
Renal impairment: Dose adjustments are not required in patients with mild to moderate renal impairment (creatinine clearance ≥ 30 mL/min). Spedra is contraindicated in patients with severe renal impairment (creatinine clearance < 30 mL/min) (see Contraindications and Pharmacology: Pharmacokinetics under Actions). Patients with mild or moderate renal impairment (creatinine clearance ≥ 30 mL/min but < 80 mL/min) who were enrolled in phase 3 studies showed decreased efficacy compared to those with normal renal function.
Hepatic impairment: Spedra is contraindicated in patients with severe hepatic impairment (Child Pugh class C) (see Contraindications and Pharmacology: Pharmacokinetics under Actions). Patients with mild to moderate hepatic impairment (Child-Pugh class A or B) should initiate treatment with the minimum efficacious dose and adjust posology based on tolerance.
Use in men with diabetes: Dose adjustments are not required in diabetic patients.
Paediatric population: There is no relevant use of Spedra in the paediatric population in the indication of erectile dysfunction.
Use in patients using other medicinal products: Concomitant use of CYP3A4 inhibitors: Co-administration of avanafil with potent CYP3A4 inhibitors (including ketoconazole, ritonavir, atazanavir, clarithromycin, indinavir, itraconazole, nefazodone, nelfinavir, saquinavir and telithromycin) is contraindicated (see Contraindications, Precautions and Interactions). In patients receiving concomitant treatment with moderate CYP3A4 inhibitors (including erythromycin, amprenavir, aprepitant, diltiazem, fluconazole, fosamprenavir, and verapamil), the maximum recommended dose of avanafil should not exceed 100 mg, with an interval of at least 48 hours between doses (see Interactions).
Method of administration: For oral use. If Spedra is taken with food, the onset of activity may be delayed compared to the fasted state (see Pharmacology: Pharmacokinetics under Actions).
Single dose of up to 800 mg of avanafil have been given to healthy subjects and multiple daily doses up to 300 mg have been given to patients. Adverse reactions were similar to those seen at lower doses but incidence rates and severities were increased.
In cases of overdose, standard supportive measures should be adopted as required. Renal dialysis is not expected to accelerate clearance as avanafil is highly bound to plasma proteins and it is not eliminated in the urine.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Patients who are using any form of organic nitrate or nitric oxide donors (such as amyl nitrite) (see Interactions).
The co-administration of type 5 phosphodiesterase (PDE5) inhibitors, including avanafil, with guanylate cyclase stimulators, such as riociguat is contraindicated as it may potentially lead to symptomatic hypotension (see Interactions).
Physicians should consider the potential cardiac risk of sexual activity in patients with pre-existing cardiovascular disease before prescribing Spedra.
The use of avanafil is contraindicated in: Patients who have suffered from a myocardial infarction, stroke, or life-threatening arrhythmia within the last 6 months; Patients with resting hypotension (blood pressure < 90/50 mmHg) or hypertension (blood pressure > 170/100 mmHg); Patients with unstable angina, angina with sexual intercourse, or congestive heart failure categorised as New York Heart Association Class 2 or greater.
Patients with severe hepatic impairment (Child-Pugh C).
Patients with severe renal impairment (creatinine clearance < 30 mL/min).
Patients who have loss of vision in one eye because of non-arteritic anterior ischemic optic neuropathy (NAION), regardless of whether this episode was in connection ornot with previous PDE5 inhibitor exposure (see Precautions).
Patients with known hereditary degenerative retinal disorders.
Patients who are using potent CYP3A4 inhibitors (including ketoconazole, ritonavir, atazanavir, clarithromycin, indinavir, itraconazole, nefazodone, nelfinavir, saquinavir and telithromycin) (see Dosage & Administration, Precautions and Interactions).
A medical history and physical examination should be undertaken to diagnose erectile dysfunction and determine potential underlying causes, before pharmacological treatment is considered.
Cardiovascular status: Prior to initiating any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients since there is a degree of cardiac risk associated with sexual activity (see Contraindications). Avanafil has vasodilator properties, resulting in mild and transient decreases in blood pressure (see Interactions), and as such potentiates the hypotensive effect of nitrates (see Contraindications). Patients with left ventricular outflow obstruction, e.g. aortic stenosis and idiopathic hypertrophic subaortic stenosis, can be sensitive to the action of vasodilators, including PDE5 inhibitors.
Priapism: Patients who experience erections lasting 4 hours or more (priapism) should be instructed to seek immediate medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency may result. Avanafil should be used with caution in patients with anatomical deformation of the penis (such as angulation, cavernosal fibrosis, or Peyronie's disease), or in patients who have conditions which may predispose them to priapism (such as sickle cell anaemia, multiple myeloma or leukaemia).
Visual problems: Visual defects and cases of non-arteritic anterior ischaemic optic neuropathy (NAION) have been reported in connection with the intake of other PDE5 inhibitors. The patient should be advised that in case of sudden visual effects, he should stop taking Spedra and consult a physician immediately (see Contraindications).
Effect on bleeding: In vitro studies with human platelets indicate that PDE5 inhibitors do not have an effect on platelet aggregation on their own, but at supratherapeutic doses they potentiate the anti-aggregatory effect of the nitric oxide donor sodium nitroprusside. In humans, PDE5 inhibitors do not appear to affect bleeding time alone or in combination with acetylsalicylic acid.
There is no safety information on the administration of avanafil to patients with bleeding disorders or active peptic ulceration. Therefore, avanafil should be administered to such patients only after careful benefit-risk assessment.
Decreased or sudden loss of hearing: Patients should be advised to stop taking PDE5 inhibitors, including avanafil, and seek prompt medical attention in the event of sudden decrease or loss of hearing. These events, which may be accompanied by tinnitus and dizziness, have been reported in temporal association to the intake of PDE5 inhibitors. It is not possible to determine whether these events are related directly to the use of PDE5 inhibitors or to other factors.
Concomitant use of alpha-blockers: The concomitant use of alpha-blockers and avanafil may lead to symptomatic hypotension in some patients due to additive vasodilatory effects (see Interactions). Consideration should be given to the following: Patients should be stable on alpha-blocker therapy prior to initiating Spedra. Patients who demonstrate haemodynamic instability on alpha-blocker therapy alone are at increased risk of symptomatic hypotension with concomitant use of avanafil.
In those patients who are stable on alpha-blocker therapy, avanafil should be initiated at the lowest dose of 50 mg.
In those patients already taking an optimised dose of Spedra, alpha-blocker therapy should be initiated at the lowest dose. Stepwise increase in alpha-blocker dose may be associated with further lowering of blood pressure when taking avanafil.
The safety of combined use of avanafil and alpha-blockers may be affected by other variables, including intravascular volume depletion and other anti-hypertensive medicinal products.
Concomitant use of CYP3A4 inhibitors: Co-administration of avanafil with potent inhibitors of CYP3A4, such as ketoconazole or ritonavir is contraindicated (see Dosage & Administration, Contraindications and Interactions).
Concomitant use of other treatments for erectile dysfunction: The safety and efficacy of combinations of Spedra andother PDE5 inhibitors or other treatments for erectile dysfunction have not been studied. Patients should be informed not to take Spedra in such combinations.
Concomitant use of alcohol: Consumption of alcohol in combination with avanafil can increase the potential for symptomatic hypotension (see Interactions). Patients should be advised that concurrent use of avanafil and alcohol may increase the likelihood of hypotension, dizziness, or syncope. Physicians should also advise patients on what to do in the event of postural hypotensive symptoms.
Populations not studied: Avanafil has not been evaluated in patients with erectile dysfunction due to spinal cord injury or other neurological disorders and in subjects with severe renal or hepatic impairment.
Effects on ability to drive and use machines: Spedra has minor influence on the ability to drive and use machines. As dizziness and altered vision were reported in clinical trials with avanafil, patients should be aware of how they react to Spedra before driving or using machines.
Pregnancy: Spedra is not indicated for use in women.
There are no data from the use of avanafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition, or postnatal development (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Breast-feeding: There are no data on the use of avanafil during breast-feeding.
Fertility: There was no effect on sperm motility or morphology after single 200 mg oral doses of avanafil in healthy volunteers.
In a clinical trial performed in healthy volunteers and adult males with mild erectile dysfunction, the daily administration of avanafil 100 mg oral doses over a period of 26 weeks was not associated with any untoward effects on sperm concentration, count, motility, or morphology.
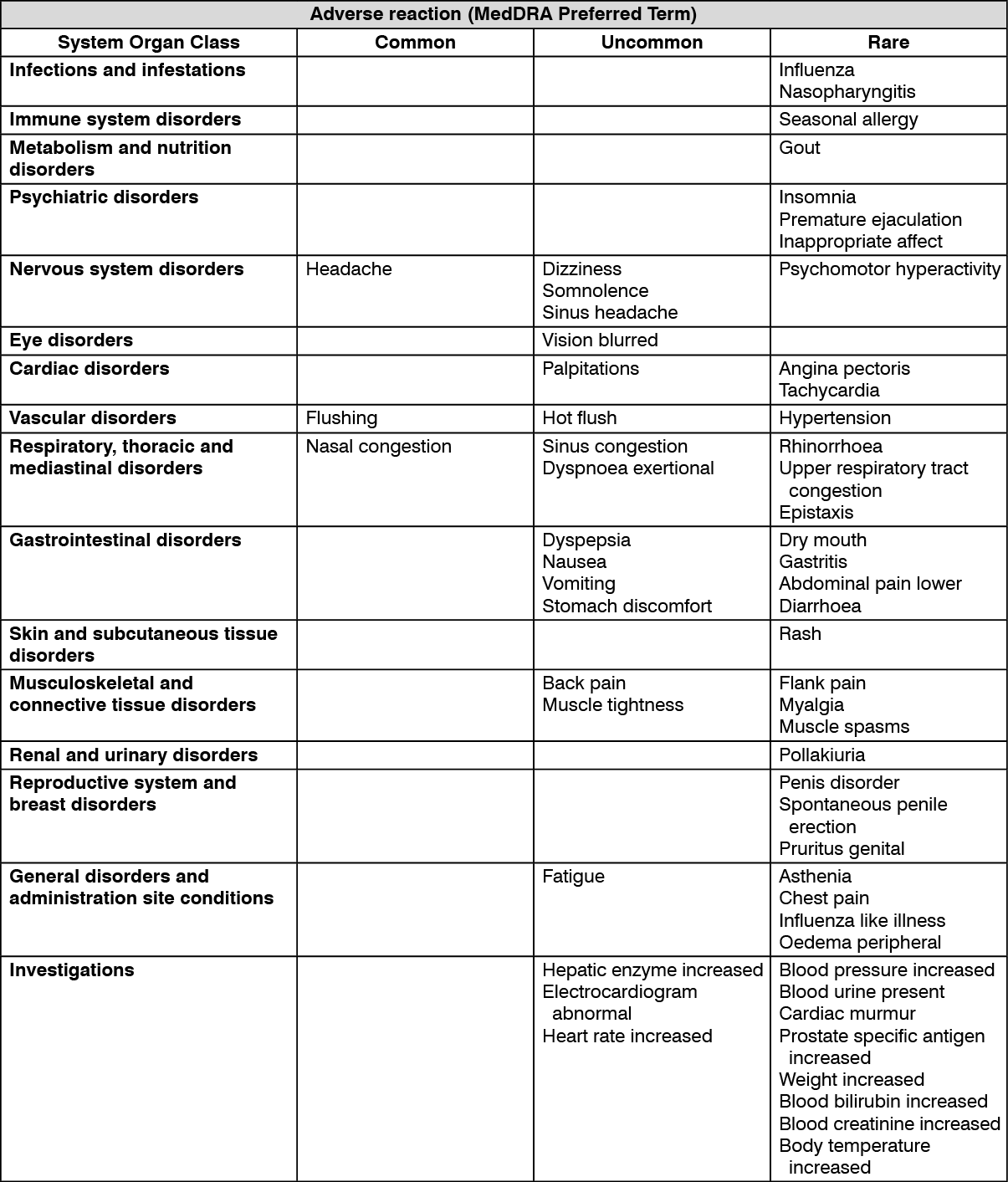
Summary of the safety profile: The safety profile of Spedra is based on 2,566 subjects exposed to avanafil during the clinical development program. The most common adverse reactions reported in clinical studies were headache, flushing, nasal and sinus congestion and back pain. Overall adverse events and adverse reactions for avanafil-treated subjects were more frequent in subjects with a Body Mass Index (BMI) < 25 (normal BMI subjects).
In the long term clinical study, the percentage of patients who experienced adverse reactions decreased with increasing length of exposure.
Tabulated list of adverse reactions: The table as follows lists the adverse reactions observed in placebo-controlled clinical trials according to the MedDRA frequency convention: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000) and not known (cannot be estimated from available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions observed with other PDE5 inhibitors:
Click on icon to see table/diagram/image
Description of selected adverse reactions observed with other PDE5 inhibitors: Non-arteritic anterior ischaemic optic neuropathy (NAION) and sudden loss of hearing have been reported ina small number of post-marketing and clinical trial cases with other PDE5 inhibitors. No cases were reported during clinical trials of avanafil (see Precautions).
Priapism has been reported in a small number of post-marketing and clinical trial cases with other PDE5 inhibitors. No cases were reported during clinical trials of avanafil.
Haematuria, haematospermia and penile haemorrhage has been reported in a small number of post-marketing and clinical trial cases with other PDE5 inhibitors.
Hypotension has been reported post-marketing with other PDE5 inhibitors, and dizziness, a symptom commonly caused by lowered blood pressure, has been reported in clinical trials with avanafil (see Interactions).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
Potential for pharmacodynamic interactions with avanafil: Nitrates: Avanafil was shown to augment the hypotensive effects of nitrates compared to placebo in healthy subjects. This is thought to result from the combined effects of nitrates and avanafil on the nitric oxide/cGMP pathway. Therefore, administration of avanafil to patients who are using any form of organic nitrate or nitric oxide donor (such as amyl nitrite) is contraindicated. In a patient who has taken avanafil within 12 hours, where nitrate administration is deemed medically necessary in a life-threatening situation, the likelihood of a significant and potentially dangerous drop in blood pressure is increased. In such circumstances, nitrates should still only be administered under close medical supervision with appropriate haemodynamic monitoring (see Contraindications).
Medicinal products reducing systemic blood pressure: As a vasodilator, avanafil may reduce systemic blood pressure. If Spedra is used in combination with another medicinal product which reduces systemic blood pressure, the additive effects may result in symptomatic hypotension (e.g. dizziness, light-headedness, syncope or near-syncope). In phase III clinical trials no events of "hypotension" but occasional episodes of "dizziness" were observed (see Adverse Reactions). One episode of "syncope" was observed in placebo and one episode on 100 mg of avanafil in phase III clinical trials.
Patients with left ventricular outflow obstruction (e.g. aortic stenosis, idiopathic hypertrophic subaortic stenosis) and those with severely impaired autonomic control of blood pressure can be particularly sensitive to the actions of vasodilators including avanafil (see Precautions).
Alpha-blockers: Haemodynamic interactions with doxazosin and tamsulosin were studied in healthy subjects in a two-period crossover-design trial. In patients receiving stable doxazosin treatment, the placebo-subtracted mean maximum decreases in standing and supine systolic blood pressure following avanafil dosing were 2.5 mmHg and 6.0 mmHg, respectively. In total, 7/24 subjects experienced values or decreases from baseline that were of potential clinical significance following avanafil dosing (see Precautions).
In patients receiving stable tamsulosin treatment, the placebo-subtracted mean maximum decreases in standing and supine systolic blood pressure following avanafil dosing were 3.6 mmHg and 3.1 mmHg, respectively and 5/24 subjects experienced blood pressure values or decreases from baseline that were of potential clinical significance following avanafil dosing (see Precautions).
Antihypertensives other than alpha-blockers: A clinical study was conducted to assess the effect of avanafil on the potentiation of the blood pressure lowering effects of selected antihypertensive medicinal products (amlodipine and enalapril). Results showed a mean maximum decrease in supine blood pressure of 2/3 mmHg compared to placebo with enalapril and 1/-1 mmHg with amlodipine when avanafil was co-administered. There was a statistically significant difference in maximum decrease from baseline in supine diastolic blood pressure with enalapril and avanafil only, which returned to baseline 4 hours after the dose of avanafil. In both cohorts, one subject experienced a decrease in blood pressure without symptoms of hypotension, which resolved within 1 hour of onset. Avanafil had no effect on the pharmacokinetics of amlodipine, but amlodipine increased the maximum and total exposure of avanafil by 28% and 60%, respectively (see Precautions).
Alcohol: Consumption of alcohol in combination with avanafil can increase the potential for symptomatic hypotension. In a single-dose three-way crossover design study evaluating healthy subjects, the mean maximum reduction in diastolic blood pressure was significantly greater following avanafil administered in combination with alcohol than following avanafil alone (3.2 mmHg) or alcohol alone (5.0 mmHg) (see Precautions).
Other treatments for erectile dysfunction: The safety and efficacy of combinations of avanafil and other PDE5 inhibitors or other treatments for erectile dysfunction have not been studied (see Precautions).
Effects of other substances on avanafil: Avanafil is a substrate of and predominantly metabolised by CYP3A4. Studies have shown that medicinal products that inhibit CYP3A4 can increase avanafil exposure (see Dosage & Administration).
CYP3A4 Inhibitors: Ketoconazole (400 mg daily), a selective and highly potent inhibitor of CYP3A4, increased avanafil 50 mg single dose Cmax and exposure (AUC) equal to 3-fold and 14-fold respectively and prolonged the half-life of avanafil to approximately 9 hours. Ritonavir (600 mg twice daily), a highly potent CYP3A4 inhibitor, which also inhibits CYP2C9, increased avanafil 50 mg single-dose Cmax and AUC equal to approximately 2-fold and 13-fold, and prolonged the half-life of avanafil to approximately 9 hours. Other strong inhibitors of CYP3A4 (e.g. itraconazole, voriconazole, clarithromycin, nefazodone, saquinavir, nelfinavir, indinavir, atazanavir, and telithromycin) would be expected to have similar effects. Consequently, co-administration of avanafil with potent CYP3A4 inhibitors is contraindicated (see Dosage & Administration, Contraindications and Precautions).
Erythromycin (500 mg twice daily), a moderate CYP3A4 inhibitor, increased avanafil 200 mg single-dose Cmax and AUC equal to approximately 2-fold and 3-fold, respectively, and prolonged the half-life of avanafil to approximately 8 hours. Other moderate CYP3A4 inhibitors (e.g. amprenavir, aprepitant, diltiazem, fluconazole, fosamprenavir, and verapamil) would be expected to have similar effects. Consequently, the maximum recommended dose of avanafil is 100 mg, not to exceed once every 48 hours for patients taking concomitant moderate CYP3A4 inhibitors (see Dosage & Administration).
Although specific interactions have not been studied, other CYP3A4 inhibitors, including grapefruit juice would likely increase avanafil exposure. Patients should be advised to avoid grapefruit juice within 24 hours prior to taking avanafil.
CYP3A4 substrate: Amlodipine (5 mg daily) increased avanafil 200 mg single-dose Cmax and AUC by approximately 28% and 60%, respectively. These exposure changes are not considered clinically significant. There was no effect of a single dose of avanafil on amlodipine plasma levels.
Although specific interactions of avanafil with rivaroxaban and apixaban (both CYP3A4 substrates) have not been studied, an interaction is not expected.
Cytochrome P450 Inducers: The potential effect of CYP inducers, especially inducers of CYP3A4 (e.g. bosentan, carbamazepine, efavirenz, phenobarbital and rifampicin) on the pharmacokinetics and efficacy of avanafil has not been evaluated. The concomitant use of avanafil and a CYP inducer is not recommended as it may decrease the efficacy of avanafil.
Effects of avanafil on other medicinal products: Cytochrome P450 Inhibition: In in vitro studies in human liver microsomes, avanafil showed a negligible potential for drug-drug interactions with CYP1A1/2, 2A6, 2B6 and 2E1. Further, the metabolites of avanafil (M4, M16 and M27), also demonstrated a minimal inhibition of CYPs 1A1/2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1 and 3A4. Based on these data avanafil is not anticipated to have a significant effect on other medicinal products metabolised by these enzymes.
Since the in vitro data identified potential avanafil interactions with CYPs 2C19, 2C8/9, 2D6 and 3A4, further clinical studies using omeprazole, rosiglitazone and desipramine did not reveal clinically relevant interactions with CYPs 2C19, 2C8/9 and 2D6.
Cytochrome P450 Induction: The potential induction of CYP1A2, CYP2B6 and CYP3A4 by avanafil evaluated in primary human hepatocytes in vitro did not reveal any potential interaction at clinically relevant concentrations.
Transporters: In vitro results showed for avanafil a modest potential for acting as P-gp substrate and P-gp inhibitor with digoxin as a substrate at concentrations lower than the calculated intestinal concentration. The potential of avanafil to interfere with the transport of other medicinal products mediated by P-gp is not known.
Based on in vitro data, at clinically relevant concentrations avanafil could be an inhibitor of BCRP.
At clinically relevant concentrations avanafil is not an inhibitor of OATP1B1, OATP1B3, OCT1, OCT2, OAT1, OAT3 and BSEP.
The impact of avanafil on other transporters is unknown.
Riociguat: Preclinical studies showed additive systemic blood pressure lowering effect when PDE5 inhibitors were combined with riociguat. In clinical studies, riociguat has shown to augment the hypotensive effects of PDE5 inhibitors. There was no evidence of favourable clinical effect of the combination in the population studied. Concomitant use of riociguat with PDE5 inhibitors, including avanafil, is contraindicated (see Contraindications).
Incompatibilities: Not applicable.
Special precautions for disposal: No special requirements.
This medicinal product does not require any special storage conditions. Store below 30°C.
Shelf life: 4 years.
G04BE10 - avanafil ; Belongs to the class of drugs used in erectile dysfunction.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
