Pharmacotherapeutic Group: SINGULAIR (montelukast sodium) is a selective and orally active leukotriene receptor antagonist that specifically inhibits the cysteinyl leukotriene CysLT
1 receptor.
Pharmacology: Mechanism of Action: The cysteinyl leukotrienes (LTC
4, LTD
4, LTE
4), are potent inflammatory eicosanoids released from various cells including mast cells and eosinophils. These important pro-asthmatic mediators bind to cysteinyl leukotriene (CysLT) receptors. The CysLT type-1 (CysLT
1) receptor is found in the human airway (including airway smooth muscle cells and airway macrophages) and on other pro-inflammatory cells (including eosinophils and certain myeloid stem cells). CysLTs have been correlated with the pathophysiology of asthma and allergic rhinitis. In asthma, leukotriene-mediated effects include a number of airway actions, including bronchoconstriction, mucous secretion, vascular permeability, and eosinophil recruitment. In allergic rhinitis, CysLTs are released from the nasal mucosa after allergen exposure during both early- and late-phase reactions and are associated with symptoms of allergic rhinitis. Intranasal challenge with CysLTs has been shown to increase nasal airway resistance and symptoms of nasal obstruction.
Montelukast is a potent, orally active compound that significantly improves parameters of asthmatic inflammation. Based on biochemical and pharmacological bioassays, it binds with high affinity and selectivity to the CysLT
1 receptor (in preference to other pharmacologically important airway receptors such as the prostanoid, cholinergic, or β-adrenergic receptor). Montelukast potently inhibits physiologic actions of LTC
4, LTD
4, and LTE
4 at the CysLT
1 receptor without any agonist activity.
Pharmacodynamics: Montelukast causes potent inhibition of airway cysteinyl leukotriene receptors as demonstrated by the ability to inhibit bronchoconstriction due to inhaled LTD
4 in asthmatic patients. Doses as low as 5-mg cause substantial blockage of LTD
4-induced bronchoconstriction.
Montelukast causes bronchodilation within 2 hours of oral administration; these effects were additive to the bronchodilation caused by a β-agonist.
Clinical studies in adults 15 years of age and older demonstrated there is no additional clinical benefit to montelukast doses above 10 mg once daily. This was shown in two chronic asthma studies using doses up to 200 mg once daily and in one exercise challenge study using doses up to 50 mg, evaluated at the end of the once-daily dosing interval.
Clinical Studies: CLINICAL STUDIES - ASTHMA: ADULTS 15 YEARS OF AGE AND OLDER: The efficacy of SINGULAIR for the chronic treatment of asthma in adults 15 years of age and older was demonstrated in two (US and Multinational) similarly designed 12-week double-blind, placebo-controlled studies in 1325 patients (795 treated with SINGULAIR and 530 treated with placebo). Patients were symptomatic and using approximately 5 puffs of β-agonist per day on an "as-needed" basis. The mean baseline percent of predicted forced expiratory volume in 1 second (FEV
1) was 66% (approximate range, 40 to 90%). In these studies, asthma symptoms, asthma-related outcomes, respiratory function, and "as-needed" β-agonist use were measured. Endpoints were analyzed in each study and in a combined analysis according to a prespecified data analysis plan. The following clinical results were observed: Asthma Symptoms and Asthma-related Outcomes: SINGULAIR, 10 mg once daily in the evening, significantly improved measurements of patient-reported daytime symptoms and nighttime awakenings in each study and in the combined analysis, compared with placebo. In patients with nocturnal awakenings of at least 2 nights per week, SINGULAIR reduced the nocturnal awakenings by 34% from baseline, significantly better than the reduction of 14% for the placebo group (combined analysis).
SINGULAIR, compared with placebo, significantly improved asthma-related outcome measurements. In the combined analysis, SINGULAIR, compared with placebo, decreased asthma attacks by 37%, corticosteroid rescue by 39%, discontinuations due to worsening asthma by 65%, asthma exacerbations by 38% and increased asthma-free days by 42%.
Physicians' and patients' global asthma evaluations and asthma-specific quality-of-life evaluations (in all domains, including normal daily activity and asthma symptoms) were significantly better with SINGULAIR compared with placebo in each study and in the combined analysis.
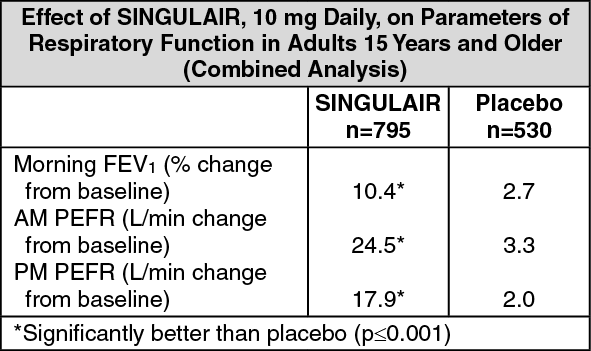
Respiratory Function: Compared with placebo, SINGULAIR caused significant improvements in parameters of respiratory function (FEV
1 and peak expiratory flow rate, PEFR) in each study and in the combined analysis: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
β-agonist Use: Compared with placebo, SINGULAIR significantly decreased the use of "as-needed" β-agonist by 26.1% from baseline compared with 4.6% in the placebo group in the combined analysis. The decreases were also significant in each of the studies (p ≤ 0.001).
Onset of Action and Maintenance of Benefits: In each study and in the combined analysis, the treatment effect of SINGULAIR, measured by daily diary card parameters, including symptom scores, "as-needed" β-agonist use, and PEFR measurements, was achieved after the first dose and was maintained throughout the dosing interval (24 hours). Treatment effect also remained constant during continuous once-daily administration in extension studies for up to one year. Withdrawal of SINGULAIR in asthmatic patients after 12 weeks of continuous use did not cause rebound worsening of asthma (see also EFFECTS ON EXERCISE-INDUCED BRONCHOCONSTRICTION as follows).
Effects Relative to Inhaled Corticosteroids: In one of the two 12-week double-blind studies in adults (Multinational), SINGULAIR was compared with inhaled beclomethasone (200 μg twice daily with a spacer device). SINGULAIR demonstrated a more rapid initial response, although over the full duration of the study beclomethasone provided a greater average treatment effect. However, a high percent of patients treated with SINGULAIR achieved similar clinical responses compared with inhaled beclomethasone.
PEDIATRIC PATIENTS 6 TO 14 YEARS OF AGE: The efficacy of SINGULAIR in pediatric patients 6 to 14 years of age was demonstrated in one 8-week double-blind, placebo-controlled study in 336 patients (201 treated with SINGULAIR and 135 treated with placebo) using β-agonist on an "as-needed" basis. The mean baseline percent predicted FEV
1 was 72% (approximate range, 45 to 90%) and approximately 36% of the patients were on inhaled corticosteroids.
Compared with placebo, SINGULAIR, one 5-mg chewable tablet daily in the evening, significantly decreased the percent of days asthma exacerbations occurred. Parents' global asthma evaluations and the pediatric asthma-specific quality-of-life evaluations (in all domains, including normal daily activity and asthma symptoms) were significantly better with SINGULAIR compared with placebo.
Compared with placebo, there was a significant improvement in morning FEV
1 (8.7% versus 4.2% change from baseline in the placebo group, p < 0.001) and a significant decrease in total "as-needed" β-agonist use (11.7% decrease from baseline versus 8.2% increase from baseline in the placebo group, p ≤ 0.050).
Similar to the adult studies, the treatment effect was achieved after the first dose and remained constant during continuous once-daily administration in clinical studies for up to 6 months.
In a 12-month study (MOntelukast Study of Asthma In Children; MOSAIC) comparing the efficacy of montelukast to inhaled fluticasone on asthma control in pediatric patients 6 to 14 years of age with mild persistent asthma, montelukast was non-inferior to fluticasone in increasing the percentage of asthma rescue-free days (LS mean of 83.6% and 86.4%, respectively). Both montelukast and fluticasone also improved asthma control on secondary endpoints: increased FEV
1 (0.27 L and 0.30 L change from baseline, respectively; p=0.232 between groups) and decreased days with β-agonist use (-22.7% and -25.4% change from baseline, respectively; p=0.003 between groups).
Growth Rate in Pediatric Patients: Two controlled clinical studies have demonstrated that montelukast did not affect the growth rate in prepubertal pediatric patients with asthma. In a study of children aged 6 to 11 years, growth rate as measured by lower leg length growth, was similar in patients treated with montelukast 5 mg once daily for 3 weeks compared with placebo, and was significantly lower in patients treated with inhaled budesonide (200 μg twice daily) for 3 weeks, compared with placebo. In a 56-week study in children aged 6 to 8 years, linear growth rate was similar in patients treated with montelukast 5 mg once daily and placebo (LS means for montelukast and placebo: 5.67 and 5.64 cm/year, respectively), and was significantly lower (LS mean: 4.86 cm/year) in patients treated with inhaled beclomethasone (200 μg twice daily), compared with placebo [difference in LS means (95% CI): -0.78 (-1.06, -0.49) cm/year]. Both montelukast and beclomethasone versus placebo demonstrated significant benefit in rescue medication use in these patients with mild asthma.
PEDIATRIC PATIENTS 6 MONTHS TO 5 YEARS OF AGE: The efficacy of SINGULAIR, one 4-mg chewable tablet daily in the evening, in pediatric patients 2 to 5 years of age was demonstrated in a 12-week double-blind, placebo-controlled study in 689 patients (461 treated with SINGULAIR and 228 treated with placebo). SINGULAIR significantly improved multiple asthma efficacy endpoints and improved parameters of asthma control.
SINGULAIR was significantly better compared with placebo in the following caregiver asthma diary efficacy endpoints: days with daytime asthma symptoms, daytime asthma symptom score (including coughing, wheezing, trouble breathing, and child activities), beta-agonist use, corticosteroid rescue, days without asthma, and overnight asthma symptoms (p < 0.05). Additionally, there was a favorable trend in treatment effect for the efficacy endpoint, asthma attack (p=0.107).
The physician's global assessment and the average of caregiver's and physician's global assessments of asthma were significantly better with SINGULAIR compared with placebo (p=0.007 and 0.015, respectively).
A treatment effect was achieved after the first dose. In addition, total blood eosinophil counts were significantly decreased (p=0.034).
In a 12-month, placebo-controlled study (PREvention of Viral Induced Asthma; PREVIA) in pediatric patients 2 to 5 years of age with mild asthma and episodic exacerbations, montelukast 4 mg once daily significantly reduced the rate of asthma exacerbation episodes compared with placebo.
Efficacy of SINGULAIR is supported in pediatric patients 6 months to 2 years of age by extrapolation from the demonstrated efficacy in patients 2 years of age and older with asthma, and is based on similar pharmacokinetic data, as well as the assumption that the disease course, pathophysiology and the drug's effect are substantially similar among these populations.
EFFECTS IN PATIENTS ON CONCOMITANT INHALED CORTICOSTEROIDS: Separate studies in adults demonstrated the ability of SINGULAIR to add to the clinical effect of inhaled corticosteroids, and to allow steroid tapering when used concomitantly.
Three large studies demonstrated SINGULAIR has additional benefits in patients taking corticosteroids. In a randomized, placebo-controlled, parallel-group study (n=226), stable asthmatic patients on initial inhaled corticosteroid doses of approximately 1600 μg per day reduced their steroid use by approximately 37% during a placebo run-in period. SINGULAIR allowed a further 47% reduction in inhaled corticosteroid dose compared with 30% for placebo over the 12-week active treatment period (p ≤ 0.050).
In another randomized, placebo-controlled, parallel-group study (n=642) in a similar population of patients maintained but not adequately controlled on inhaled corticosteroids (beclomethasone 400 μg/day), SINGULAIR provided additional clinical benefit, compared with placebo. Complete abrupt removal of beclomethasone in patients receiving both treatments caused clinical deterioration in some patients, suggesting that tapering inhaled corticosteroids as tolerated rather than abrupt removal of steroids is preferred.
In aspirin-sensitive asthmatic patients, nearly all of whom were receiving concomitant inhaled and/or oral corticosteroids, a 4-week randomized, parallel-group study (n=80) demonstrated that SINGULAIR, compared with placebo, resulted in significant improvement in parameters of asthma control.
EFFECTS ON EXERCISE-INDUCED BRONCHOCONSTRICTION: In a 12-week, parallel group study of 110 adult patients 15 years of age and older, SINGULAIR, 10 mg, prevented exercise-induced bronchoconstriction (EIB) as demonstrated by significant inhibition of the following, compared with placebo: the extent and duration of fall in FEV
1 over 60 minutes after exercise (as measured by the area under the % fall in FEV
1 versus time curve after exercise, AUC); the maximal percent fall in FEV
1 after exercise; the time to recovery to within 5% of the pre-exercise FEV
1.
Protection was consistent throughout the 12-week treatment period, indicating that tolerance did not occur. In a separate crossover study, protection was observed after two once-daily doses.
In pediatric patients 6 to 14 years of age, using the 5-mg chewable tablet, an identically designed cross-over study demonstrated similar protection and the protection was maintained throughout the dosing interval (24 hours).
EFFECTS ON ASTHMATIC INFLAMMATION: Several studies have shown SINGULAIR inhibits parameters of asthmatic inflammation. In a placebo-controlled crossover study (n=12), SINGULAIR inhibited early- and late-phase bronchoconstriction due to antigen challenge by 75 and 57%, respectively.
Because inflammatory cell (eosinophil) infiltration is an important feature of asthma, the effects of SINGULAIR on eosinophils in the peripheral blood and airway were examined. In Phase IIb/III clinical studies in adults, SINGULAIR significantly decreased peripheral blood eosinophils approximately 15% from baseline, compared with placebo. In pediatric patients 6 to 14 years of age, SINGULAIR also significantly decreased peripheral blood eosinophils 13% over the 8-week treatment period, compared with placebo.
In a 4-week, randomized, parallel group study (n=40) in adults, SINGULAIR significantly decreased airway eosinophils (as assessed in sputum) by 48% from baseline compared with an increase of 23% from baseline with placebo. In this study, peripheral blood eosinophils significantly decreased, and clinical asthma endpoints improved with treatment with SINGULAIR.
CLINICAL STUDIES - ALLERGIC RHINITIS: The efficacy of SINGULAIR for the treatment of seasonal allergic rhinitis was investigated in similarly designed randomized, 2-week, double-blind, placebo-controlled trials including 4924 patients (1751 patients were treated with SINGULAIR). Patients were 15 years of age and older with a history of seasonal allergic rhinitis, a positive skin test to at least one relevant seasonal allergen, and active symptoms of seasonal allergic rhinitis at study initiation.
In a combined analysis of three pivotal studies, SINGULAIR 10-mg tablets administered to 1189 patients once daily in the evening resulted in a statistically significant improvement in the primary endpoint, daytime nasal symptoms score, and its individual components (nasal congestion, rhinorrhea, nasal itching, and sneezing); nighttime symptoms score, and its individual components (nasal congestion upon awakening, difficulty going to sleep, and nighttime awakenings); daytime eye symptoms score, and its individual components (tearing, itchy, red, and puffy eyes); global evaluations of allergic rhinitis by patients and by physicians; and composite symptoms score (composed of the daytime nasal and nighttime symptoms scores), compared with placebo.
In a separate 4-week study in which SINGULAIR was administered once daily in the morning, the efficacy over the initial 2 weeks was significantly different from placebo and consistent with the effect observed in studies using evening dosing. Additionally, the effect over the entire 4 weeks was consistent with the 2-week results.
In patients with seasonal allergic rhinitis aged 15 years and older who received SINGULAIR, a median decrease of 13% in peripheral blood eosinophil counts was noted, compared with placebo, over the double-blind treatment periods.
The efficacy of SINGULAIR for the treatment of perennial allergic rhinitis was investigated in two, similarly designed randomized, 6-week, double-blind, placebo-controlled studies including 3235 patients (1632 patients were treated with SINGULAIR). Patients were 15 to 82 years of age with a history of perennial allergic rhinitis, positive skin test results to relevant perennial allergens (including dust mites, animal dander, and mold spores), and active symptoms of perennial allergic rhinitis at study initiation.
In one study, SINGULAIR 10-mg tablets administered to 1000 patients once daily resulted in a statistically significant improvement in the primary endpoint, Daytime Nasal Symptoms score, and its individual components (nasal congestion, rhinorrhea, and sneezing), compared with placebo. SINGULAIR also demonstrated patient-perceived improvement of allergic rhinitis as assessed by the secondary endpoints of Global Evaluation of Allergic Rhinitis by Patient, and Rhinoconjunctivitis Quality-of-Life overall score (average of scores for the 7 domains of activity, sleep, non-nose/non-eye symptoms, practical problems, nasal symptoms, eye symptoms, and emotions), compared with placebo.
The efficacy of SINGULAIR for the treatment of seasonal allergic rhinitis in pediatric patients 2 to 14 years of age, and for the treatment of perennial allergic rhinitis in pediatric patients 6 months to 14 years of age is supported by extrapolation from the demonstrated efficacy in patients 15 years of age and older with allergic rhinitis as well as the assumption that the disease course, pathophysiology and the drug's effect are substantially similar among these populations.
Pharmacokinetics: Absorption: Montelukast is rapidly and nearly completely absorbed following oral administration. For the 10-mg film-coated tablet, the mean peak plasma concentration (C
max) is achieved 3 hours (T
max) after administration in adults in the fasted state. The mean oral bioavailability is 64%. The oral bioavailability and C
max are not influenced by a standard meal.
For the 5-mg chewable tablet, the C
max is achieved 2 hours after administration in adults in the fasted state. The mean oral bioavailability is 73%. Food does not have a clinically important influence with chronic administration.
For the 4-mg chewable tablet, C
max is achieved 2 hours after administration in pediatric patients 2 to 5 years of age in the fasted state.
The 4-mg oral granule formulation is bioequivalent to the 4-mg chewable tablet when administered to adults in the fasted state. The coadministration of applesauce or a standard meal with the oral granule formulation did not have a clinically meaningful effect on the pharmacokinetics of montelukast as determined by AUC (1225.7 vs 1223.1 ng·hr/mL with and without applesauce, respectively and 1191.8 vs 1148.5 ng·hr/mL with and without a standard meal, respectively).
Safety and efficacy were demonstrated in clinical studies where the 4-mg chewable tablet, 5-mg chewable tablet, and 10-mg film-coated tablet were administered without regard to the timing of food ingestion. The safety of SINGULAIR was also demonstrated in a clinical study in which the 4-mg oral granules were administered without regard to the timing of food ingestion.
Distribution: Montelukast is more than 99% bound to plasma proteins. The steady-state volume of distribution of montelukast averages 8 to 11 liters. Studies in rats with radiolabeled montelukast indicate minimal distribution across the blood-brain barrier. In addition, concentrations of radiolabeled material at 24 hours postdose were minimal in all other tissues.
Metabolism: Montelukast is extensively metabolized. In studies with therapeutic doses, plasma concentrations of metabolites of montelukast are undetectable at steady state in adults and pediatric patients.
In vitro studies using human liver microsomes indicate that cytochrome P450 3A4, 2C8 and 2C9 are involved in the metabolism of montelukast. Based on further
in vitro results in human liver microsomes, therapeutic plasma concentrations of montelukast do not inhibit cytochromes P450 3A4, 2C9, 1A2, 2A6, 2C19, or 2D6.
Elimination: The plasma clearance of montelukast averages 45 mL/min in healthy adults. Following an oral dose of radiolabeled montelukast, 86% of the radioactivity was recovered in 5-day fecal collections and <0.2% was recovered in urine. Coupled with estimates of montelukast oral bioavailability, this indicates montelukast and its metabolites are excreted almost exclusively
via the bile.
In several studies, the mean plasma half-life of montelukast ranged from 2.7 to 5.5 hours in healthy young adults. The pharmacokinetics of montelukast are nearly linear for oral doses up to 50 mg. No difference in pharmacokinetics was noted between dosing in the morning or in the evening. During once-daily dosing with 10-mg montelukast, there is little accumulation of the parent drug in plasma (~14%).
The comparative pharmacokinetics of montelukast when administered as two 5-mg chewable tablets versus one 10-mg film-coated tablet have not been evaluated. Therefore these two products should not be used interchangeably.
Characteristics in Patients: Gender: The pharmacokinetics of montelukast are similar in males and females.
Elderly: The pharmacokinetic profile and the oral bioavailability of a single 10-mg oral dose of montelukast are similar in elderly and younger adults. The plasma half-life of montelukast is slightly longer in the elderly. No dosage adjustment in the elderly is required.
Race: Pharmacokinetic differences due to race have not been studied. In clinical studies, there do not appear to be any differences in clinically important effects.
Hepatic Insufficiency: Patients with mild-to-moderate hepatic insufficiency and clinical evidence of cirrhosis had evidence of decreased metabolism of montelukast resulting in approximately 41% higher mean montelukast area under the plasma concentration curve (AUC) following a single 10-mg dose. The elimination of montelukast is slightly prolonged compared with that in healthy subjects (mean half-life, 7.4 hours). No dosage adjustment is required in patients with mild-to-moderate hepatic insufficiency. There are no clinical data in patients with severe hepatic insufficiency (Child-Pugh score > 9).
Renal Insufficiency: Since montelukast and its metabolites are not excreted in the urine, the pharmacokinetics of montelukast were not evaluated in patients with renal insufficiency. No dosage adjustment is recommended in these patients.
Adolescents and Pediatric Patients: The plasma concentration profile of montelukast following administration of the 10-mg film-coated tablet is similar in adolescents ≥15 years old and young adults. The 10-mg film-coated tablet is recommended for use in patients ≥15 years old.
Pharmacokinetic studies show that the plasma profiles of the 4-mg oral granule formulation in pediatric patients 6 months to 2 years of age, the 4-mg chewable tablet in pediatric patients 2 to 5 years of age, and the 5-mg chewable tablet in pediatric patients 6 to 14 years of age were similar to the plasma profile of the 10-mg film-coated tablet in adults.
Toxicology: Animal Toxicology: Acute Toxicity: No mortality occurred following a single oral administration of montelukast sodium at doses up to 5000 mg/kg, in mice and rats, (15,000 mg/m
2 and 29,500 mg/m
2 in mice and rats, respectively) the maximum dose tested (oral a LD
50 >5000 mg/kg). This dose is equivalent to 25,000 times the recommended daily adult human dose*.
Chronic Toxicity: The toxic potential of montelukast sodium was evaluated in a series of repeated dose toxicity studies of up to 53 weeks in monkeys and rats and up to 14 weeks in infant monkeys and in mice. Montelukast sodium was well tolerated at doses which provide a wide margin of safety based on total dose administered. The no effect level for all toxicological parameters in any of the species tested was at least 125 times the recommended human dose*. There were no findings that would preclude administration at the therapeutic dosage level for both adults and pediatric patients.
Carcinogenicity: Montelukast sodium was not carcinogenic when administered at oral doses of up to 200 mg/kg/day in a 106-week study in rats, or at oral doses of up to 100 mg/kg/day in a 92-week study in mice. These doses are equivalent to 1000 times and 500 times the recommended adult human dose*.
Mutagenesis: Montelukast sodium was found to be neither genotoxic nor mutagenic. Montelukast sodium was negative in the
in vitro microbial mutagenesis assay and the V-79 mammalian cell mutagenesis assays, with and without metabolic activation. There was no evidence of genotoxicity in the
in vitro alkaline elution assay in rat hepatocytes and the
in vitro chromosomal aberration assays in Chinese hamster ovary cells, with or without a microsomal enzyme activation system. Similarly, there was no induction of chromosomal aberrations in bone marrow cells of male or female mice after the administration of oral doses of up to 1200 mg/kg (3600 mg/m
2) (6000 times the recommended daily adult dose*).
Reproduction: Fertility and reproductive performance were not affected in studies with male rats given oral doses of up to 800 mg/kg/day or with female rats given doses of up to 100 mg/kg/day. These dosage provide margins of 4000-fold and 500-fold respectively above the recommended adult human dose*.
*Based on an adult patient weight of 50 kg.
Development: In developmental toxicity studies, there were no treatment related adverse effects at doses up to 400 mg/kg/day in rats and up to 100 mg/kg/day in rabbits. Fetal exposure of montelukast sodium in rats and rabbits does occur and significant concentrations of drug were observed in milk of lactating rats.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out
