Solution for injection: Saizen Liquid 6 mg solution for injection: Each cartridge contains 1.03 ml solution (6 mg somatropin*).
Saizen Liquid 12 mg & 20 mg for injection: Each cartridge contains 1.50 ml solution (12 mg somatropin*) or 2.50 ml solution (20 mg somatropin*).
*recombinant human growth hormone, produced by recombinant DNA technology in mammalian cells.
pH of 5.6-6.6 and osmolality 250-450 mOsm/kg.
Powder for injection 3.33 mg vial: Each vial of Saizen 3.33 mg contains somatropin* (recombinant human growth hormone).
*produced by recombinant DNA technology in mammalian cells.
After reconstitution with the enclosed solvent, each vial shall contain ≥ 0.67 mg of Saizen/ml.
Appearance of the solvent: clear colourless solution.
The pH of the reconstituted solution is 7.4-8.5.
Powder for injection 8 mg click.easy vial: Each vial of Saizen 8 mg click.easy contains 8 mg somatropin* (recombinant human growth hormone).
*produced by recombinant DNA technology in mammalian cells.
Reconstitution with the contents of the bacteriostatic solvent cartridge gives a concentration of 5.83 mg/ml.
The pH of the reconstituted solution is 6.5-8.5.
Excipients/Inactive Ingredients: Solution for injection: Sucrose, Poloxamer 188, Phenol, Citric Acid (for pH adjustment), Sodium Hydroxide (for pH adjustment), Water for Injection.
Powder for injection 3.33 mg vial: Powder: Mannitol, Disodium phosphate dihydrate, Sodium dihydrogen phosphate monohydrate.
Solvent: Sodium chloride (0.9% w/v) and benzyl alcohol (0.9% w/v, as preservative) solution for injection.
Powder for injection 8 mg click.easy vial: Powder: Sucrose, Phosphoric acid (for pH-adjustment), Sodium Hydroxide (for pH-adjustment).
Solvent: Metacresol (as preservative 0.3% w/v) solution in water for injection.
Pharmacotherapeutic group: Anterior pituitary lobe hormones and analogues. ATC code: H01AC01.
Pharmacology: Pharmacodynamics: Saizen contains recombinant human growth hormone (r-hGH) produced by genetically engineered mammalian cells.
It is a peptide of 191 amino acids identical to human pituitary growth hormone with respect to amino acid sequence and composition as well as peptide map, isoelectric point, molecular weight, isomeric structure and bioactivity.
Growth hormone is synthesised in a transformed murine cell line that has been modified by the addition of the gene for pituitary growth hormone.
Saizen is an anabolic and anticatabolic agent, which exerts effects not only on growth but also on body composition and metabolism. It interacts with specific receptors on a variety of cell types including myocytes, hepatocytes, adipocytes, lymphocytes and hematopoietic cells. Some, but not all of its effects are mediated through another class of hormones known as somatomedins (IGF-1 and IGF-2).
Depending on the dose, the administration of Saizen elicits a rise in IGF-1, IGFBP-3, non-esterified fatty acids and glycerol, a decrease in blood urea, and decreases in urinary nitrogen, sodium and potassium excretion. The duration of the increase in growth hormone levels may play a role in determining the magnitude of the effects. A relative saturation of the effects of Saizen at high doses is probable. This is not the case for glycaemia and urinary C-peptide excretion, which are significantly elevated after high doses (20 mg).
In a randomised clinical trial, three years treatment of pre-pubertal short children born SGA with a dose of 0.067 mg/kg/day resulted in a mean gain of +1.8 height-SDS. In those children who did not receive treatment beyond 3 years, part of the treatment benefit was lost, but the patients retained a significant gain of +0.7 height-SDS at final height (p<0.01 compared to baseline). Patients who received a second treatment course after a variable period of observation experienced a total gain of +1.3 height-SDS (p<0.001 [for Solution for injection/Powder for injection 8 mg clickeasy vial only] & p=0.001 [for Powder for injection 3.33 mg vial only] compared to baseline) at final height. (The mean cumulative treatment duration in the latter group was 6.1 years.) The gain in height-SDS (+1.3±1.1) at final height in this group was significantly (p<0.05) different from the gain in height-SDS obtained in the first group (+0.7±0.8) that received only 3.0 years of treatment on average.
A second clinical trial investigated two different dose regimens over four years. One group was treated with 0.067 mg/kg/day for 2 years and then observed without treatment for 2 years. The second group received 0.067 mg/kg/day in the first and third year and no treatment in the second and fourth year. Either treatment regimen resulted in a cumulative administered dose of 0.033 mg/kg/day over the four-year study period. Both groups showed a comparable acceleration of growth and a significant improvement of +1.55 (p<0.0001) and + 1.43 (p<0.0001) height-SDS respectively at the end of the four year study period. Long-term safety data are still limited.
Pharmacokinetics: The pharmacokinetics of Saizen are linear at least up to doses of 8 IU (2.67 mg). At higher doses (60 IU/20 mg) some degree of non-linearity cannot be ruled out, however with no clinical relevance.
Following intravenous administration in healthy volunteers the volume of distribution at steady-state is around 7 L, total metabolic clearance is around 15 L/h, while the renal clearance is negligible, and the drug exhibits an elimination half-life of 20 to 35 min.
Following single-dose subcutaneous and intramuscular administration of Saizen, the apparent terminal half-life is much longer, around 2 to 4 hours. This is due to a rate limiting absorption process.
Maximum serum growth hormone concentrations are reached after approximately 4 hours and serum growth hormone levels return to baseline within 24 hours, indicating that no accumulation of growth hormone will occur during repeated administrations.
The absolute bioavailability of both routes is 70-90%.
Solution for injection: Saizen solutions for injection (5.83 and 8.00 mg/ml) administered subcutaneously have been shown to be bioequivalent versus the 8 mg freeze-dried formulation.
Renal impairment: Somatropin clearance is known to be reduced in patients with renal impairment. However, the clinical significance of this finding is unknown.
For prepubertal children with growth failure due to chronic renal failure a specific posology is recommended (see Dosage & Administration).
Hepatic impairment: Somatropin clearance is known to be reduced in patients with hepatic impairment. However, as Saizen has not been studied in patients with hepatic impairment, the clinical significance of this finding is unknown.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for human based on conventional studies of safety pharmacology, single and repeated dose toxicity and genotoxicity. Formal carcinogenicity bioassays were not performed. This is justified, given the proteinous nature of the drug substance and the negative outcome of the genotoxicity testing. The potential effects of recombinant human growth hormone on the growth of pre-existing tumours have been evaluated through in vitro and in vivo experiments which have shown that recombinant human growth hormone is not expected to cause or stimulate tumours in patients.
Reproductive toxicology studies do not indicate any adverse effect on fertility and reproduction, despite administration of doses sufficiently high to produce some pharmacological effects on growth.
Solution for injection: The local tolerability of Saizen solution for injection was shown to be good and suitable for subcutaneous administration, when injected in animals at a concentration of 8.00 mg/m1 and volumes of 1 ml/site.
Powder for injection 8 mg click.easy vial: The local tolerability of Saizen solutions containing 0.3% metacresol when injected in animals was considered good and found suitable for subcutaneous or intramuscular administration.
Saizen is indicated in the treatment of: growth failure in children caused by decreased or absent secretion of endogenous growth hormone; growth failure in girls with gonadal dysgenesis (Turner Syndrome), confirmed by chromosomal analysis; growth disturbance (current height SDS < -2.5 and parental adjusted height SDS < -1) in short children born small for gestational age (SGA) with a birth weight and/or length below - 2 SD, who failed to show catch-up growth (HV SDS < 0 during the last year) by 4 years of age or later; replacement therapy in adults with pronounced growth hormone deficiency as diagnosed by a single dynamic test for growth hormone deficiency.
Patients must also fulfill the following criteria: Childhood Onset: Patients who were diagnosed as growth hormone deficient during childhood, must be retested and their growth hormone deficiency confirmed before replacement therapy with Saizen is started.
Adult Onset: Patients must have growth hormone deficiency as a result of hypothalamic or pituitary disease and at least one other hormone deficiency diagnosed (except for prolactin) and adequate replacement therapy instituted, before replacement therapy using growth hormone may begin.
Saizen is intended for multiple dose use in an individual patient.
Saizen dosage should be individualised for each patient based on body surface area (BSA) or on body weight (BW).
Posology: It is recommended that Saizen be administered at bedtime according to the following dosage: Children and adolescents: Growth failure due to inadequate endogenous growth hormone secretion: 0.7-1.0 mg/m2 body surface area per day or 0.025-0.035 mg/kg body weight (BW) per day by subcutaneous administration or intramuscular administration (for Powder for injection 3.33 mg vial).
Growth failure in girls due to gonadal dysgenesis (Turner Syndrome): 1.4 mg/m2 body surface area (BSA) per day or 0.045-0.050 mg/kg body weight (BW) per day by subcutaneous administration.
Concomitant therapy with non-androgenic anabolic steroids in patients with Turner Syndrome can enhance the growth response.
Growth failure in prepubertal children due to chronic renal failure (CRF): 1.4 mg/m2 body surface area (BSA), approximately equal to 0.045-0.050 mg/kg body weight (BW), per day by subcutaneous administration.
Growth failure in short children born small for gestational age (SGA): The recommended daily dose is 0.035 mg/kg body weight (or 1 mg/m2/day, equal to 0.1 U/kg/day or 3 IU/m2/day) per day, by subcutaneous administration.
Treatment should be discontinued when the patient has reached a satisfactory adult height, or the epiphyses are fused.
For growth disturbance in short children born SGA, treatment is usually recommended until final height is reached. Treatment should be discontinued after the first year if height velocity SDS is below +1. Treatment should be discontinued when final height is reached (defined as height velocity <2 cm/year), and if confirmation is required if bone age is >14 years (girls) or >16 years (boys), corresponding to closure of the epiphyseal growth plates.
Adults: Growth Hormone Deficiency in adults: At the start of somatropin therapy, low doses of 0.15-0.3 mg are recommended, given as a daily subcutaneous injection. The dose should be adjusted stepwise, controlled by Insulin-like Growth Factor 1 (IGF-1) values. The recommended final growth hormone dose seldom exceeds 1.0 mg/day. In general the lowest efficacious dose should be administered. Women may require higher doses than men, with men showing an increasing IGF-1 sensitivity over time. This means that there is a risk that women, especially those on oral oestrogen replacement are under-treated while men are over-treated. In older or overweight patients, lower doses may be necessary.
Patients with renal or hepatic impairment: Currently available data are described in Pharmacology: Pharmacokinetics under Actions but no recommendation on a posology can be made.
Powder for injection 3.33 mg vial: Benzyl alcohol as a preservative in bacteriostatic sodium chloride solution may cause toxic reactions and anaphylactoid reactions in infants and children up to 3 years old and must not be given to premature babies or neonates. Saizen may be reconstituted with Sodium Chloride Injection BP or Sterile Water for Injections for immediate use when administering to children under 3 years of age.
Method of administration: Solution for injection: For administration of the solution for injection of Saizen follow the instructions given in the package leaflet and in the instruction manual provided with the selected injector: cool.click needle-free auto-injectors, easypod auto-injector or aluetta pen injector.
Intended users of easypod are primarily children starting from the age of 7 up to adults. Use of the devices by children should always be made under adult's supervision.
For instructions for handling please see Special precautions for disposal and other handling under Cautions for Usage.
Powder for injection 3.33 mg vial: The powder for solution for injection should be used with the enclosed solvent for parenteral use. The reconstituted solution for injection should be clear with no particles. For instructions for preparation, please see Instructions for use/handling under Cautions for Usage.
Powder for injection 8 mg click.easy vial: For administration of the reconstituted solution for injection of Saizen 8 mg click.easy follow the instructions given in the package leaflet and in the instruction manual provided with the selected auto injector: one.click auto-injector, cool.click needle-free auto-injectors or easypod auto-injector.
Intended users of easypod are primarily children starting from the age of 7 up to adults. Use of the devices by children should always be made under adult's supervision.
The powder for solution for injection must be reconstituted with the enclosed bacteriostatic solvent (0.3% (w/v) metacresol solution in water for injections) for parenteral use, using the click.easy reconstitution device. For instructions for preparation please see Instructions for use/handling under Cautions for Usage.
Exceeding the recommended doses can cause side effects. Overdosage can lead to hypoglycaemia and subsequently to hyperglycaemia. Moreover, somatropin overdose is likely to cause manifestations of fluid retention.
Hypersensitivity to the active ingredient or to any of the excipients.
Somatropin should not be used for growth promotion in children with closed epiphyses.
Somatropin must not be used when there is any evidence of activity of a tumour. Intracranial tumours must be inactive and antitumour therapy must be completed prior to starting GH therapy. Treatment should be discontinued if there is evidence of tumour growth.
Somatropin must not be used in case of proliferative or preproliferative diabetic retinopathy.
Patients with acute critical illness suffering complications following open heart surgery, abdominal surgery, multiple accidental trauma, acute respiratory failure or similar conditions should not be treated with somatropin.
In children with chronic renal disease, treatment with somatropin should be discontinued at renal transplantation.
Treatment should be carried out under the regular guidance of a physician who is experienced in the diagnosis and management of patients with growth hormone deficiency.
The maximum recommended daily dose should not be exceeded (see Dosage & Administration).
Neoplasm: Patients with an intra- or extra-cranial neoplasia in remission who are receiving treatment with growth hormone should be examined carefully and at regular intervals by the physician.
Patients with growth hormone deficiency secondary to an intracranial tumour should be examined frequently for progression or recurrence of the underlying disease process.
In childhood cancer survivors, an increased risk of a second neoplasm has been reported in patients treated with somatropin after their first neoplasm. Intracranial tumours, in particular meningiomas, in patients treated with radiation to the head for their first neoplasm, were the most common of these second neoplasms.
Prader-Willi Syndrome: Saizen is not indicated for the long-term treatment of paediatric patients who have growth failure due to genetically confirmed Prader-Willi Syndrome, unless they also have a diagnosis of growth hormone deficiency. There have been reports of sleep apnoea and sudden death after initiating therapy with growth hormone in paediatric patients with Prader-Willi Syndrome who had one or more of the following risk factors: severe obesity, history of upper airway obstruction or sleep apnoea, or unidentified respiratory infection.
Leukaemia: Leukaemia has been reported in a small number of growth hormone deficiency patients, some of whom have been treated with somatropin. However, there is no evidence that leukaemia incidence is increased in growth hormone recipients without predisposition factors.
Insulin sensitivity: Because somatropin may reduce insulin sensitivity, patients should be monitored for evidence of glucose intolerance. For patients with diabetes mellitus, the insulin dose may require adjustment after somatropin containing product therapy is instituted. Patients with diabetes or glucose intolerance should be monitored closely during somatropin therapy.
Retinopathy: Stable background retinopathy should not lead to discontinuation of somatropin replacement therapy.
Thyroid function: Growth hormone increases the extra thyroid conversion of T4 to T3 and may, as such, unmask incipient hypothyroidism. Monitoring of thyroid function should therefore be conducted in all patients. In patients with hypopituitarism, standard replacement therapy must be closely monitored when somatropin therapy is administered.
Benign intracranial hypertension: In cases of severe or recurrent headache, visual problems, nausea and/or vomiting, a funduscopy for papilloedema is recommended. If papilloedema is confirmed, a diagnosis of benign intracranial hypertension (or pseudotumor cerebri) should be considered and if appropriate, Saizen treatment should be discontinued. At present, there is insufficient evidence to guide clinical decision-making in patients with resolved intracranial hypertension. If growth hormone is restarted, careful monitoring for symptoms of intracranial hypertension is necessary.
Pancreatitis: Although rare, pancreatitis should be considered in somatropin-treated patients, especially children who develop abdominal pain.
Scoliosis: Scoliosis is known to be more frequent in some of the patient groups treated with somatropin, for example Turner syndrome. In addition, rapid growth in any child can cause progression of scoliosis. Somatropin has not been shown to increase the incidence or severity of scoliosis. Signs of scoliosis should be monitored during treatment.
Antibodies: As with all somatropin containing products, a small percentage of patients may develop antibodies to somatropin. The binding capacity of these antibodies is low and there is no effect on growth rate. Testing for antibodies to somatropin should be carried out in any patient who fails to respond to therapy.
Slipped capital femoral epiphysis: Slipped capital femoral epiphysis is often associated with endocrine disorders such as growth hormone deficiency and hypothyroidism, and with growth spurts. In children treated with growth hormone, slipped capital femoral epiphysis may either be due to underlying endocrine disorders or to the increased growth velocity caused by the treatment. Growth spurts may increase the risk of joint-related problems, the hip joint being under particular strain during the prepubertal growth spurt. Physicians and parents should be alert to the development of a limp or complaints of hip or knee pain in children treated with Saizen.
Growth failure due to chronic renal failure: Patients with growth failure due to chronic renal failure should be examined periodically for evidence of progression of renal osteodystrophy. Slipped capital femoral epiphysis or avascular necrosis of the femoral head may be seen in children with advanced renal osteodystrophy and it is uncertain whether these problems are affected by growth hormone therapy. X rays of the hip should be obtained prior to initiating therapy.
In children with chronic renal failure, renal function should have decreased to below 50% of normal before therapy is instituted. To verify the growth disturbance, growth should have been followed for a year before institution of therapy. Conservative treatment for renal insufficiency (which includes control of acidosis, hyperparathyroidism and nutritional status for one year prior to the treatment) should have been established and should be maintained during treatment. Treatment should be discontinued at the time of renal transplantation.
Children born small for gestational age (SGA): In short children born SGA other medical reasons or treatments that could explain growth disturbance should be ruled out before starting treatment.
For SGA patients it is recommended to measure fasting insulin and blood glucose before start of treatment and annually thereafter. In patients with increased risk for diabetes mellitus (e.g. familial history of diabetes, obesity, increased body mass index, severe insulin resistance, acanthosis nigricans) oral glucose tolerance testing (OGTT) should be performed. If overt diabetes occurs, growth hormone should not be administered.
For SGA patients it is recommended to measure IGF-I level before start of treatment and twice a year thereafter. If on repeated measurements IGF-I levels exceed +2 SD compared to references for age and pubertal status, the IGF-I/IGFBP-3 ratio could be taken into account to consider dose adjustment.
Experience in initiating treatment in SGA patients near onset of puberty is limited. It is therefore not recommended to initiate treatment near onset of puberty. Experience with SGA patients with Silver-Russel syndrome is limited.
Some of the height gain obtained with treating short children born SGA with somatropin may be lost if treatment is stopped before final height is reached.
Fluid retention: Fluid retention is expected during growth hormone replacement therapy in adults.
In case of persistent oedema or severe paraesthesia the dosage should be decreased in order to avoid the development of carpal tunnel syndrome.
Acute critical illness: In all patients developing acute critical illness, the possible benefit of treatment with somatropin must be weighed against the potential risk involved.
Interaction with glucocorticoids: Initiation of growth hormone replacement may unmask secondary adrenal insufficiency in some patients by reducing the activity of 11β-hydroxysteroid dehydrogenase, type 1 (11β-HSD1), an enzyme converting inactive cortisone to cortisol and glucocorticoid replacement may be required. Initiation of somatropin in patients receiving glucocorticoid replacement therapy may lead to manifestation of cortisol deficiency. Adjustment of glucocorticoid dose may be required (see Interactions).
Use with oral oestrogen therapy: If a woman taking somatropin begins oral oestrogen therapy, the dose of somatropin may need to be increased to maintain the serum IGF-1 levels within the normal age-appropriate range. Conversely, if a woman on somatropin discontinues oral oestrogen therapy, the dose of somatropin may need to be reduced to avoid excess of growth hormone and/or side effects (see Interactions).
General: The injection site should be varied to prevent lipoatrophy.
Growth Hormone Deficiency in the adult is a lifelong condition and should be treated accordingly, however experience with patients over sixty years and experience with prolonged treatment is limited.
Powder for injection 3.33 mg vial: Benzyl alcohol as a preservative in bacteriostatic sodium chloride solution may cause toxic reactions and anaphylactoid reactions in infants and children up to 3 years old and must not be given to premature babies or neonates. Saizen may be reconstituted with Sodium Chloride Injection BP or Sterile Water for Injections for immediate use when administering to children under 3 years of age.
Effects on ability to drive and use machines: Saizen has no influence on the ability to drive and use machines.
Pregnancy: Solution for injection: From the reproductive studies performed in animals with somatropin containing products, there is no evidence of an increased risk of adverse reactions for the embryo or foetus. There are no data from the use of somatropin during pregnancy in animals (see Pharmacology: Toxicology: Preclinical safety data under Actions). Therefore, somatropin containing products are not recommended during pregnancy and in woman of childbearing potential not using contraception.
Powder for injection 3.33 mg vial/Powder for injection 8 mg click.easy vial: Animal studies are insufficient and/or animal data is not available with regard to effects on pregnancy, embryofoetal development, parturition or postnatal development (see Pharmacology: Toxicology: Preclinical safety data under Actions). No clinical data on exposed pregnancies are available. Therefore, somatropin containing products are not recommended during pregnancy and in woman of childbearing potential not using contraception.
Breastfeeding: There have been no clinical studies conducted with somatropin in breast-feeding women. It is not known whether somatropin is excreted in human milk. Therefore caution should be exercised when somatropin is administered to breast-feeding women.
Fertility: Non-clinical toxicity studies showed that recombinant human growth hormone did not induce adverse effects on male and female fertility (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Up to 10% of patients may experience redness and itching at the site of injection, particularly when the subcutaneous route is used.
Fluid retention is expected during growth hormone replacement therapy in adults. Oedema, joint swelling, arthralgias, myalgias and paraesthesias may be clinical manifestations of fluid retention. However, these symptoms/signs are usually transient and dose dependent.
Adult patients with growth hormone deficiency, following diagnosis of growth hormone deficiency in childhood, reported side-effects less frequently than those with adult onset growth hormone deficiency.
Antibodies to somatropin can form in a small percentage of patients; to date the antibodies have been of low binding capacity and have not been associated with growth attenuation except in patients with gene deletions. In very rare instances, where short stature is due to deletion of the growth hormone gene complex, treatment with growth hormone may induce growth attenuating antibodies.
Leukaemia has been reported in a small number of growth hormone deficiency patients, some of whom have been treated with somatropin. However, there is no evidence that leukaemia incidence is increased in growth hormone recipients without predisposing factors.
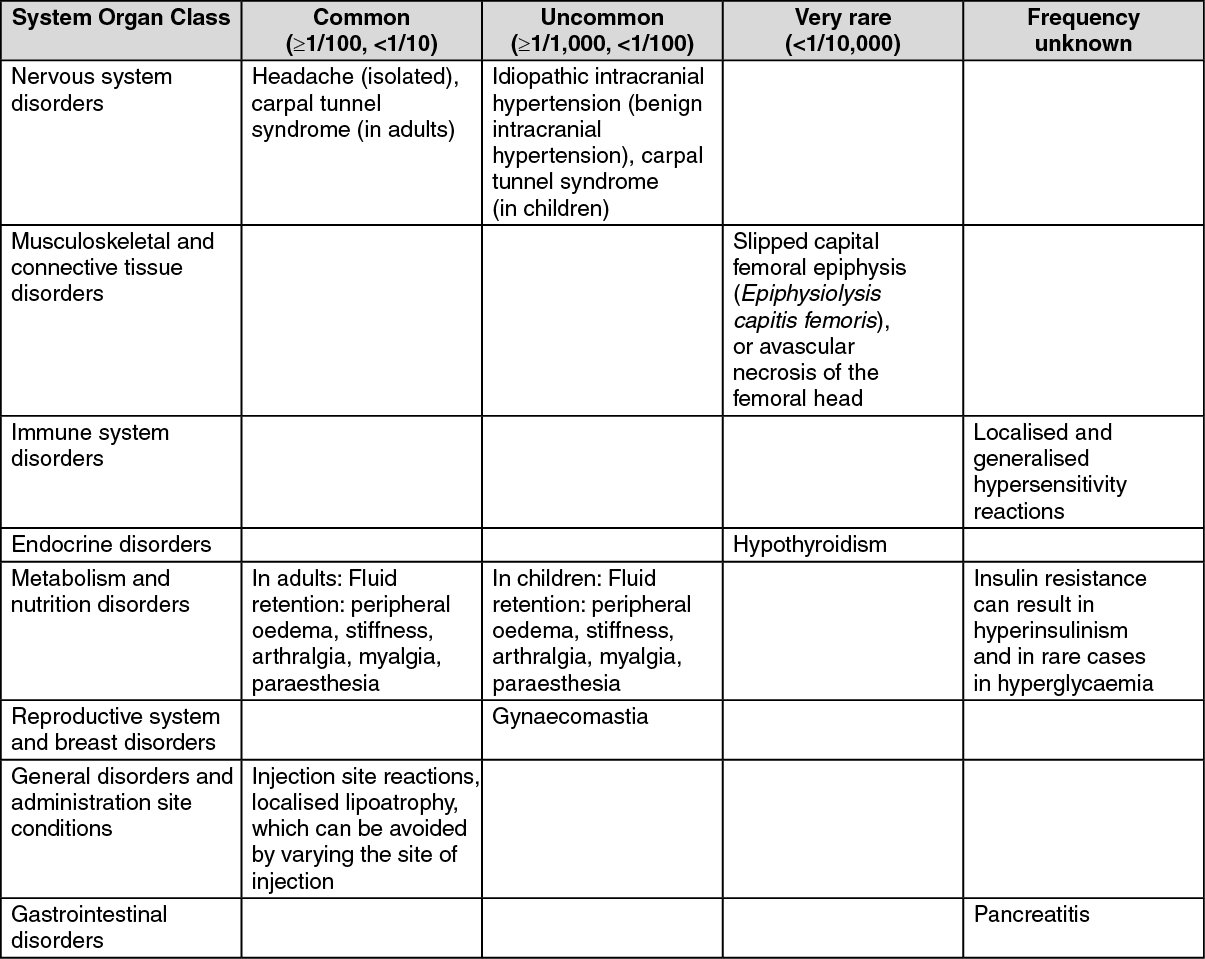
The following definitions apply to the frequency terminology used hereafter: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), frequency not known (cannot be estimated from the available data).
Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Reporting of suspected adverse reactions: Powder for injection 3.33 mg vial/Powder for injection 8 mg click.easy vial:
Click on icon to see table/diagram/image
Reporting of suspected adverse reactions: Powder for injection 3.33 mg vial/Powder for injection 8 mg click.easy vial: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
Concomitant treatment with glucocorticoids/corticosteroids inhibits the growth promotion effects of Saizen. Patients with ACTH deficiency should have their glucocorticoid replacement therapy carefully adjusted to avoid any inhibitory effect on growth hormone.
Growth hormone decreases the conversion of cortisone to cortisol and may unmask previously undiscovered central hypoadrenalism or render low glucocorticoid replacement doses ineffective (see Precautions).
In women on oral oestrogen replacement, a higher dose of growth hormone may be required to achieve the treatment goal (see Precautions).
Data from an interaction study performed in growth hormone deficient adults, suggests that somatropin administration may increase the clearance of compounds known to be metabolised by cytochrome P450 isoenzymes. The clearance of compounds metabolised by cytochrome P450 3A4 (e.g. sex steroids, corticosteroids, anticonvulsants and cyclosporine) may be especially increased resulting in lower plasma levels of these compounds. The clinical significance of this is unknown.
Incompatibilities: Solution for injection/Powder for injection 8 mg click.easy vial: In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Powder for injection 3.33 mg vial: In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products except those mentioned in Instructions for use/handling as previously mentioned.
Special precautions for disposal and other handling: Solution for injection: The cartridge containing the solution of Saizen Liquid is for use only with the easypod auto-injector or the aluetta pen injector. For storage of injectors containing a cartridge, see Storage.
The aluetta pen injectors and Saizen cartridges are available in several presentations. Each aluetta pen injector is colour coded and must only be used with the matching colour coded Saizen cartridge to give the correct dose. The aluetta pen injector 6 (blue) must be used with the cartridge containing 6 mg somatropin (blue). The aluetta pen injector 12 (red) must be used with the cartridge containing 12 mg somatropin (red). The aluetta pen injector 20 (yellow) must be used with the cartridge containing 20 mg somatropin (yellow). The solution for injection should be clear to slightly opalescent with no particles and without visible signs of deterioration. If the solution contains particles, it must not be injected.
Any unused product or waste material should be disposed of in accordance with local requirements.
Powder for injection 3.33 mg vial: To reconstitute Saizen, inject 5 ml of the bacteriostatic solvent into the vial of Saizen 3.33 mg aiming the liquid against the glass wall. Swirl the vial with a gentle rotary motion until the content is dissolved completely. Avoid vigorous shaking. Discard any unused solvent.
Benzyl alcohol as a preservative in bacteriostatic sodium chloride solution may cause toxic reactions and anaphylactoid reactions in infants and children up to 3 years old and must not be given to premature babies or neonates. Saizen may be reconstituted with Sodium Chloride Injection BP or Sterile Water for Injections for immediate use when administering to children under 3 years of age.
Any unused product or waste material should be disposed of in accordance with local requirements.
Powder for injection 8 mg click.easy vial: The cartridge containing the reconstituted solution of Saizen 8 mg click.easy is for use only with the one. click auto-injector, the cool.click needle-free autoinjectors, or the easypod auto-injector.
For storage of the auto-injectors containing the cartridge, see Storage. The reconstituted solution for injection should be clear with no particles. If the solution contains particles, it must not be injected.
Any unused product or waste material should be disposed of in accordance with local requirements.
Important information: Patients should be thoroughly instructed in the reconstitution procedure.
For young children, the reconstitution process should be supervised by an adult.
For administration of Saizen 8 mg click.easy please read the following instructions carefully.
When the medicine is injected into the same place every time for a long time, it can cause damage. It is important to keep changing the place where the patient has the injection. The doctor or pharmacist can speak about which part of the body the patient should use. Do not use any areas in which the patient feels lumps, firm knots, depressions, or pain; talk to the doctor or pharmacist about anything the patient finds. Clean the skin at the injection site with soap and water.
A separate leaflet gives the patient detailed instructions in pictures about how to use this reconstituted kits.
Please consult the doctor or pharmacist, if the patient has any questions concerning the reconstitution process.
How to prepare the solution of Saizen 8 mg click.easy: Make sure the click.easy is complete by checking that the Saizen vial, the sterile transfer cannula and the solvent cartridge are present.
Check that the tamper evident seals on the click.easy housing and on the cap are not broken. If either of the tamper evident seals are broken return it to the pharmacist or doctor.
Place all elements needed for the preparation of the solution on a clean surface.
Wash the hands with soap and water.
1. Place the click.easy reconstitution device vertically on a flat surface with the vial at the bottom and the cap facing upward.
2. Push the cap down until it will go no further. (Note: The tamper evident seal on the click.easy housing is now broken).
3. Turn slightly the cap clockwise until the green button is positioned in the vertical opening.
4. Continue pushing the cap down very slowly until it will go no further to transfer the solvent from the cartridge into the vial (Note: The tamper evident seal on the cap is now broken). It is important to push slowly to prevent foam to appear in the vial. Check that all the solvent has been transferred into the vial.
5. Dissolve the powder with the solvent by gently swirling the click.easy (Please note that the patient should not shake the solution strongly or the solution will foam). Avoid vigorous shaking to prevent creation of foam. Let the solution stand until the powder is completely dissolved. If the solution contains particles, it must not be injected. Push the cap back down until it will go no further and keep it in position.
6. Turn the click.easy so that the vial is at the top and pull the cap slowly downwards until the solution is completely drawn back into the cartridge.
Check that no more than one or two drops of solution remain in the vial.
If there are more than one or two drops of solution remaining in the vial, slowly push the cap up until some of the solution is back in the vial and gently tap the click.easy. Then draw the solution slowly again back into the cartridge.
7. Remove any excess air that has been drawn into the cartridge by pushing slowly the cap up until no air is visible in the cartridge.
(Note: Avoid pulling the cap down too fast, as this will draw air into the cartridge).
8. Keeping the click.easy in this position (vial on the top) unscrew the cap and remove it. Still keeping the same position (vial on the top) remove the cartridge containing the reconstituted solution for injection from the click.easy.
9. Carefully peel off the outer label using the tab provided.
Write the reconstitution date on the transparent inner label on the cartridge. Discard the click.easy safely in accordance with the local requirements.
The cartridge containing the reconstituted solution of Saizen is now ready to be used for administration with the one.click auto-injector, Easypod auto-injector or cool.click needle-free auto-injector.
The reconstituted solution for injection should be clear with no particles. If the solution contains particles, it must not be injected.
How to perform the daily self-administration of Saizen: For instructions on how to load the cartridge into the one.click auto-injector, Easypod auto-injector or how to use the cool.click needle-free auto-injector and inject the reconstituted solution of Saizen, please carefully read the corresponding instruction manual with each auto-injector. Use of the devices by children should always be made under adult's supervision.
Solution for injection: Store in the original package in order to protect from light. Store in a refrigerator (2°C-8°C). Do not freeze.
After first injection, store in a refrigerator (2°C-8°C) for a maximum of 28 days, of which up to 7 days, can be outside of a refrigerator at or below 25°C.
Powder for injection 3.33 mg vial: Store at 2°C to 8°C in the original package.
Store the reconstituted product at 2°C to 8°C in the original package.
Do not freeze.
Powder for injection 8 mg click.easy vial: Do not store above 30°C. Do not freeze. Store in the original package. Store the reconstituted product in a refrigerator (2°C to 8°C).
Shelf life: Solution for injection: 24 months.
Shelf life of the solution for injection in the opened cartridge: The ready-to-use solution for injection contains a preserving agent and must, from a microbiological point of view, be kept refrigerated (2°C-8°C) after the first injection and used within 28 days. Do not freeze. Any remaining amounts should be discarded after 28 days.
The easypod auto-injector or aluetta pen injector must be kept refrigerated (2°C-8°C) if it contains a cartridge.
Powder for injection 3.33 mg vial: 2 years.
The reconstituted solution for injection is stable for 14 days.
Powder for injection 8 mg click.easy vial: 3 years.
After reconstitution, the product may be stored for a maximum of 28 days in a refrigerator (2°C to 8°C).
H01AC01 - somatropin ; Belongs to the class of somatropin and somatropin agonists. Used in anterior pituitary lobe hormone and analogue preparations.
Saizen powd for inj (Clickeasy vial) 8 mg
1's
Saizen powd for inj (vial) 3.33 mg
1's
Saizen soln for inj 12 mg
1's
Saizen soln for inj 20 mg
1's
Saizen soln for inj 6 mg
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 8 mg94fd0f37-0685-4143-9827-a79f01085457.GIF)
 3.33 mg8ec04836-1820-4cff-811b-a79f0108546a.GIF)



 Sign Out
Sign Out
