


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of Action: Upadacitinib is a selective and reversible Janus Kinase (JAK) inhibitor. JAKs are intracellular enzymes that transmit cytokine or growth factor signals involved in a broad range of cellular processes including inflammatory responses, hematopoiesis and immune surveillance. The JAK family of enzymes contains four members, JAK1, JAK2, JAK3 and TYK2 which work in pairs to phosphorylate and activate signal transducers and activators of transcription (STATs). This phosphorylation, in turn, modulates gene expression and cellular function. JAK1 is important in inflammatory cytokine signals while JAK2 is important for red blood cell maturation and JAK3 signals play a role in immune surveillance and lymphocyte function.
In human cellular assays, upadacitinib preferentially inhibits signalling by JAK1 or JAK1/3 with functional selectivity over cytokine receptors that signal via pairs of JAK2. Atopic dermatitis is driven by pro-inflammatory cytokines (including IL-4, IL-13, IL-22, TSLP, IL-31 and IFN-γ) that transduce signals via the JAK1 pathway. Inhibiting JAK1 with upadacitinib reduces the signaling of many mediators which drive the signs and symptoms of atopic dermatitis such as eczematous skin lesions and pruritus.
Pharmacodynamic effects: Inhibition of IL-6 Induced STAT3 and IL-7 Induced STAT5 Phosphorylation: In healthy volunteers, the administration of upadacitinib (immediate release formulation) resulted in a dose- and concentration-dependent inhibition of IL-6 (JAK1/JAK2)-induced STAT3 and IL-7 (JAK1/JAK3)-induced STAT5 phosphorylation in whole blood. The maximal inhibition was observed 1 hour after dosing which returned to near baseline by the end of dosing interval.
Lymphocytes: In patients with rheumatoid arthritis, treatment with upadacitinib was associated with a small, transient increase in mean ALC from baseline up to Week 36 which gradually returned to at or near baseline levels with continued treatment.
hsCRP: In patients with rheumatoid arthritis, treatment with upadacitinib was associated with decreases from baseline in mean hsCRP levels as early as Week 1 which were maintained with continued treatment.
Vaccine Study: The influence of upadacitinib on the humoral response following the administration of inactivated pneumococcal polysaccharide conjugate vaccine (13-valent, adsorbed) was evaluated in 111 patients with rheumatoid arthritis under stable treatment with upadacitinib 15 mg (n=87) or 30 mg (n=24). 97% of patients (n=108) were on concomitant methotrexate. The primary endpoint was the proportion of patients with satisfactory humoral response defined as ≥2-fold increase in antibody concentration from baseline to Week 4 in at least 6 out of the 12 pneumococcal antigens (1, 3, 4, 5, 6B, 7F, 9V, 14, 18C, 19A, 19F, and 23F). Results at Week 4 demonstrated a satisfactory humoral response in 67.5% (95% CI: 57.4, 77.5) and 56.5% (95% CI: 36.3, 76.8) of patients treated with upadacitinib 15 mg and 30 mg, respectively.
Clinical efficacy and safety: Rheumatoid arthritis: The efficacy and safety of upadacitinib 15 mg once daily was assessed in five Phase 3 randomised, double-blind, multicentre studies in patients with moderately to severely active rheumatoid arthritis and fulfilling the ACR/EULAR 2010 classification criteria (see Table 1). Patients 18 years of age and older were eligible to participate. The presence of at least 6 tender and 6 swollen joints and evidence of systemic inflammation based on elevation of hsCRP was required at baseline. Four studies included long-term extensions for up to 5 years, and one study (SELECT-COMPARE) included a long-term extension for up to 10 years.
The primary analysis for each of these studies included all randomised subjects who received at least 1 dose of upadacitinib or placebo drug, and non-responder imputation was used for categorical endpoints.
Across the Phase 3 studies, the efficacy seen with upadacitinib 15 mg QD was generally similar to that observed with upadacitinib 30 mg QD. (See Table 1.)
 Click on icon to see table/diagram/image
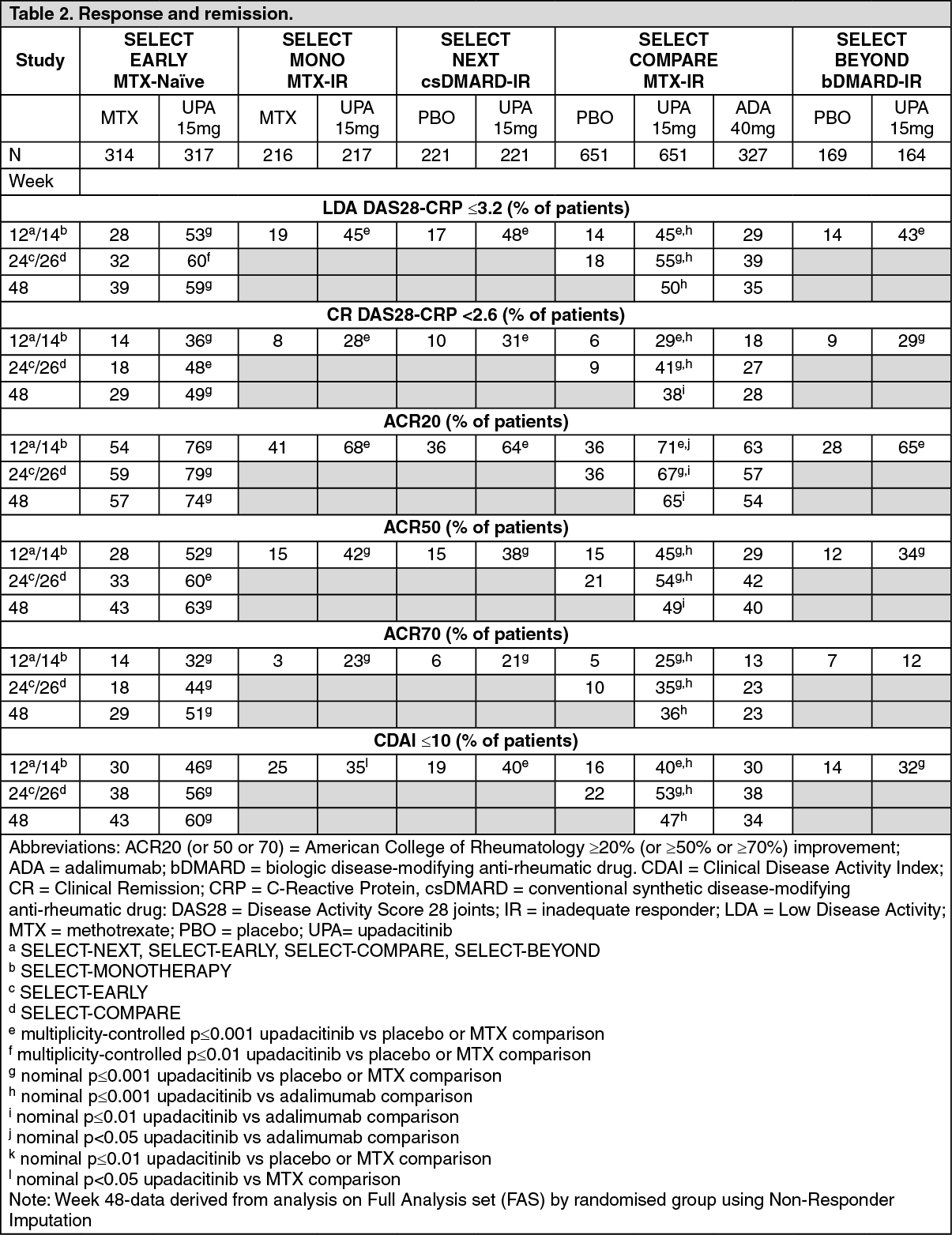
Click on icon to see table/diagram/imageClinical Response: Remission and low disease activity: In the studies, a significantly higher proportion of patients treated with upadacitinib 15 mg achieved low disease activity (DAS28-CRP ≤3.2) and clinical remission (DAS28-CRP <2.6) compared to placebo, MTX or adalimumab (Table 2). Compared to adalimumab, significantly higher rates of low disease activity were achieved at week 12 in SELECT-COMPARE. Overall, both low disease activity and clinical remission rates were consistent across patient populations, with or without MTX. At 3 years, 297/651 (45.6%) and 111/327 (33.9%) patients remained on originally randomised treatment of upadacitinib 15 mg or adalimumab, respectively, in SELECT-COMPARE, and 216/317 (68.1%) and 149/315 (47.3%) patients remained on originally randomised treatment of upadacitinib 15 mg or MTX monotherapy, respectively, in SELECT-EARLY. Among the patients who remained on their originally allocated treatment, low disease activity and clinical remission were maintained through 3 years.
ACR Response: In all studies, more patients treated with upadacitinib 15 mg achieved ACR20, ACR50, and ACR70 responses at 12 weeks compared to placebo, MTX, or adalimumab (Table 2). Time to onset of efficacy was rapid across measures with greater responses seen as early as week 1 for ACR20. Durable response rates were observed (with or without MTX), with ACR20/50/70 responses maintained through 3 years among the patients who remained on their originally allocated treatment.
Treatment with upadacitinib 15 mg, alone or in combination with csDMARDs, resulted in improvements in individual ACR components, including tender and swollen joint counts, patient and physician global assessments, HAQ-DI, pain assessment and hsCRP. (See Table 2.)
 Click on icon to see table/diagram/image
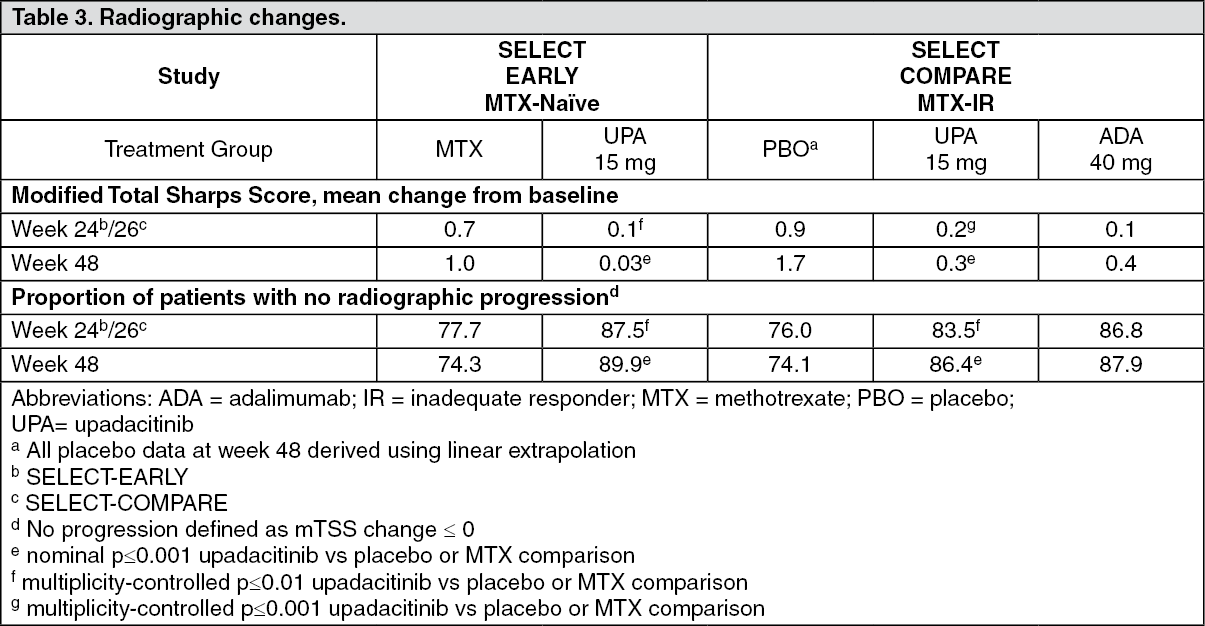
Click on icon to see table/diagram/imageRadiographic Response: Inhibition of progression of structural joint damage was assessed using the modified Total Sharp Score (mTSS) and its components, the erosion score and joint space narrowing score, at weeks 24/26 and week 48 in SELECT-EARLY and SELECT-COMPARE.
Treatment with upadacitinib 15 mg resulted in significantly greater inhibition of the progression of structural joint damage compared to placebo in combination with MTX in SELECT-COMPARE and as monotherapy compared to MTX in SELECT-EARLY (Table 3). Analyses of erosion and joint space narrowing scores were consistent with the overall scores. The proportion of patients with no radiographic progression (mTSS change ≤ 0) was significantly higher with upadacitinib 15 mg in both studies. Inhibition of progression of structural joint damage was maintained through Week 96 in both studies for patients who remained on their originally allocated treatment with upadacitinib 15 mg (based on available results from 327 patients in SELECT-COMPARE and 238 patients in SELECT-EARLY). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePhysical Function Response and Health-Related Outcomes: Treatment with upadacitinib 15 mg, alone or in combination with csDMARDs, resulted in a significantly greater improvement in physical function compared to all comparators as measured by HAQ-DI (see Table 4).
Improvements in HAQ-DI and pain were maintained through 3 years for patients who remained on their originally allocated treatment with upadacitinib 15 mg based on available results from SELECT-COMPARE and SELECT-EARLY. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the studies SELECT-MONOTHERAPY, SELECT-NEXT, and SELECT-COMPARE, treatment with upadacitinib 15 mg resulted in a significantly greater improvement in the mean duration of morning joint stiffness compared to placebo or MTX.
In the clinical studies, upadacitinib treated patients reported significant improvements in patient-reported quality of life, as measured by the Short Form (36) Health Survey (SF-36) Physical Component Score compared to placebo and MTX. Moreover, upadacitinib treated patients reported significant improvements in fatigue, as measured by the Functional Assessment of Chronic Illness Therapy-Fatigue score (FACIT-F) compared to placebo.
Psoriatic arthritis: The efficacy and safety of upadacitinib 15 mg once daily were assessed in two Phase 3 randomised, double-blind, multicenter, placebo-controlled studies in patients 18 years of age or older with moderately to severely active psoriatic arthritis. All patients had active psoriatic arthritis for at least 6 months based upon the Classification Criteria for Psoriatic Arthritis (CASPAR), at least 3 tender joints and at least 3 swollen joints, and active plaque psoriasis or history of plaque psoriasis. For both studies, the primary endpoint was the proportion of patients who achieved an ACR20 response at week 12.
SELECT-PsA 1 was a 24-week trial in 1705 patients who had an inadequate response or intolerance to at least one non-biologic DMARD. At baseline, 1393 (82%) of patients were on at least one concomitant non-biologic DMARD; 1084 (64%) of patients received concomitant MTX only; and 311 (18%) of patients were on monotherapy. Patients received upadacitinib 15 mg or 30 mg once daily, adalimumab, or placebo. At week 24, all patients randomised to placebo were switched to upadacitinib 15 mg or 30 mg once daily in a blinded manner. SELECT-PsA 1 included a long-term extension for up to 5 years.
SELECT-PsA 2 was a 24-week trial in 642 patients who had an inadequate response or intolerance to at least one biologic DMARD. At baseline, 296 (46%) of patients were on at least one concomitant non-biologic DMARD; 222 (35%) of patients received concomitant MTX only; and 345 (54%) of patients were on monotherapy. Patients received upadacitinib 15 mg or 30 mg once daily or placebo. At week 24, all patients randomised to placebo were switched to upadacitinib 15 mg or 30 mg once daily in a blinded manner. SELECT-PsA 2 included a long-term extension for up to 3 years.
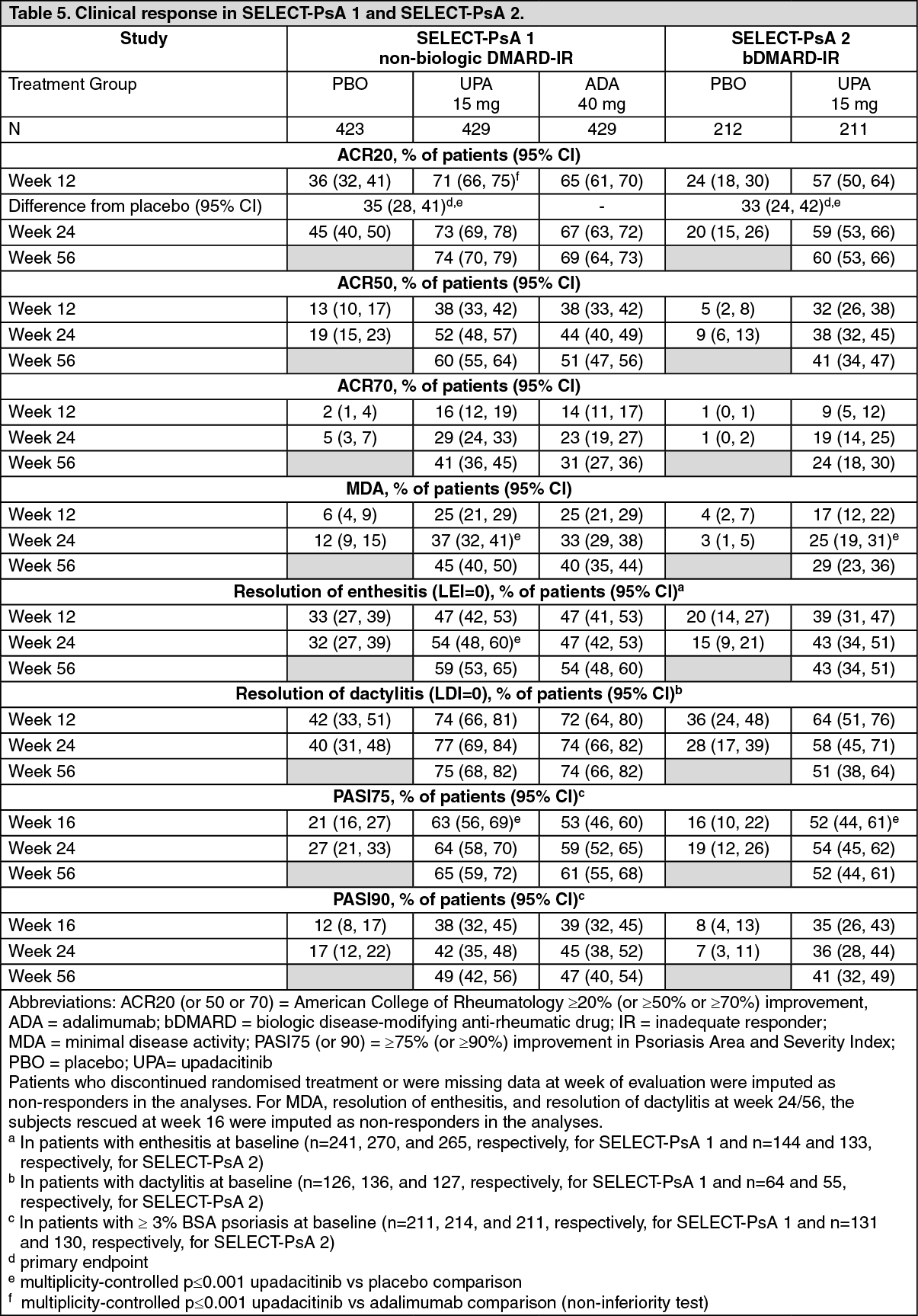
Clinical response: In both studies, a statistically significant greater proportion of patients treated with upadacitinib 15 mg achieved ACR20 response compared to placebo at week 12 (Table 5). Time to onset of efficacy was rapid across measures with greater responses seen as early as week 2 for ACR20.
Treatment with upadacitinib 15 mg resulted in improvements in individual ACR components, including tender/painful and swollen joint counts, patient and physician global assessments, HAQ-DI, pain assessment, and hsCRP compared to placebo.
In SELECT-PsA 1, upadacitinib 15 mg achieved non-inferiority compared to adalimumab in the proportion of patients achieving ACR20 response at week 12; however, superiority to adalimumab could not be demonstrated.
In both studies, consistent responses were observed alone or in combination with methotrexate for primary and key secondary endpoints.
The efficacy of upadacitinib 15 mg was demonstrated regardless of subgroups evaluated including baseline BMI, baseline hsCRP, and number of prior non-biologic DMARDs (≤1 or >1). (See Table 5.)
 Click on icon to see table/diagram/image
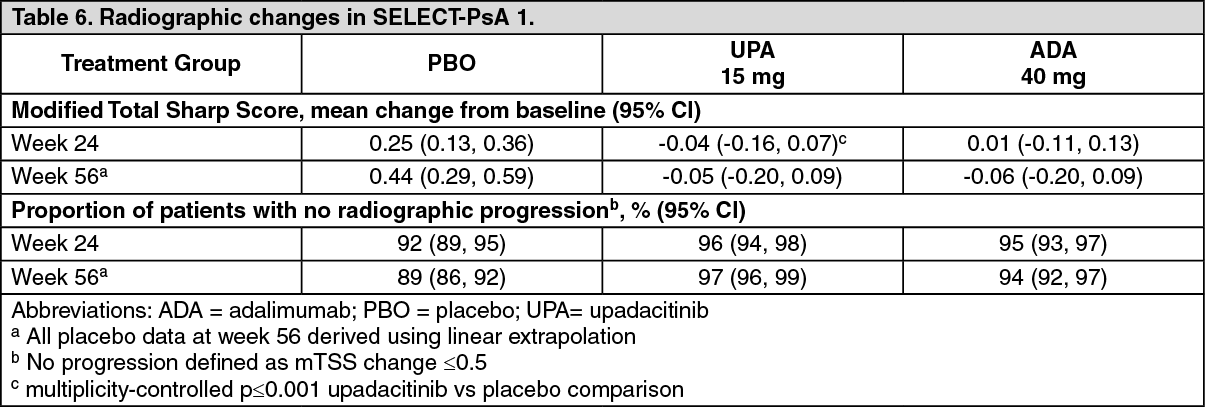
Click on icon to see table/diagram/imageRadiographic response: In SELECT-PsA 1, inhibition of progression of structural damage was assessed radiographically and expressed as the change from baseline in modified Total Sharp Score (mTSS) and its components, the erosion score and the joint space narrowing score, at week 24.
Treatment with upadacitinib 15 mg resulted in statistically significant greater inhibition of the progression of structural joint damage compared to placebo at week 24 (Table 6). Erosion and joint space narrowing scores were consistent with the overall scores. The proportion of patients with no radiographic progression (mTSS change ≤ 0.5) was higher with upadacitinib 15 mg compared to placebo at week 24. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePhysical function response and health-related outcomes: In SELECT-PsA 1, patients treated with upadacitinib 15 mg showed statistically significant improvement from baseline in physical function as assessed by HAQ-DI at week 12 (-0.42 [95% CI: -0.47, -0.37]) compared to placebo (-0.14 [95% CI: -0.18, -0.09]); improvement in patients treated with adalimumab was -0.34 (95% CI: -0.38, -0.29). In SELECT-PsA 2, patients treated with upadacitinib 15 mg showed statistically significant improvement from baseline in HAQ-DI at week 12 (-0.30 [95% CI: -0.37, -0.24]) compared to placebo (-0.10 [95% CI: -0.16, -0.03]). Improvement in physical function was maintained through week 56 in both studies.
Health-related quality of life was assessed by SF-36v2. In both studies, patients receiving upadacitinib 15 mg experienced statistically significant greater improvement from baseline in the Physical Component Summary score compared to placebo at week 12. Improvements from baseline were maintained through week 56 in both studies.
Patients receiving upadacitinib 15 mg experienced statistically significant improvement from baseline in fatigue, as measured by FACIT-F score, at week 12 compared to placebo in both studies. Improvements from baseline were maintained through week 56 in both studies.
At baseline, psoriatic spondylitis was reported in 31% and 34% of patients in SELECT-PsA 1 and SELECT-PsA 2, respectively. Patients with psoriatic spondylitis treated with upadacitinib 15 mg showed improvements from baseline in Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores compared to placebo at week 24. Improvements from baseline were maintained through week 56 in both studies.
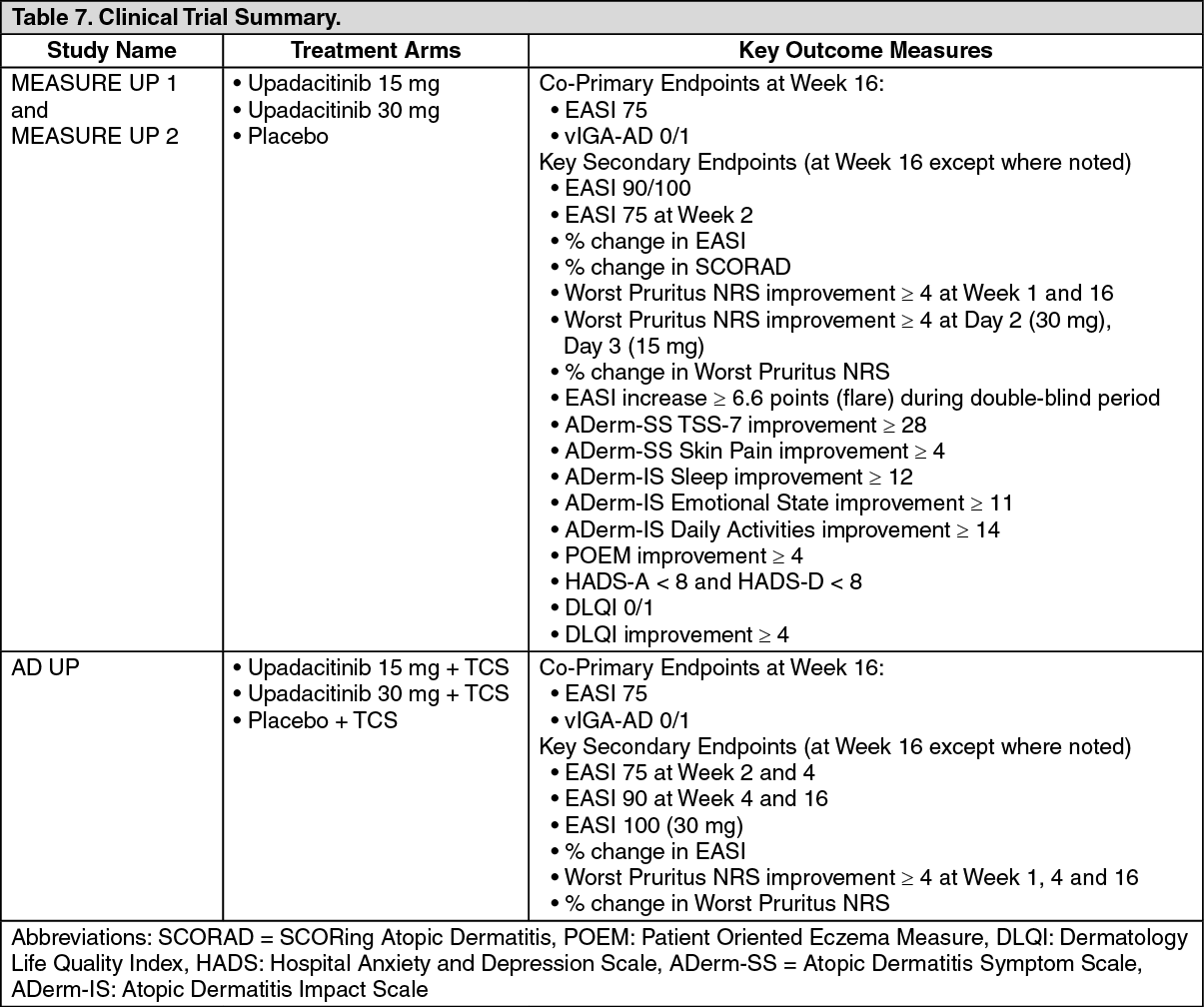
Atopic dermatitis: The efficacy and safety of upadacitinib 15 mg and 30 mg once daily was assessed in three Phase 3 randomized, double-blind, multicenter studies (MEASURE UP 1, MEASURE UP 2 and AD UP) in a total of 2584 patients 12 years of age and older (Table 7). Upadacitinib was evaluated in 344 adolescent and 2240 adult patients with moderate to severe atopic dermatitis (AD) not adequately controlled by topical medication(s). At baseline, patients had to have all the following: an Investigator's Global Assessment (vIGA-AD) score ≥3 in the overall assessment of AD (erythema, induration/papulation, and oozing/crusting) on an increasing severity scale of 0 to 4, an Eczema Area and Severity Index (EASI) score ≥16 (composite score assessing extent and severity of erythema, oedema/papulation, scratches and lichenification across 4 different body sites), a minimum body surface area (BSA) involvement of ≥10%, and weekly average Worst Pruritus Numerical Rating Scale (NRS) ≥4.
In all three studies, patients received upadacitinib once daily doses of 15 mg, 30 mg or matching placebo for 16 weeks. In the AD UP study, patients also received concomitant topical corticosteroids (TCS). Following completion of the double-blinded period, patients originally randomized to upadacitinib were to continue receiving the same dose until week 260. Patients in the placebo group were re-randomized in a 1:1 ratio to receive upadacitinib 15 mg or 30 mg until week 260. (See Table 7.)
 Click on icon to see table/diagram/image
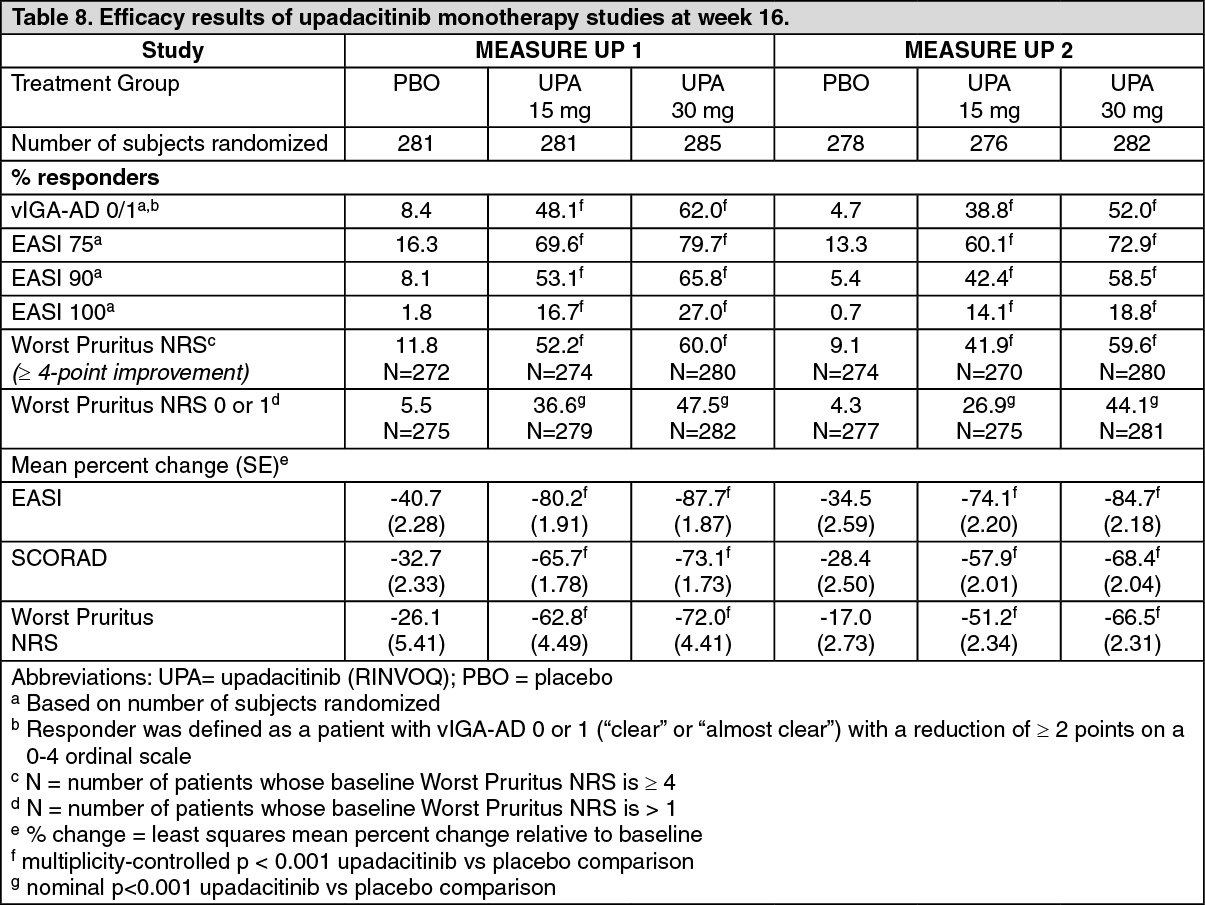
Click on icon to see table/diagram/imageClinical Response: Monotherapy Studies (MEASURE UP 1 AND MEASURE UP 2): In the MEASURE UP studies, a significantly greater proportion of patients treated with upadacitinib 15 mg or 30 mg achieved vIGA-AD 0 or 1 response and achieved EASI 75 compared to placebo at week 16 (Table 8). A rapid improvement in skin clearance (defined as EASI 75 by week 2) was achieved for both doses compared to placebo (p < 0.001).
A significantly greater proportion of patients treated with upadacitinib 15 mg or 30 mg achieved clinically meaningful improvement in itch (defined as a ≥4-point reduction in the Worst Pruritus NRS) compared to placebo at week 16. Rapid improvement in itch (defined as a ≥4-point reduction in Worst Pruritus NRS by week 1) was achieved for both doses compared to placebo (p < 0.001), with differences observed as early as 1 day after initiating upadacitinib 30 mg (Day 2, p < 0.001) and 2 days after initiating upadacitinib 15 mg (Day 3, p < 0.001).
A significantly smaller proportion of patients treated with upadacitinib 15 mg or 30 mg had a disease flare, defined as a clinically meaningful worsening of disease (increase in EASI by ≥6.6), during the initial 16 weeks of treatment compared to placebo (p < 0.001).
Figure 1 and Figure 2 show proportion of patients achieving an EASI 75 response and the proportion of patients with ≥4-point improvement in the Worst Pruritus NRS, respectively up to week 16. (See Table 8, Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image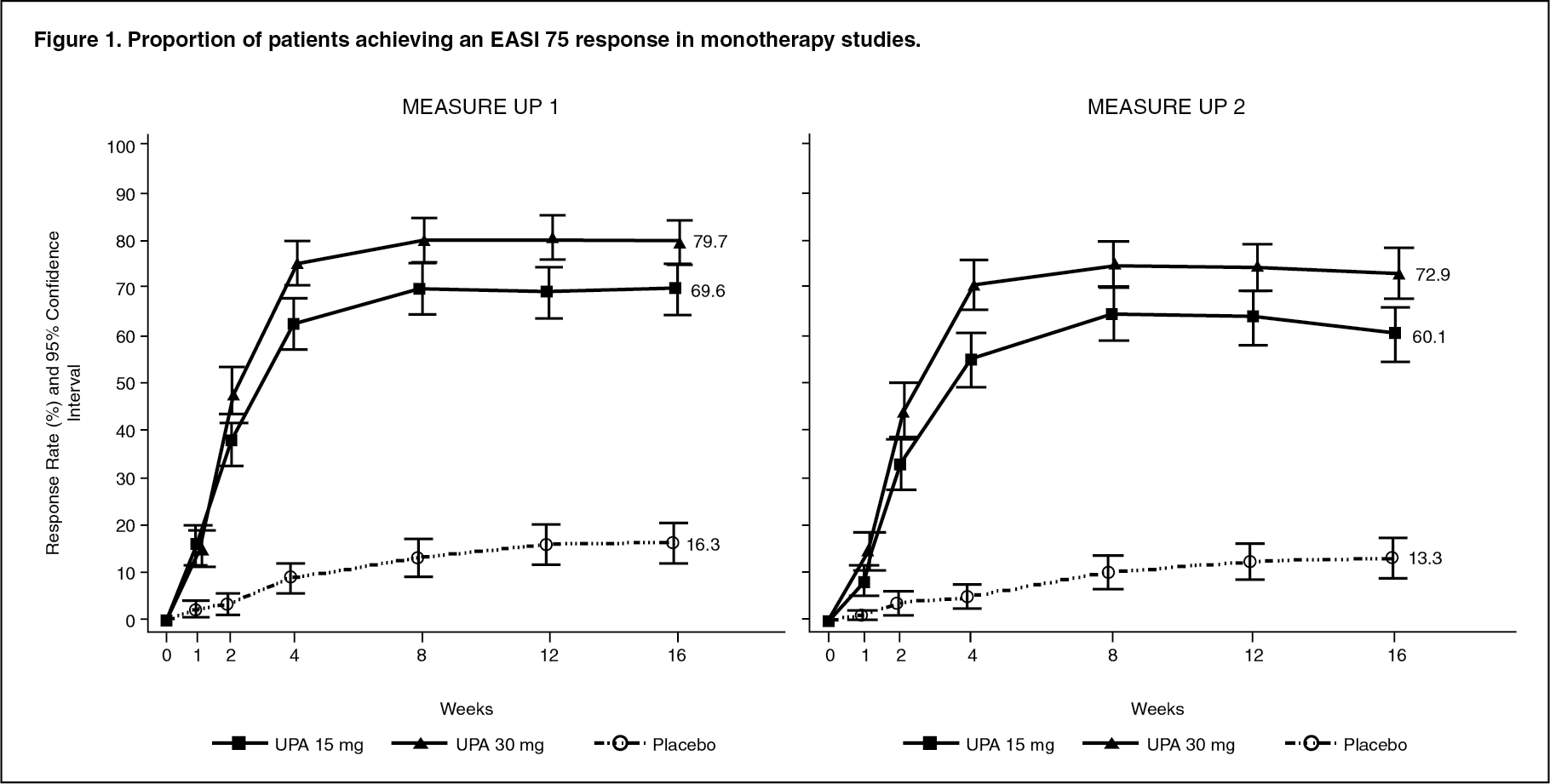 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image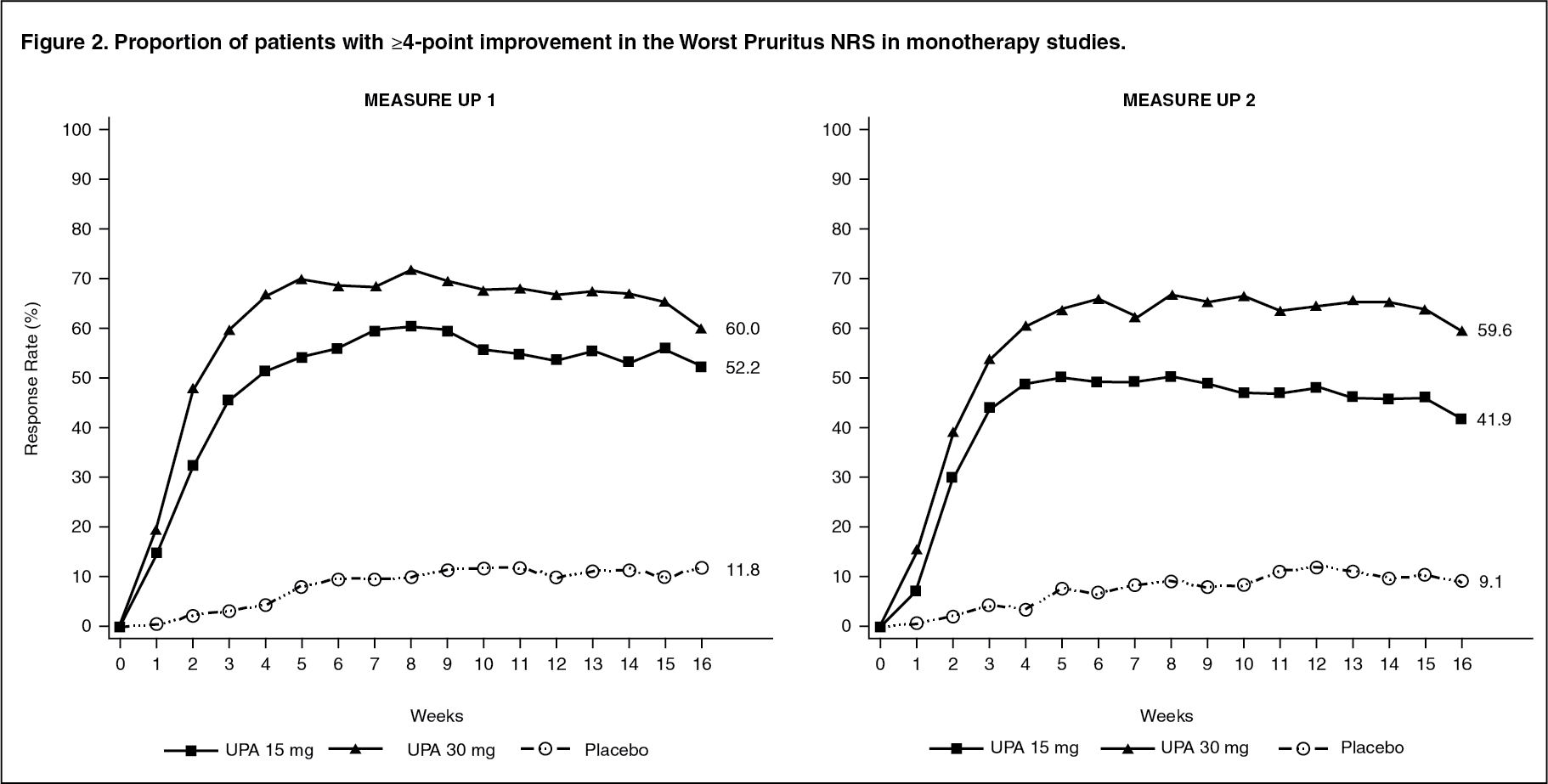 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn both studies, results at week 16 continued to be observed through week 52 in patients treated with upadacitinib 15 mg or 30 mg.
Treatment effects in subgroups (weight, age, gender, race, and prior systemic treatment with immunosuppressants) in both studies were consistent with the results in the overall study population.
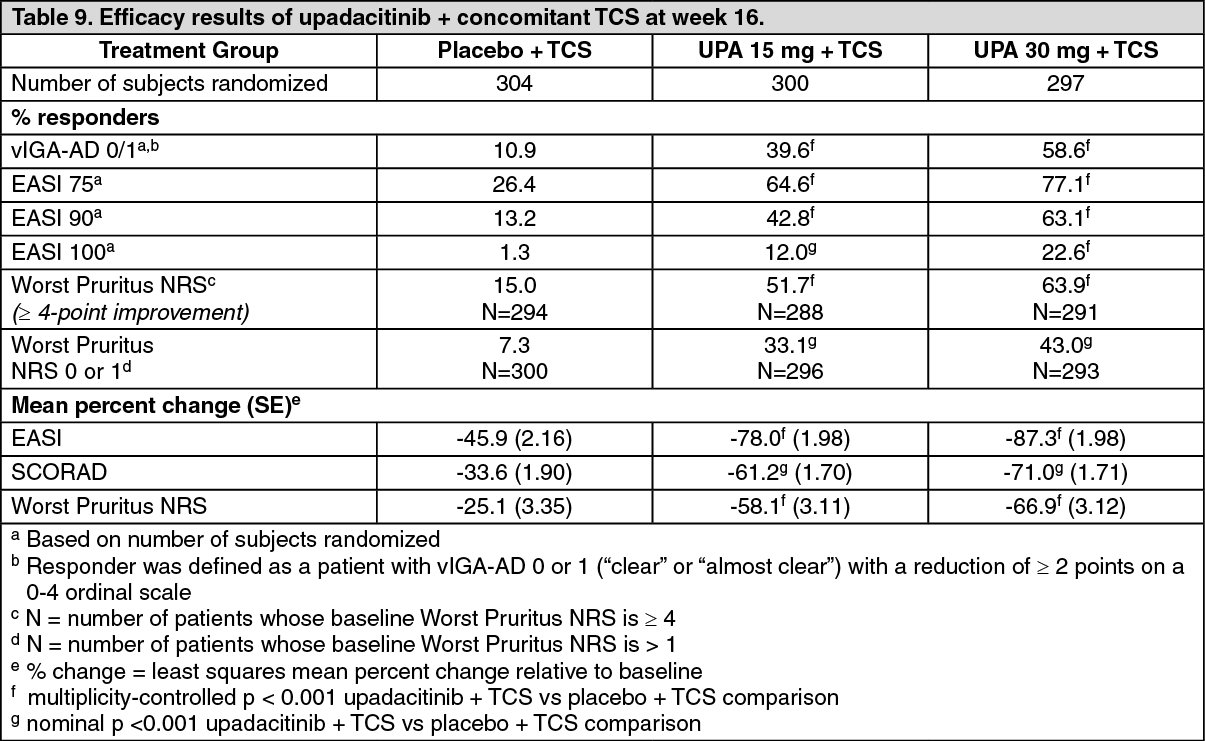
Concomitant TCS Study (AD UP): In AD UP, a significantly greater proportion of patients treated with upadacitinib 15 mg + TCS or 30 mg + TCS achieved vIGA-AD 0 or 1 response and achieved EASI 75 compared to placebo + TCS at week 16 (Table 9). A rapid improvement in skin clearance (defined as EASI 75 by week 2) was achieved for both doses compared to placebo + TCS (p < 0.001). In addition, a higher EASI 90 response rate was achieved at week 4 for both doses compared to placebo + TCS (p < 0.001).
A significantly greater proportion of patients treated with upadacitinib 15 mg + TCS or 30 mg + TCS achieved a clinically meaningful improvement in itch (defined as a ≥4-point reduction in the Worst Pruritus NRS) compared to placebo + TCS at week 16. A rapid improvement in itch (defined as a ≥4-point reduction in Worst Pruritus NRS by week 1) was achieved for both doses compared to placebo + TCS (p < 0.001).
Figure 3 and Figure 4 show proportion of patients achieving an EASI 75 response and the proportion of patients with ≥4-point improvement in the Worst Pruritus NRS, respectively up to week 16. (See Table 9, Figures 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image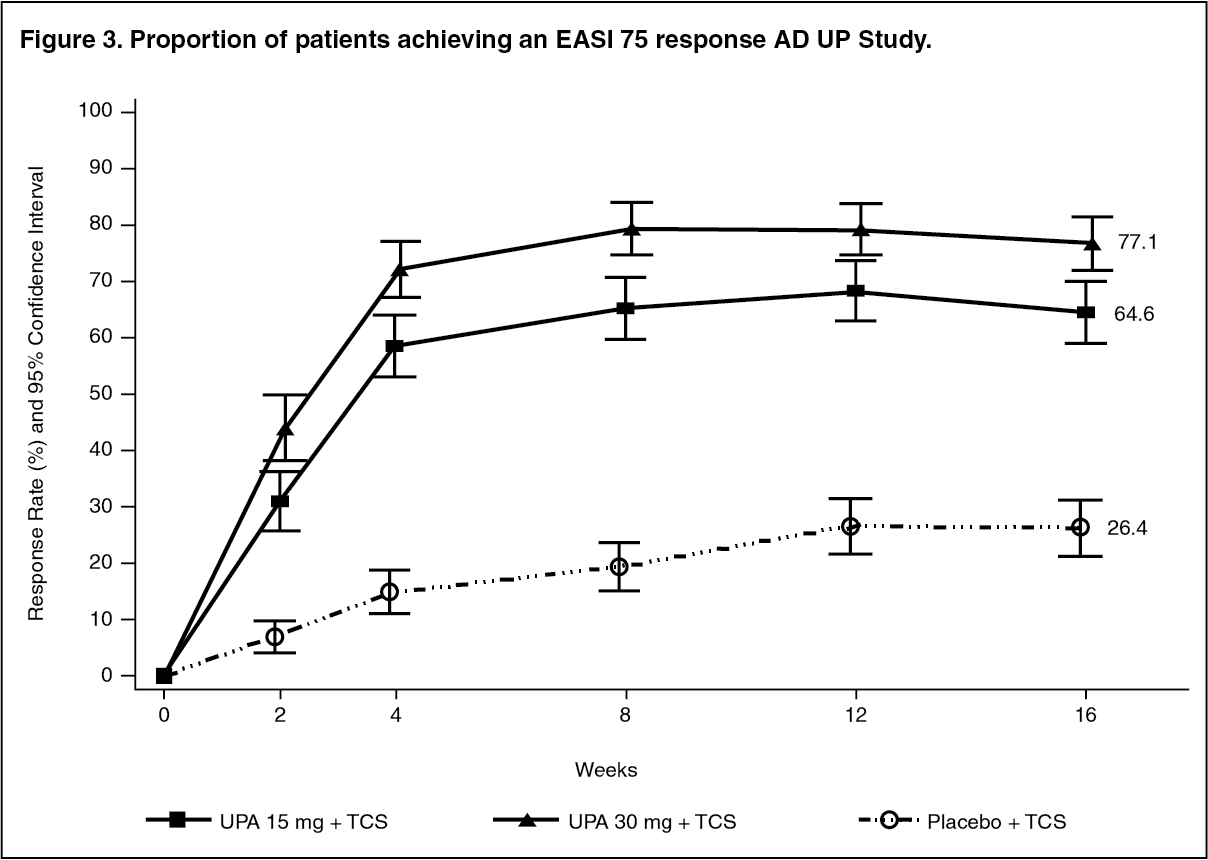 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image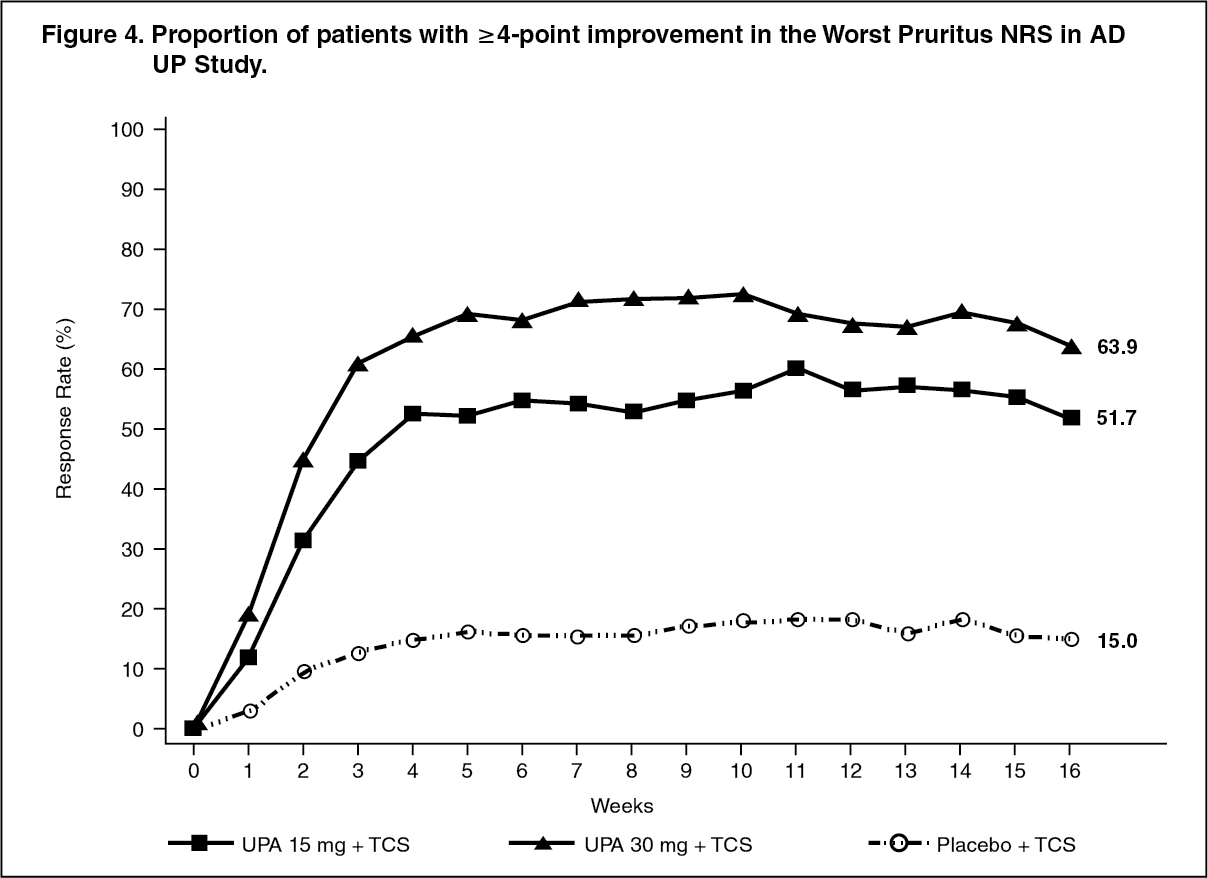 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment effects in subgroups (weight, age, gender, race, and prior systemic treatment with immunosuppressants) in AD UP were consistent with the results in the overall study population.
Subjects treated with either upadacitinib 15 mg or 30 mg had significantly more days free of TCS use with a concurrent EASI 75 response (mean: 33.5 and 47.5 days, respectively) over the 16-week period, compared to placebo group (mean: 7.9 days).
Results at week 16 continued to be observed through week 52 in patients treated with upadacitinib 15 mg or 30 mg.
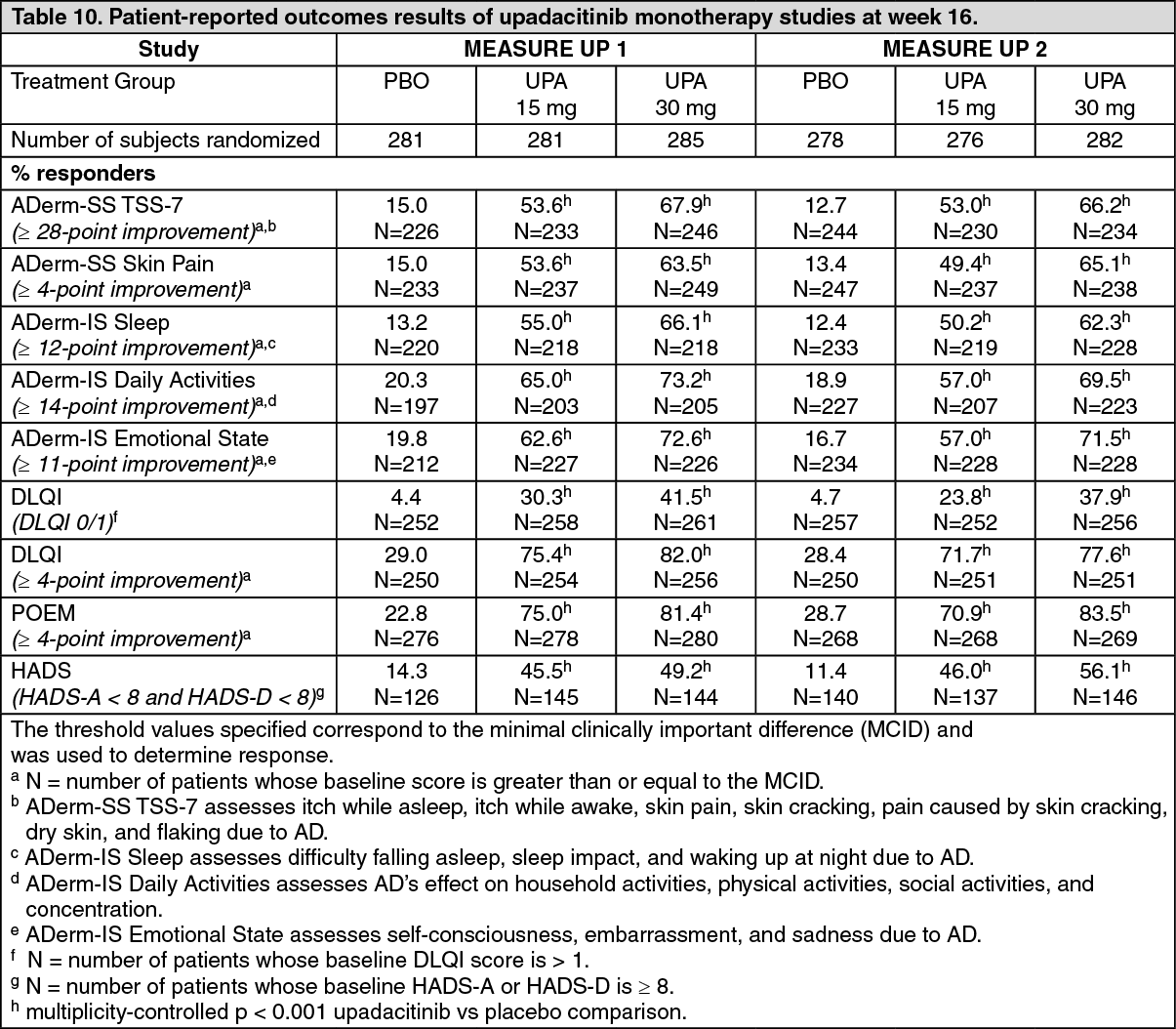
Quality of Life/Patient reported outcomes: In the MEASURE UP studies, a significantly greater proportion of patients treated with upadacitinib 15 mg or 30 mg reported clinically meaningful reductions in the symptoms of AD and the impact of AD on health-related quality of life compared to placebo at week 16 (Table 10). A significantly greater proportion of patients treated with upadacitinib achieved clinically meaningful reductions in AD symptom severity as measured by ADerm-SS TSS-7 and ADerm-SS Skin Pain compared to placebo at week 16. A greater proportion of patients treated with upadacitinib achieved clinically meaningful reductions in the patient-reported effects of AD on sleep, daily activities and emotional state as measured by the ADerm-IS domain scores compared to placebo at week 16. Similarly, compared to placebo at week 16, a greater proportion of patients treated with upadacitinib achieved clinically meaningful improvements in AD symptom frequency and health-related quality of life as measured by the POEM and DLQI.
Anxiety and depression symptoms as measured by the HADS score were significantly reduced; in patients with baseline HADS-anxiety or HADS-depression subscale scores ≥8 (the cut-off value for anxiety or depression), a greater proportion of patients in the upadacitinib 15 mg or 30 mg groups achieved HADS-anxiety and HADS-depression scores <8 at week 16 compared to placebo (Table 10). (See Table 10.)
 Click on icon to see table/diagram/image
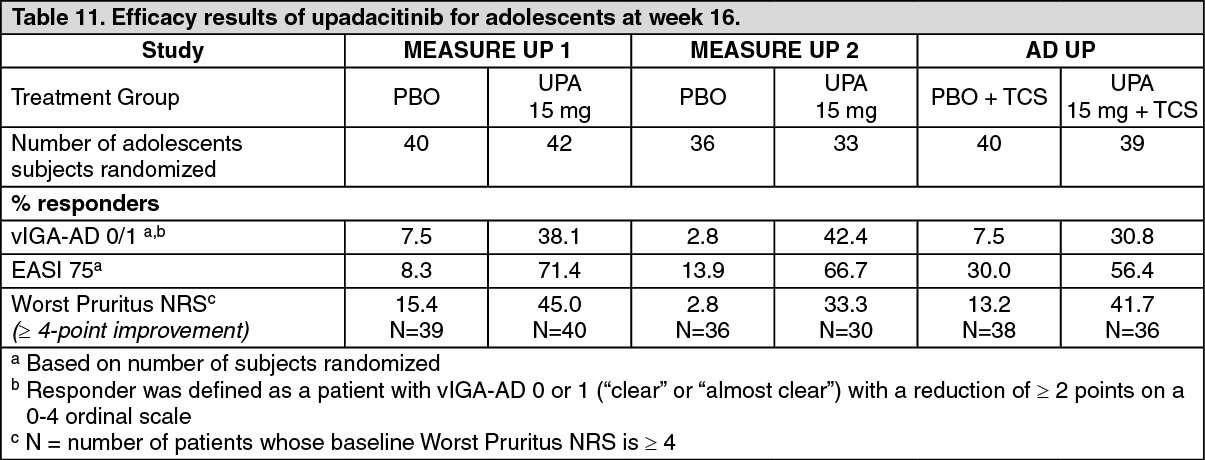
Click on icon to see table/diagram/imagePaediatric population: A total of 344 adolescents aged 12 to 17 years with moderate to severe atopic dermatitis were randomized across the three Phase 3 studies to receive either 15 mg (N=114) or 30 mg (N=114) upadacitinib or matching placebo (N=116), in monotherapy or combination with topical corticosteroids. Efficacy was consistent between the adolescents and adults (Table 11). The adverse event profile in adolescents was generally similar to that in adults. Safety and efficacy of upadacitinib in adolescents weighing less than 40 kg and in patients less than 12 years of age with atopic dermatitis have not been established. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe European Medicines Agency has deferred the obligation to submit the results of studies with RINVOQ in one or more subsets of the paediatric population in chronic idiopathic arthritis (including rheumatoid arthritis, psoriatic arthritis, spondyloarthritis, juvenile idiopathic arthritis and atopic dermatitis) (see Dosage & Administration for information on paediatric use).
Ankylosing Spondylitis (AS, radiographic axial spondyloarthritis): The efficacy and safety of RINVOQ 15 mg once daily were assessed in two randomised, double-blind, multicentre, placebo-controlled studies in patients 18 years of age or older with active ankylosing spondylitis based upon the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥4 and Patient's Assessment of Total Back Pain score ≥4. Both studies included long-term extensions for up to 2 years.
SELECT-AXIS 1 was a 14-week placebo-controlled trial in 187 ankylosing spondylitis patients with an inadequate response to at least two NSAIDs or intolerance to or contraindication for NSAIDs and had no previous exposure to biologic DMARDs. At baseline, patients had symptoms of ankylosing spondylitis for an average of 14.4 years and approximately 16% of the patients were on a concomitant csDMARD. Patients received upadacitinib 15 mg once daily or placebo. At week 14, all patients randomised to placebo were switched to upadacitinib 15 mg once daily. The primary endpoint was the proportion of patients achieving an Assessment of SpondylArthritis international Society 40 (ASAS40) response at week 14.
SELECT-AXIS 2 (AS) was a 14-week placebo-controlled trial in 420 ankylosing spondylitis patients with prior exposure to bDMARDs (77.4% had lack of efficacy to either a tumour necrosis factor (TNF) blocker or interleukin-17 inhibitor (IL-17i); 30.2% had intolerance; 12.9% had prior exposure but not lack of efficacy to two bDMARDs). At baseline, patients had symptoms of ankylosing spondylitis for an average of 12.8 years and approximately 31% of the patients were on a concomitant csDMARD. Patients received upadacitinib 15 mg once daily or placebo. At week 14, all patients randomised to placebo were switched to upadacitinib 15 mg once daily. The primary endpoint was the proportion of patients achieving an Assessment of SpondylArthritis international Society 40 (ASAS40) response at week 14.
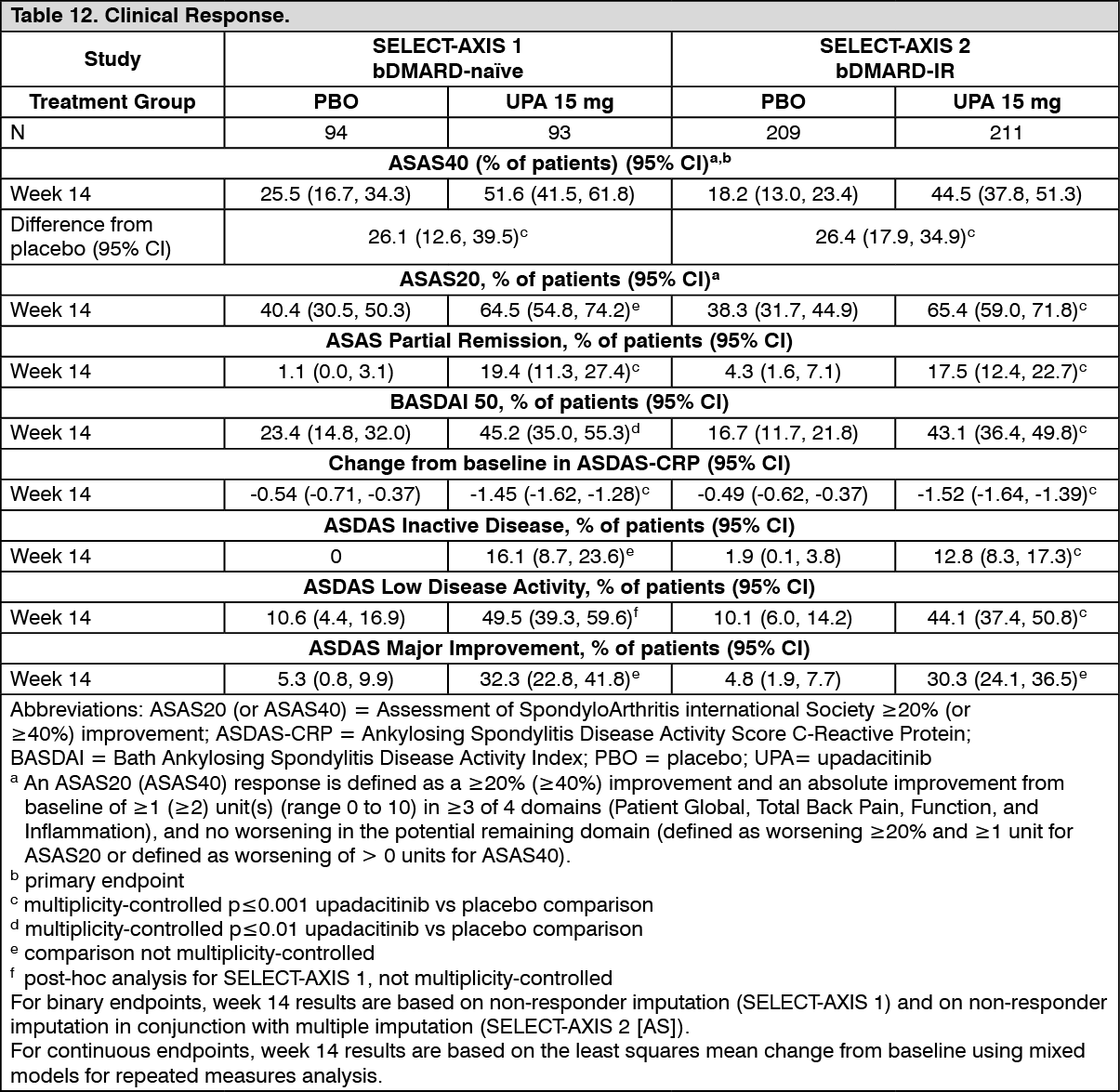
Clinical Response: In both studies, a significantly greater proportion of patients treated with RINVOQ 15 mg achieved an ASAS40 response compared to placebo at Week 14 (Table 12). A numerical difference between treatment groups was observed from week 2 in SELECT-AXIS 1 and week 4 in SELECT-AXIS 2 (AS) for ASAS40.
Treatment with RINVOQ 15 mg resulted in improvements in individual ASAS components, (patient global assessment of disease activity, total back pain assessment, inflammation, and function) and other measures of disease activity, including hsCRP, at week 14 compared to placebo.
The efficacy of upadacitinib 15 mg was demonstrated regardless of subgroups evaluated including gender, baseline BMI, symptom duration of AS, baseline hsCRP, and prior use of bDMARDs. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn SELECT-AXIS 1, efficacy was maintained through 2 years as assessed by the endpoints presented in Table 12.
Physical Function Response and Health-Related Outcomes: In both studies, patients treated with RINVOQ 15 mg showed significant improvement in physical function from baseline compared to placebo as assessed by the Bath Ankylosing Spondylitis Functional Index (BASFI) change from baseline at week 14. In SELECT-AXIS 1, improvement in BASFI was maintained through 2 years.
In SELECT-AXIS 2 (AS), patients treated with RINVOQ 15 mg showed significant improvements in total back pain and nocturnal back pain compared to placebo at Week 14.
In SELECT-AXIS 2 (AS), patients treated with RINVOQ 15 mg showed significant improvements in health-related quality of life and overall health as measured by ASQoL and ASAS Health Index, respectively, compared to placebo at Week 14.
Enthesitis: In SELECT-AXIS 2, patients with pre-existing enthesitis (n=310) treated with RINVOQ 15 mg showed significant improvement in enthesitis compared to placebo as measured by change from baseline in Maastricht Ankylosing Spondylitis Enthesitis Score (MASES) at week 14.
Spinal mobility: In SELECT-AXIS 2 (AS), patients treated with RINVOQ 15 mg showed significant improvement in spinal mobility compared to placebo as measured by change from baseline in Bath Ankylosing Spondylitis Metrology Index (BASMI) at Week 14.
Objective Measures of Inflammation: Signs of inflammation were assessed by MRI and expressed as change from baseline in the SPARCC score for spine and sacroiliac joints. In both studies, at Week 14, significant improvement of inflammatory signs in the spine was observed in patients treated with RINVOQ 15 mg compared to placebo. In SELECT-AXIS 1, improvement in inflammation as assessed by MRI was maintained through 2 years.
Pharmacokinetics: Upadacitinib plasma exposures are proportional to dose over the therapeutic dose range. Steady-state plasma concentrations are achieved within 4 days with minimal accumulation after multiple once-daily administrations.
Absorption: Following oral administration of upadacitinib extended-release formulation, upadacitinib is absorbed with a median Tmax of 2 to 4 hours. Coadministration of upadacitinib with a high-fat meal had no clinically relevant effect on upadacitinib exposures (increased AUC by 29% and Cmax by 39%). In clinical trials, upadacitinib was administered without regard to meals (see Dosage & Administration). In vitro, upadacitinib is a substrate for the efflux transporters P-gp and BCRP.
Distribution: Upadacitinib is 52% bound to plasma proteins. Upadacitinib partitions similarly between plasma and blood cellular components, as indicated by the blood to plasma ratio of 1.0.
Metabolism: Upadacitinib metabolism is mediated by CYP3A4 with a potential minor contribution from CYP2D6. The pharmacologic activity of upadacitinib is attributed to the parent molecule. In a human radiolabeled study, unchanged upadacitinib accounted for 79% of the total radioactivity in plasma while the main metabolite (product of monooxidation followed by glucuronidation) accounted for 13% of the total plasma radioactivity. No active metabolites have been identified for upadacitinib.
Elimination: Following single dose administration of [14C]-upadacitinib immediate-release solution, upadacitinib was eliminated predominantly as the unchanged parent substance in urine (24%) and faeces (38%). Approximately 34% of upadacitinib dose was excreted as metabolites. Upadacitinib mean terminal elimination half-life ranged from 9 to 14 hours.
Special populations: Renal impairment: Upadacitinib AUC was 18%, 33%, and 44% higher in subjects with mild (estimated glomerular filtration rate 60 to 89 mL/min/1.73 m2), moderate (estimated glomerular filtration rate 30 to 59 mL/min/1.73 m2), and severe (estimated glomerular filtration rate 15 to 29 mL/min/1.73 m2) renal impairment, respectively, compared to subjects with normal renal function. Upadacitinib Cmax was similar in subjects with normal and impaired renal function. Mild or moderate renal impairment has no clinically relevant effect on upadacitinib exposure following the 15 mg or 30 mg once daily dosing regimens. The recommended dose is 15 mg once daily for patients with severe renal impairment.
Hepatic impairment: Mild (Child-Pugh A) and moderate (Child-Pugh B) hepatic impairment has no clinically relevant effect on upadacitinib exposure. Upadacitinib AUC was 28% and 24% higher in subjects with mild and moderate hepatic impairment, respectively, compared to subjects with normal liver function. Upadacitinib Cmax was unchanged in subjects with mild hepatic impairment and 43% higher in subjects with moderate hepatic impairment compared to subjects with normal liver function. Upadacitinib was not studied in patients with severe (Child-Pugh C) hepatic impairment.
Paediatric population: The pharmacokinetics of upadacitinib have not yet been evaluated in a paediatric patients with rheumatoid arthritis and psoriatic arthritis (see Dosage & Administration). Upadacitinib pharmacokinetics and steady-state concentrations are similar for adults and adolescents 12 to 17 years of age with atopic dermatitis.
The pharmacokinetics of upadacitinib in paediatric patients (< 12 years of age) with atopic dermatitis have not been established.
Intrinsic factors: Age, sex, body weight, race, and ethnicity did not have a clinically meaningful effect on upadacitinib exposure. Upadacitinib pharmacokinetics are consistent between rheumatoid arthritis, psoriatic arthritis, atopic dermatitis and ankylosing spondylitis patients.
Toxicology: Preclinical safety data: Upadacitinib, at exposures (based on AUC) approximately 4 and 10 times the clinical dose of 15 mg and 2 and 5 times the clinical dose of 30 mg in male and female Sprague-Dawley rats, respectively, was not carcinogenic in a 2-year carcinogenicity study in Sprague-Dawley rats. Upadacitinib was not carcinogenic in a 26-week carcinogenicity study in CByB6F1-Tg(HRAS)2Jic transgenic mice.
Upadacitinib was not mutagenic or genotoxic based on the results of in vitro and in vivo tests for gene mutations and chromosomal aberrations.
Upadacitinib had no effect on fertility in male or female rats at exposures up to approximately 21 and 43 times the maximum recommended human dose (MRHD) of 30 mg in males and females, respectively, on an AUC basis in a fertility and early embryonic development study. Dose-related increases in foetal resorptions associated with post-implantation losses in this fertility study in rats were attributed to the developmental/teratogenic effects of upadacitinib. No adverse effects were observed at exposures below clinical exposure (based on AUC). Post-implantation losses were observed at exposures 11 times the clinical exposure at the MRHD of 30 mg (based on AUC).
In animal embryo-foetal development studies, upadacitinib was teratogenic in both rats and rabbits. Upadacitinib resulted in increases in skeletal malformations in rats at 1.6 and 0.8 times the clinical exposure (AUC-based) at the 15 and 30 mg (MRHD) doses, respectively. In rabbits an increased incidence of cardiovascular malformations was observed at 15 and 7.6 times the clinical exposure at the 15 and 30 mg doses (AUC-based), respectively. No developmental toxicity was observed at approximately 0.15 times (rat) and at similar exposure in rabbits as the exposures at the MRHD of 30 mg. In a pre- and post-natal development study in pregnant female rats, oral upadacitinib administration at exposures approximately 1.4 times the MRHD of 30 mg resulted in no maternal effects, no effects on parturition, lactation or maternal behaviour and no effects on the offspring.
Following administration of upadacitinib to lactating rats, the concentrations of upadacitinib in milk over time generally paralleled those in plasma, with approximately 30-fold higher exposure in milk relative to maternal plasma. Approximately 97% of upadacitinib-related material in milk was the parent molecule, upadacitinib.
Administration of upadacitinib to juvenile Sprague-Dawley rats (from postnatal day 15 to 63) resulted in exposures and pharmacologic effects on the lymphoid system similar to those observed in adult rats. No adverse findings were observed in juvenile rats at exposures (AUC) approximately 9.4 and 4.8 times the exposures at the clinical doses of 15 mg and 30 mg, respectively (based on exposures in adult RA patients).