


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of action: Galantamine, a tertiary alkaloid is a selective, competitive and reversible inhibitor of acetylcholinesterase. In addition, galantamine enhances the intrinsic action of acetylcholine on nicotinic receptors, probably through binding to an allosteric site of the receptor. As a consequence, an increased activity in the cholinergic system associated with improved cognitive function can be achieved in patients with dementia of the Alzheimer type.
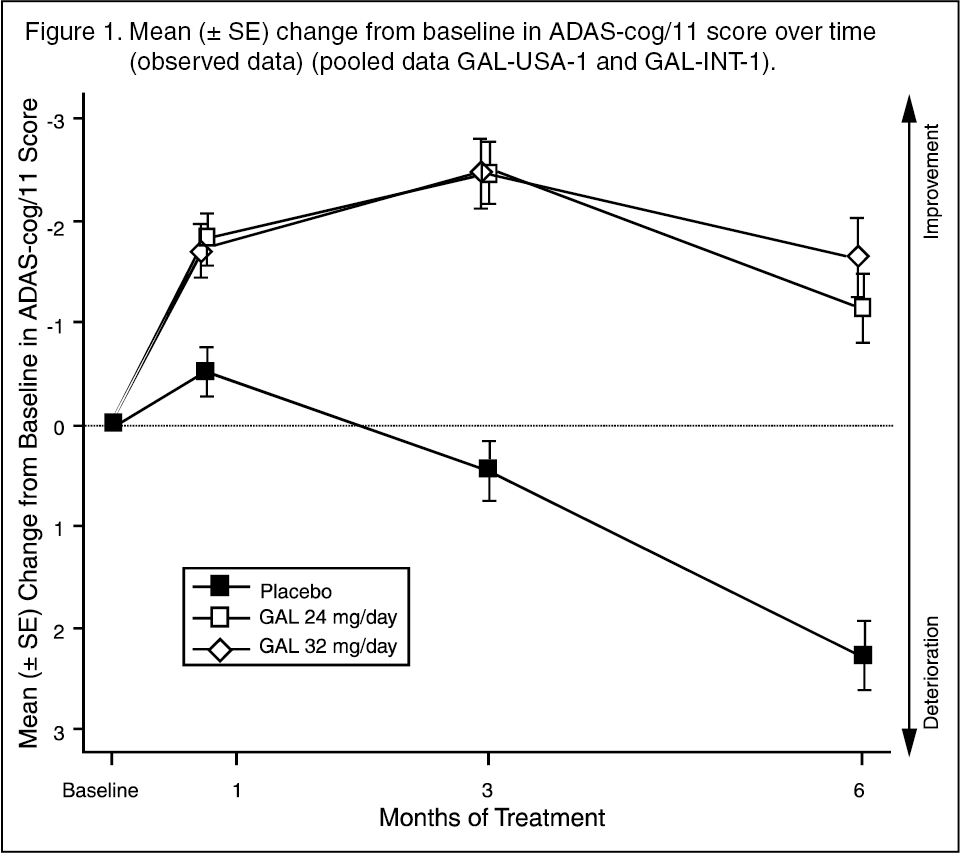
Clinical studies: The dosages of REMINYL shown to be effective in controlled clinical trials in Alzheimer's disease were 16, 24 and 32 mg/day. Of these doses, 16 and 24 mg/day were determined to have the best benefit/risk relationship and are the recommended doses. Galantamine's efficacy has been studied using four specific outcome measures: the ADAS-cog (a performance based measure of cognition), the CIBIC-plus (a global assessment by an independent physician based on a clinical interview with the patient and caregiver), several measurements of the activities of daily living and the Neuropsychiatric Inventory (NPI, a scale that measures behavioural disturbances).
In clinical studies, performance of galantamine treated patients on the ADAS-Cog (see Figure 1) and CIBIC-plus was consistently statistically significantly better than that of patients who were on placebo. Patients who were treated for 6 months with galantamine had ADAS-cog scores that were significantly improved compared to their baseline scores. Compared to the untreated patients there was a substantial and sustained benefit in cognitive functioning. Galantamine treatment also significantly preserved the activities of daily living, such as dressing, hygiene, meal preparation. These were assessed using the Disability Assessment in Dementia (the DAD) and the Alzheimer's Disease Cooperative Study (ADCS)-ADL-Inventory, caregiver-rated assessments. Galantamine doses of 16 and 24 mg daily maintained the NPI score throughout the observation period whereas the score of the placebo patients clearly deteriorated, as a result of the emergence of behavioural disturbances. (See Figure 1 and Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image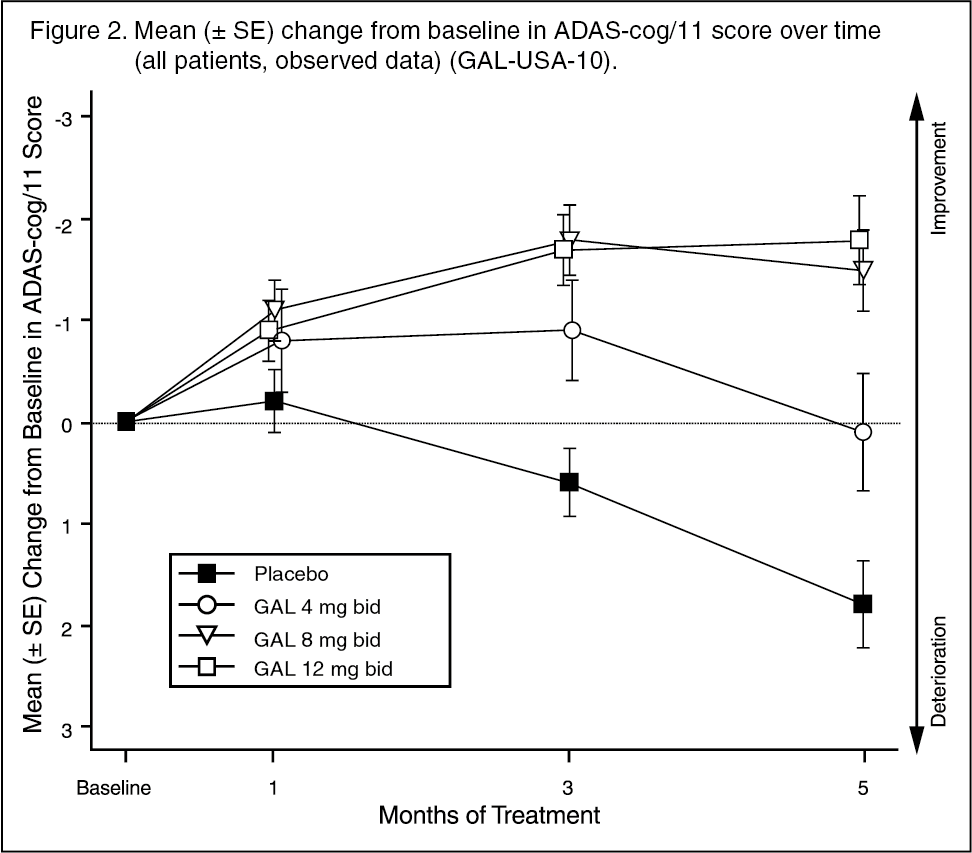 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLong-term treatment (combination of 6 months double-blind followed by 6 months open treatment) suggested that patients' cognitive and functional performance was maintained for a full year.
The efficacy of REMINYL prolonged release capsules was studied in a randomized, double-blind, placebo-controlled trial in Alzheimer's disease. Patients received galantamine 8 mg/day for 4 weeks, followed by galantamine 16 mg/day for 4 weeks. At week 8, the dose could be increased to 24 mg/day based on safety and tolerability, and could be reduced to 16 mg/day at week 12. The dose chosen at week 12 was fixed for the remainder of the 6 months. In the protocol-specified primary efficacy analysis for the two endpoints (ADAS-cog/11 and CIBIC-plus) at Month 6 simultaneously, REMINYL prolonged release showed a statistically significant improvement over placebo for ADAS-cog/11 only. In addition, REMINYL prolonged release was statistically significantly better than placebo in improving activities of daily living (ADCS-ADL), a key secondary efficacy measure. Efficacy results were similar for REMINYL prolonged release capsules and REMINYL tablets, which served as an active control in this study.
Long-term (2 year) efficacy and safety in mild to moderately severe Alzheimer's disease: A randomized, double-blind, placebo-controlled, parallel group, multi-center study evaluated the long-term (2-year) efficacy and safety of galantamine prolonged release capsules in the treatment of patients with mild to moderately-severe Alzheimer's disease. One thousand and twenty three patients were randomized to the placebo group, and 1028 to the galantamine group. Demographic and baseline characteristics were similar between the groups. The majority of patients were female (65%) and white (99.9%). The median age was 74 years, and baseline Mini-Mental State Examination (MMSE) score was 19.
On the primary efficacy endpoint (defined as change from baseline in the MMSE score at Month 24), there was a significantly less cognitive impairment in the galantamine group compared with placebo in the change from baseline in MMSE at Month 24 (-1.41 versus -2.14; p<0.001). On the key secondary efficacy endpoints (defined as change in MMSE at Month 6 and change in DAD score at Month 24), there was significantly greater improvement in change from baseline in MMSE at Month 6 in the galantamine group compared with placebo (mean change of 0.15 versus -0.28; p<0.001) and significantly less impairment in the DAD score at Month 24 in the galantamine group compared to placebo (-8.2 versus -10.8; p=0.002).
On the primary safety endpoint (mortality), there was a total of 89 deaths; 56 (5.5%) deaths in the placebo group and 33 (3.2%) deaths in the galantamine group. This represents a significantly higher rate of death in the placebo group compared with galantamine [hazard ratio and 95% confidence intervals of 0.58 (0.37 – 0.89) (p=0.011)].
Alzheimer's disease with cerebrovascular disease (AD+CVD): The efficacy and safety of galantamine in subjects with Alzheimer's disease and significant cerebrovascular disease (AD+CVD) was investigated in a double-blind, placebo-controlled study. There were 282 subjects, 48% of the total study population (N=592), who met criteria for AD+CVD. Although the clinical trial was not powered for subgroup analyses, galantamine-treated subjects experienced a statistically significant improvement, compared to placebo-treated subjects on both primary outcomes [(cognition: ADAS-cog/11 [p<0.001]; global clinical assessment: CIBIC-plus [p<0.001] and on a measure of activities of daily living (DAD [p=0.003]). Overall, the safety and tolerability of galantamine in subjects with AD+CVD was similar to that seen in previous studies of galantamine in Alzheimer's disease. The most frequently reported adverse event in subjects was nausea (19% of galantamine and 11% of placebo subjects). Other events, occurring in >5% of AD+CVD subjects and reported more frequently in the galantamine than the placebo group, were dizziness, vomiting, abdominal pain, diarrhea, and fatigue. The incidence of "cerebrovascular disorders" (e.g., stroke) was higher in the placebo group (placebo, 5/96 [5%] subjects; galantamine, 2/186 [1%] subjects).
Overall, the safety profile in AD+CVD was consistent with that observed in studies of galantamine in subjects with Alzheimer's disease.
Mild cognitive impairment (MCI): Two, 2-year controlled trials in subjects with MCI did not meet dual primary efficacy outcomes. Although mortality was low (0.7%), more deaths were initially recorded in subjects randomized to galantamine (13/1026) than to placebo (1/1022), but the incidence of serious adverse events was identical (19%) between treatment groups.
The 24-month intent-to-treat analysis recorded 20 deaths among subjects randomised to placebo compared to 34 deaths recorded among subjects randomised to galantamine (relative risk [95% CI] = 1.70 [1.00, 2.90]; p = 0.051. Of subjects who died within the protocol-specified period of 30 days of discontinuing double-blind study medication, there were 14 in the galantamine group and 3 in the placebo group (relative risk [95% CI] = 4.08 [1.57,10.57]; p = 0.004). Thirteen deaths in the placebo group and 20 deaths in the galantamine group were found to be directly related to adverse events that occurred while the subjects were exposed to double-blind study drug (relative risk [95% CI] = 1.54 (0.78, 3.04); p = 0.218.
More placebo-treated than galantamine-treated subjects discontinued prior to death, which may have accounted for the difference in mortality initially recorded. When data retrieved from the large proportion of patients in both treatment groups who discontinued prior to completion of the double-blind period (GAL-COG-3002) were included, a total of 102 deaths were identified, 56 in the galantamine group and 46 in the placebo group (relative risk [95% CI] = 1.24 [0.84,1.83]; p = 0.274).
The deaths were due to various causes that were not unexpected in an elderly population, with about half of the deaths in both groups were due to vascular causes.
Pharmacokinetics: Absorption: After oral intake of a single dose of 8 mg galantamine as tablets, absorption is rapid, with a peak plasma concentration of 43 ± 13 ng/ml, which is reached after 1.2 hours, and a mean AUC∞ of 427 ± 102 ng.h/ml. The absolute oral bioavailability of galantamine is 88.5%. Oral intake of galantamine tablets with food slows down its rate of absorption (Cmax reduced by about 25%), but does not affect the extent to which it is absorbed (AUC).
After repeated oral dosing of 12 mg galantamine twice a day as tablets, mean trough and peak plasma concentrations fluctuated between 30 and 90 ng/ml. The pharmacokinetics of galantamine are linear in the dose range 4-16 mg twice a day.
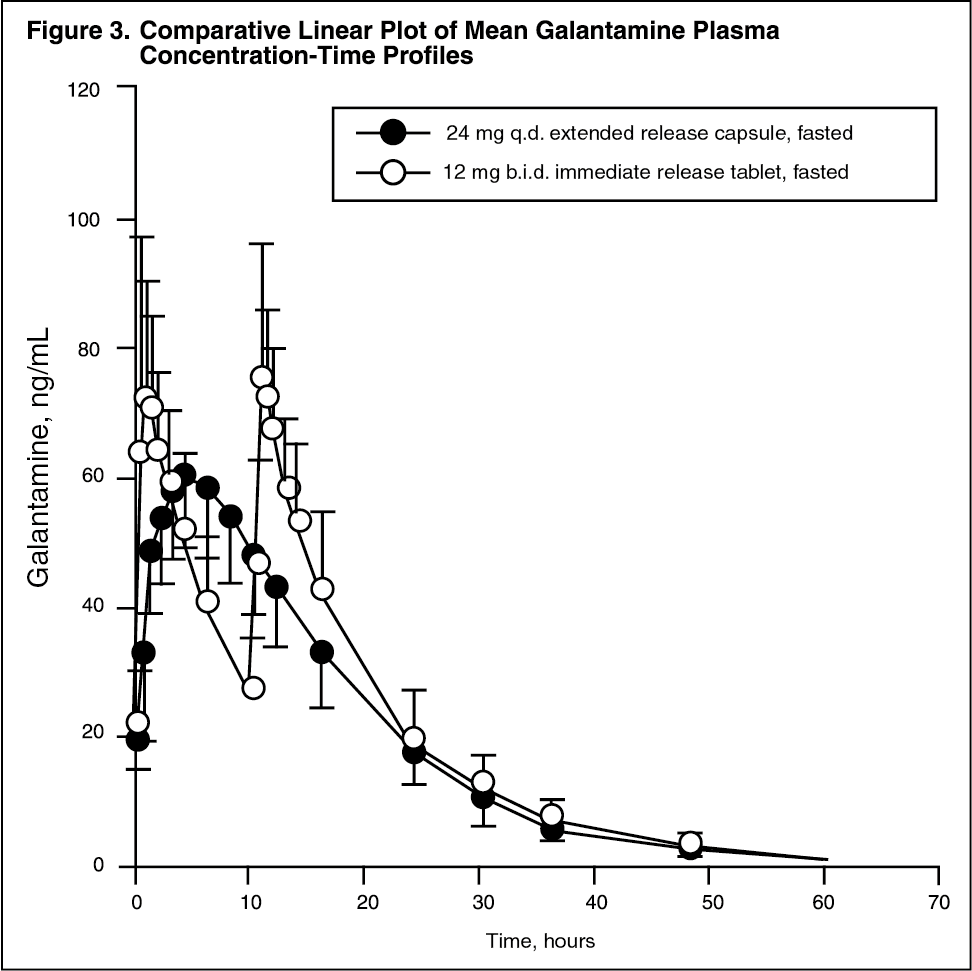
Bioavailability of immediate-release versus prolonged release formulations: In a steady-state bioavailability study, REMINYL prolonged release capsules, 24 mg once daily, were shown to be bioequivalent to the 12 mg twice-daily immediate release tablets with respect to AUC24h and Cmin. The Cmax value of the 24 mg once-daily prolonged release capsule, which is reached after 4.4 hours, was about 24% lower than that of the 12 mg twice-daily immediate release tablet. Food had no effect on the steady-state bioavailability of the 24 mg prolonged release capsules. In a dose-proportionality study of REMINYL prolonged release capsules in healthy elderly and younger adult subjects, steady-state plasma concentrations were achieved within 6 days at all doses (8 mg, 16 mg) in both age groups. Steady-state pharmacokinetics were dose proportional within the studied dose range of 8 mg to 24 mg in both age groups. (See Figure 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDistribution: Galantamine has a moderate volume of distribution (average Vdss of 175 l).
The plasma protein binding of galantamine is low: 17.7 ± 0.8%. In whole blood, galantamine is mainly distributed to blood cells (52.7%) and plasma water (39.0%), whereas the fraction of galantamine bound to plasma proteins in only 8.4%. The blood-to-plasma concentration ratio of galantamine is 1.17.
Metabolism: Major metabolic pathways were N-oxidation, N-demethylation, O-demethylation, glucuronidation and epimerization. O-demethylation was far more important in extensive metabolisers of CYP2D6. The levels of excretion of total radioactivity in urine and faeces were not different between poor and extensive metabolisers. In vitro studies confirmed that cytochrome P450 2D6 and 3A4 were the major cytochrome P450 isoenzymes involved in the metabolism of galantamine.
In plasma from poor and extensive metabolisers, unchanged galantamine and its glucuronide accounted for most of the sample radioactivity. In plasma from extensive metabolisers, the glucuronide of O-desmethylgalantamine was also important.
None of the active metabolites of galantamine (norgalantamine, O-desmethylgalantamine and O-desmethyl-norgalantamine) could be detected in their unconjugated form in plasma from poor or extensive metabolisers after single dosing. Norgalantamine was detectable in plasma from patients after multiple dosing, but did not represent more than 10% of the galantamine levels.
Elimination: Galantamine is a low-clearance drug (plasma clearance of approximately 300 ml/min). The elimination of galantamine is bi-exponential, with a terminal half-life in the order of 7-8 h.
Seven days after a single oral dose of 4 mg 3H-galantamine, 90-97% of the radioactivity was recovered in urine and 2.2-6.3% in the feces. After i.v. and oral administration, 18-22% of the dose was excreted as unchanged galantamine in the urine in 24 hours, with a renal clearance of about 65 ml/min, which represents 20-25% of the total plasma clearance.
Special Populations: Renal impairment: The disposition of galantamine was studied in young subjects with varying degrees of renal function. Elimination of galantamine decreased with decreasing creatinine clearance. Plasma concentrations of galantamine increased in subjects with impaired renal function by 38% in moderate (creatinine clearance=52-104 ml/min) or 67% in severe renal impairment (creatinine clearance=9-51 ml/min), compared to age and weight-matched healthy subjects (creatinine clearance=121 ml/min). A population pharmacokinetic analysis and simulations indicate that no dose-adjustments are needed in Alzheimer patients with renal impairment provided that the creatinine clearance is at least 9 ml/min (see Special populations under Dosage & Administration) as the galantamine clearance is lower in the Alzheimer population.
Hepatic impairment: The pharmacokinetics of galantamine in subjects with mild hepatic impairment (Child-Pugh score of 5-6) were comparable to those in healthy subjects. In patients with moderate hepatic impairment (Child-Pugh score of 7-9), AUC and half-life of galantamine were increased by about 30% (see Special populations under Dosage & Administration).
Characteristics in patients with Alzheimer's disease: Data from clinical trials in patients indicate that the plasma concentrations of galantamine in patients with Alzheimer's disease are 30-40% higher than in healthy young subjects.
Toxicology: NON-CLINICAL INFORMATION: All other preclinical safety data relevant to the prescriber have been included in the appropriate sections.